Accessibility and quality of medical service in the context of health care modernization

Author: Kalashnikov Konstantin Nikolaevich, Kalachikova Olga Nikolaevna
Journal: Economic and Social Changes: Facts, Trends, Forecast @volnc-esc-en
Section: Social development
Article in issue: 2 (32) т.7, 2014.
Free access
Assessment of access to health care is a complicated scientific and practical problem. The solution can not be limited to formal indicators of state and departmental statistics. Existing solely for the purpose to preserve the citizens’ health, the health care system must be based and reconstructed on the opinion of its customers, the territory’s residents who receive medical services under the state guarantees program. That is why, the necessary, if not the most important, component to assess the health care access is sociological data analysis. The Institute of Socio-Economic Development of Territories of the Russian Academy of Sciences has carried out the measurement and analysis of the Vologda Oblast population’s estimates of the access to medical services and its quality, provided by regional health institutions. This study is especially important because a number of reforms and the Program of Health Care Modernization have been implemented in the Russian health care over the last years. The authors have found out that the reforms improved the provision of the medical institutions with equipment, but the problem of staff shortage was not solved. What is more, the region’s residents are still concerned about ethics violations, medical workers’ rude behavior and difficulty to make an appointment at the doctor’s. These problems remain acute.
Health care modernization, medical aid, access to medical services and its quality, sociological research, vologda oblast
Short address: https://sciup.org/147223569
IDR: 147223569 | UDC: 614.2(470.12) | DOI: 10.15838/esc/2014.2.32.10
Text of the scientific article Accessibility and quality of medical service in the context of health care modernization
Since the early 2000s the Russian health care has undergone a number of modernization reforms, which today, after almost 15 years, should be given at least an interim evaluation. The content of the activities and the declared objectives sound clear and theoretically true: increasing the effectiveness of health care and providing the population with accessible medical care. The mechanisms to achieve this goal are consequent and quite reasonable. Particularly, it is a shift of emphasis from secondary health care, which is well developed in Russia [7], but does not justify its scale, to the primary link with its strategic advantages, such as early diagnosis and prevention, introduction of advanced methods to pay for medical care, changing the medical personnel payment system, when their efforts are taken into account.
However, most citizens, facing health care problems in everyday life, apprehend only strategic objective of expanding the access to medical care, and judge about its achievement by experience. The traditional problems of Russian health care, such as queues, disrespectful and uncaring attitude of health workers, increasing payment for medical services, insufficient provision of medicines, still retain and do not satisfy people.
Let us consider an example. Even the relatively prosperous 2000s experienced reduction in the amount of bedspace, which began in the 1990s crisis. In 2007 the formal method to estimate the Executive bodies’ performance was approved, according to which the reduction of places at day-night hospitals was regarded as a sign of the effective public spending1. The compensatory measures were not taken. As a result, in 2000–2012 the provision with hospital beds declined in the Russian Federation (by 27%), in the Northwestern Federal district regions (by 25% in total) and in the Vologda Oblast (by 28%). The given reduction is unlikely to contribute to the expansion of access to medical services.
The Program of Health Care Modernization, implemented in 2011–2012, was looked to, as its 5 billion budget is very significant for the region. In the conditions of deficit financing, the implementation of target programs becomes the only opportunity to enlarge medical institutions’ resources, at least in some territories.
The article, on the basis of a sociological survey of the Vologda Oblast population, considers how these processes influence the population’s assessment of the access to and quality of medical care2.
When starting a substantial part of the ar-ticle, let us focus on the citizens’ assessment of their own role in maintaining health, which is especially important in modern conditions, when a person’s own life is becoming the main arena of the struggle for human health [6]. Over a relatively short period of 2005–2013 the population’s consciousness has changed in the Vologda Oblast: particularly, people have become increasingly aware of their responsibility for health. Thus, if in 2005, 73% of the population considered themselves partly or fully responsible for their own health, in 2013 this indicator increased to 88%. At the same time, there decreased the proportion of citizens, who lay this responsibility on health workers (from 23% in 2005 to 14% in 2013), relatives and family members (from 9% to 3%). There is a significant reduction (from 25% in 2005 to 7% in 2013) in the proportion of people who consider the state to be responsible for their health. Indirectly this fact reflects the growth of civil consciousness and the expand of society atomization process [1]. The regional researches reveal the same [6].
On the background of the changing patterns of health factors [10] the person’s role in its preservation and strengthening is growing. However, this should not depreciate the importance of health care and medicine. These two subjects’ effective cooperation in matters of health preservation and life prolongation is critical nowadays. Medical activity is a manifestation of self-preservation behavior, way of life [3]. Therefore, the prevention and timely use of the qualified medical care remain the important aspects of health preservation.
As a rule, people visit a doctor in the period when they are ill. Another significant reason to visit medical institutions is periodic health examination. The 2013 survey indicates that 44% of the population visited a hospitable because of poor health for the last 12 months;
21% – for periodic health examination, 17% – for diseases prevention ( tab. 1 ). According to the 2013 data, 13% of the population selfmedicated. A quarter of the population noted that in the past year they had not had a sick-leave certificate, 22% – missed work days due to sickness and disease.
The measured level of the access to medical care in 2011–2013 remained almost unchanged: 77% of the region residents were more or less satisfied with the provision of medical services. The sum of low values (22% for the region as a whole) exceeds the sum of high values (14%). The most popular value is “satisfactory” (63% of the population) (tab. 2) .
The assessment of rural and urban residents do not differ significantly, however, the villagers are less inclined to describe the access to health care as high than citizens (8% of the estimates in municipalities against 18% – in Vologda and 13% – in Cherepovets).
Table 1. Distribution of answers to the question: “Why have you made an appointment with a doctor for the last 12 months?” (as a percentage of the number of respondents)
|
Answers |
Vologda |
Cherepovets |
Districts |
Oblast |
|
For prevention |
45.5 |
46.5 |
42.5 |
44.3 |
|
In the period when I was ill |
17.1 |
21.2 |
23.1 |
21.1 |
|
For periodic health examination |
16.6 |
12.8 |
18.8 |
16.7 |
|
I don’t remember |
3.6 |
4.6 |
9.9 |
6.9 |
|
I have not seen a doctor because I have self-medicated |
16.4 |
16.1 |
8.4 |
12.5 |
|
I have not seen a doctor because I have not been ill |
10.6 |
11.0 |
10.5 |
10.7 |
|
Source: data of ISEDT RAS sociological research in 2013. |
Table 2. Distribution of answers to the question: “Please, estimate the overall level of the access to health care (in % of respondents number)
|
Answers |
Vologda |
Cherepovets |
Districts |
Oblast |
|
High |
4.2 |
0.5 |
1.9 |
2.1 |
|
Quite high |
17.9 |
13.0 |
8.3 |
12.0 |
|
Satisfactory |
54.8 |
66.5 |
65.2 |
62.9 |
|
Rather low |
15.8 |
12.3 |
14.6 |
14.3 |
|
Low |
5.5 |
5.9 |
8.8 |
7.2 |
|
Medical services are not available |
1.0 |
0.5 |
0.4 |
0.6 |
|
Source: data of ISEDT RAS sociological research in 2013. |
||||
The analyzed correlation between demographic characteristics of the population and the assessment of access to health care has not revealed any special features: there are both positive and negative estimates among men and women, aged from 30 to 60–55.
The retrospective review of medical institutions for the period of the Modernization Program shows that the traditional problems have remained acute, but the year of 2013, compared to previous years, witnessed a noticeable improvement in all considered aspects, except for “the lack of necessary professionals”. Till 2010 more than half of the region inhabitants marked long queues at medical institutions and the inability to make an appointment at the doctor’s at a convenient time, in 2012 and 2013 their number decreased significantly (up to 50% and 36%, respectively) (tab. 3) . The lack of necessary professionals was a problem for 34% of the population in 2012 and 42% in 2013. People do not like doctors’ rude behavior (18% in 2012, and 13% in 2013), their carelessness (24% and 16%, respectively) and ongoing commercialization of health care (17 and 14%).
The respondents, highly assessing the accessibility and quality of medical services, agree with the presence of the mentioned problems, especially with those of doctors’ disrespectful attitude and payment for medical care.
Drawing attention to the fact that the most common problem for the region’s population is still the difficulty to arrange a visit to a doctor at a convenient time, it should be noted that the information technology plays its role in enhancing the access to health care. People, highly assessing this role, use electronic terminals (infomats) to make an appointment at the doctor’s by 4.5 times more likely than the dissatisfied with the present level of medical services access. This demonstrates the prospects of electronic devices and the Internet in boosting the efficiency of medical service provision.
However, today the practical role of information technologies is insignificant. The absolute majority of residents (82%) do not use the infomats for this purpose and slightly more than half know about their existence (at the time of publishing the article there are 37 infomats in the region). What is more, 62% of the respondents are unable to arrange a visit to a doctor via the Internet. The given research does not study the causes, but there is no doubt that the reasons are not only people’s low level of digital literacy, but also usual conservatism and habits. Moreover, the opportunities of “electronic reception” will not be able to solve the problem of the access to health care without proper staffing in hospitals.
Table 3. Negative phenomena in the medical institutions’ activities in the Vologda Oblast (% of the number citizens who have attended hospitals and opted such answers as “it satisfies partially”, “it does not satisfy in many cases”, “it does not satisfy at all”)
|
Negative phenomenon |
2002–2006 |
2008 |
2010 |
2012 |
2013 |
|
Inability to get an appointment at a convenient time, long queues |
58.1 |
56.7 |
59.4 |
49.7 |
35.8 |
|
Lack of necessary professionals |
- |
24.9 |
34.8 |
34.3 |
41.6 |
|
Negligent attitude of health workers |
- |
18.0 |
24.2 |
23.5 |
15.5 |
|
Rudeness, disrespect to patients |
15.2 |
11.5 |
12.5 |
18.3 |
12.5 |
|
Lack of information on the specialists’ work |
21.0 |
14.7 |
23.5 |
18.2 |
|
|
Need to pay for medical services, |
16.9 |
9.9 |
14.5 |
17.2 |
13.7 |
|
Source: data of ISEDT RAS sociological research in 2013. |
|||||
However, there is some correlation between the use of registration terminals and the Internet for an appointment to see a doctor and key demographic characteristics of the population (tab. 4) . Older people are often not aware of the availability of electronic registration and do not use them.
Women of young and middle age groups use electronic technology more active than men of similar ages. For example, the sum of answers to the question about the availability of “electronic reception” shows that the ratio of answers “Yes” and “No” for men of 30–60 is 24 and 28%, respectively, for women – 28% and 18%.
The significant number of settlements with small population, dispersed over a wide area, and poor infrastructure make the issue of medical institutions’ territorial and transport accessibility very relevant.
Contrary to the expectations, the way to the nearest medical institution takes slightly more time for villagers than for citizens. The only significant difference in terms of “cityvillage” arises when the time to get to place of destination takes “more than two hours”: this option is marked by 7% of rural residents and by 1–2% of urban residents ( tab. 5 ).
As for the public transport quality, the difference between villages and big cities is more visible: it is bad for 17% of the rural population, 5% for people in Vologda and 2% for people in Cherepovets. The residents of Cherepovets estimate the availability of public transport much more highly than the residents of the regional capital, but this problem refers
Table 4. Age and gender characteristics of the population and “electronic reception” (as a percentage of the number of respondents)
|
Socio-demographic characteristics of respondent |
Do you know that you can use electronic devices (infomats) via the Internet to make an appointment with a doctor? |
Do you have an opportunity to make an appointment with a doctor via the Internet? |
Do you use electronic terminals (infomats) to make an appointment with a doctor? |
|||
|
Yes |
No |
Yes |
No |
Yes |
No |
|
|
Sex/age |
||||||
|
Men up to 30 |
12.1 |
10.4 |
12.5 |
10.6 |
11.7 |
11.3 |
|
of 30–60 |
24.2 |
27.8 |
26.1 |
25.5 |
22.3 |
26.3 |
|
over 60 |
5.4 |
10.6 |
4.7 |
9.6 |
5.9 |
8.1 |
|
Women up to 30 years |
14.8 |
6.4 |
17.2 |
7.5 |
17.6 |
9.8 |
|
of 30–55 |
27.8 |
18.2 |
30.4 |
19.5 |
33.2 |
21.6 |
|
over 55 |
15.8 |
26.6 |
9.1 |
27.3 |
9.4 |
23.0 |
|
Source: data of ISEDT RAS sociological research in 2013. |
||||||
Table 5. Distribution of answers to the question: “How much time does it takes you to get to the nearest doctor/medical assistant or hospitable?” (as a percentage of the number of respondents)
The access to health care is also characterized by the payment for the services, which role will increase with the growing commercialization of health care. Among people, expressing dissatisfaction with the existing level of medical services availability, 14% have indicated the need to pay for health services
(tab. 7) . The prevalence of commercial practices in the field of public health is demonstrated by the significant proportion of people (44%), who have paid for treatment in the current year (37% of urban inhabitants have not spent money on treatment)3.
The access to medical treatment is considered as low more often by those people who have paid for them (26% against 41%; tab. 8) .
Table 6. Distribution of answers to the question: “How does the public transport, you use, work?” (as a percentage of the number of respondents)
|
Answers |
Vologda |
Cherepovets |
Districts |
Oblast |
|
Good in general |
26.8 |
40.4 |
7.2 |
20.9 |
|
Rather good |
36.9 |
43.0 |
30.1 |
35.2 |
|
Rather bad |
16.4 |
5.6 |
17.7 |
14.2 |
|
Bad |
4.9 |
2.3 |
16.6 |
9.9 |
|
I do not know |
15.1 |
8.7 |
28.5 |
19.9 |
|
Source: data of ISEDT RAS sociological research in 2013. |
||||
Table 7. Distribution of answers to the question: “Have you spent money on treatment at a medical institution this year?” (as a percentage of the number of respondents)
|
Answers |
Vologda |
Cherepovets |
Districts |
Oblast |
|
Yes, monthly |
11.2 |
7.4 |
5.9 |
7.7 |
|
Yes, once in three months |
16.1 |
10.2 |
6.9 |
10.1 |
|
Yes, once in six months |
15.8 |
13.6 |
13.0 |
13.9 |
|
Yes, once a year |
15.3 |
21.0 |
6.5 |
12.5 |
|
No, I have not |
23.9 |
36.6 |
44.2 |
37.0 |
|
No, I have not, because I have not been ill |
16.4 |
10.5 |
21.3 |
17.2 |
|
Source: data of ISEDT RAS sociological research in 2013. |
||||
Table 8. Age and gender characteristics of the population and assessment of the access to medical services (as a percentage of the number of respondents)
|
Have you spent money for treatment at a medical institution this year? |
How do you assess the level of access to health care? |
||
|
High |
Satisfactory |
Low |
|
|
Yes, monthly |
8.5 |
7.1 |
8.7 |
|
Yes, once in three months |
12.7 |
8.8 |
12.0 |
|
Yes, once in six months |
11.8 |
15.1 |
12.3 |
|
Yes, once a year |
7.5 |
12.5 |
16.0 |
|
No, I have not |
41.0 |
39.4 |
26.2 |
|
No, I have not, because I have not been ill |
17.9 |
15.7 |
21.7 |
|
Source: data of ISEDT RAS sociological research in 2013 |
|||
3 The question wording should be clarified and the costs should not include money, spent by an outpatient on the purchase of medicine.
Seventy five percent of the region’s population has noticed that most payments for treatment are formal. There is a small amount of informal payments. However, 28% of the population has spent their own money to pay for treatment procedure, 7% – on medicaments, when having inpatient treatment ( tab. 9 ).
The dynamics of the population’ estimates of the access to health care is interesting. Since 2003 there has been a tendency of decrease in the share of respondents who consider that the access to health services has not changed for the last 12 months.
The share of the region’s residents, marking negative tendencies in the sphere of medical services accessibility, is not stable. The increase in the number of dissatisfied with the changes was recorded in 2005–2006. After the sharp rise up to 28% in 2010 this indicator started to decline, reaching 12% by 2013. The share of positive estimations is not stable as well; however since 2007 it is decreasing. So, in 2013 only 8% of the population has appreciated the change in the access to health services ( fig .).
The medical care quality is another critical characteristic for the population. The sociological survey data are not the most reliable method to assess the quality of medical care for several reasons. There is information asymmetry between medical workers and patients that prevents objective perception of the quality parameters of medical services. The ability to achieve the high-qualitied medical services is limited by public guarantees and financial possibilities of the state [2, 4]. Thus, the quality standards are the result of a compromise between theoretically correct ideas of humanism and recognition of the patient’s interests as a supreme value and limited resources of budgets and extra-budgetary funds for their provision.
The most acceptable way to mitigate information asymmetry in the framework of this organizational model is standardization of medical assistance. However, in this case the patient’s notion about a proper (or desired) level of health services quality can differ from formal regulations. Moreover, taking into account the phenomenon of asymmetric information, it is logical to assume that patients consider medical care quality as effectiveness of disease control, as well as conditions of its provision, including a wide range of measurable moments (for example, professional culture of the medical staff, cleanliness of a sick room, etc.). Despite these circumstances, we can say that the assessment of medical care quality is one of the informative indicators of efficiency of medical institutions’ activity, reflecting the current situation and the problematic aspects that require attention and interference.
The Vologda Oblast population’s estimates of the health services quality have undergone significant changes during implementation of the Modernization Program. In 2011 78% of the population was more or less satisfied with the medical services quality, in 2013 the figure rose to 82%.
Table 9. Distribution of answers to the question: “When paying for treatment at a hospital, you pay the money... (as a percentage of those who have spent money on treatment this year)
|
Answers |
Vologda |
Cherepovets |
Districts |
Oblast |
|
To a pay desk of the medical institution |
70.2 |
87.7 |
69.2 |
75.3 |
|
To a head of the medical institution |
3.1 |
0.5 |
0.0 |
1.2 |
|
To a doctor |
7.1 |
4.9 |
3.0 |
5.0 |
|
To a medical personnel (a nurse, a medical assistant) |
3.1 |
2.5 |
2.6 |
2.7 |
|
To a hospital attendant |
1.3 |
2.9 |
0.0 |
1.4 |
|
Source: data of ISEDT RAS sociological research in 2013. |
||||
Distribution of answers to the question: “Have you noticed any change in the access to health services over the past 12 months?” (in % of those who have sought medical help)
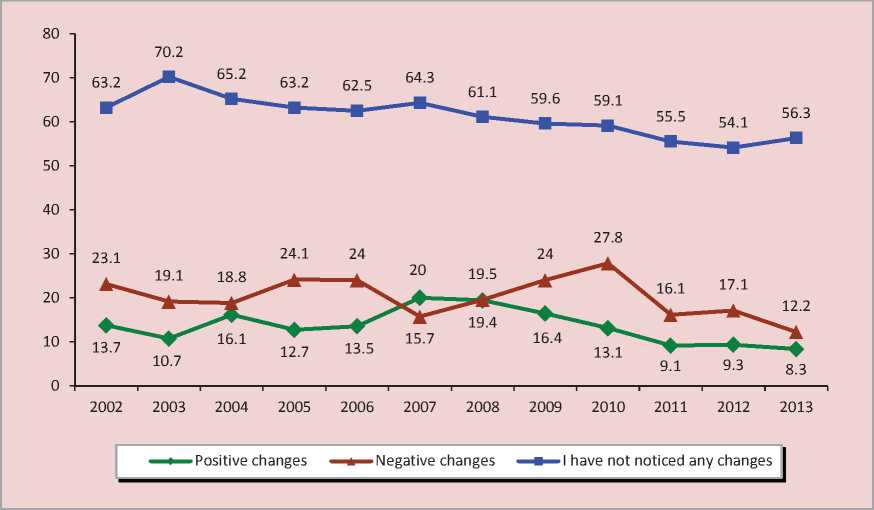
Source: ISEDT RAS data.
The sum of the highest ratings (18% for the region as a whole) is close to the sum of low estimates (17%). The most common is a “satisfactory” estimate: 64% of the Vologda Oblast population has such point of view ( tab. 10 ).
The difference in assessments of health care quality between big cities and municipal districts is that rural residents are less likely to give high marks than residents of Vologda and Cherepovets, however, this difference is redistributed with the answer variant “satisfactory”.
The connection between age and gender characteristics and estimation of medical aid quality is reflected in the fact that older people have negative assessments more often.
The ratio of the availability and quality of medical care is an interesting question. Foreign researches, first of all inter-country ones, concerning a comparative analysis of different public health systems, often view the gap between availability and quality of medical services as the specification of the health protection models. Let us consider the results of the study, conducted by the Gallup University in America. It is based on telephone interviews of the population in Canada, the US and the UK. In Canada satisfaction with the access to health care (57%) is slightly higher than satisfaction with the quality (52%); in the UK where there is also a high share of public resources in health care, satisfaction with accessibility and quality of medical care is lower, but the population’s estimates do not differ practically (43% and 42%, respectively). The US residents, where health care is based on paid services and there is not a universal health insurance system, estimate the access to expensive health services as very low (only 25% of the Americans is satisfied with the medical care availability), but the quality is not highly valued as well (only 48% is satisfied with the quality) [11].
Table 11. Distribution of answers to the question: “How do you assess the quality of medical care?”
|
How do you assess the medical services quality? |
How do you assess the access to medical services? |
||
|
High |
Satisfactory |
Low |
|
|
Very good |
8.5 |
0.2 |
0.6 |
|
Rather good |
51.7 |
13.8 |
4.0 |
|
Satisfactory |
37.0 |
77.5 |
45.4 |
|
Bad |
2.8 |
7.9 |
44.2 |
|
Very bad |
0.0 |
0.5 |
5.8 |
|
Source: data of ISEDT RAS sociological research in 2013 |
|||
According to the results of our study, the Vologda Oblast population assesses the quality and access in a unified manner. The respondents, highly evaluating the access to health services, practically do not estimate the quality negatively (there are no answers “very bad”, the share of answers “bad” is insignificant (3%), while the total share of answers “good” and “fairly good” reaches 60%). On the contrary, among the people, dissatisfied with the current level of access to health care, at least half of them have negative assessments of its quality (tab. 11) . One can suppose that people do not differentiate the notions “access” and “quality” of medical services, a priori assuming that a qualified specialist, working in this sphere, does his/her best.
There is correlation between the estimates of quality and services payment. Among those who do not use paid medical services, the proportion of low estimates of their quality is higher, compared to those who pay for health services (37% against 26%).
It should be recognized that the assessment of medical care quality is highly subjective and can not reflect real changes in the medical institutions’ activities. The study of the access to medical services is always more objective in this respect. However, ignoring people’s estimate of medical care quality can be a big mistake.
Thus, the population’s responses to questions about the quality and access to local health services do not contain univocal assessment of the current health care or the Modernization Program results. On the one hand, directly or indirectly the population’s opinions point to the deep structural problems and negative private practice, for many years hampering the increase in access to health care. But, on the other hand, one cannot but notice positive changes in a number of activities and citizens’ loyalty to the Russian healthcare system in general.
Although most people are satisfied with the access to and quality of medical assistance, just a small number of them appreciate it highly. The population is concerned of difficulties to arrange to see a doctor, lack of specialists, rude and careless attitude of medical workers and difficult access to many medical services.
It is known that the patients’ characteristic to expect health services of a high level and neglect their success is an objective fact of social life throughout the world, however, it should not become the reason to ignore the citizens’ collective opinion that the national health care system has a number of problems that limit the accessibility and quality of medical services and are still far from being solved.
References Accessibility and quality of medical service in the context of health care modernization
- Balatsky E.V. Zakonomernosti i paradoksy sotsial’noi evolyutsii . Obshchestvennye nauki i sovremennost’ , 2013, no.2, pp. 138-150
- Duganov M.D., Kalashnikov K.N. Metodologicheskie podkhody k otsenke effektivnosti regional’nogo zdravookhraneniya . Ekonomicheskie i sotsial’nye peremeny: fakty, tendentsii, prognoz , 2011, no.6, pp. 93-105.
- Kalachikova O.N., Korchagina P.S. Osnovnye tendentsii samosokhranitel’nogo povedeniya naseleniya regiona . Problemy razvitiya territorii , Vologda: ISERT RAN, 2012, no.5(61), pp. 72-82.
- Kalashnikov K.N., Kondakova N.A. Rezul’tativnost’ programmy modernizatsii zdravookhraneniya: otsenki patsientov i vrachei . Zdravookhranenie , 2014, no.2, pp. 28-38.
- Lastochkina M.A. Sotsial’naya zashchishchennost’ naseleniya Rossii: obzor issledovanii poslednikh let . Ekonomicheskie i sotsial’nye peremeny: fakty, tendentsii, prognoz , 2013, no.2, pp. 171-179.
- Pervichnaya mediko-sanitarnaya pomoshch’ segodnya aktual’nee, chem kogda-libo: doklad o sostoyanii zdravookhraneniya v mire, 2008 g . Geneva: VOZ, 2008. 152 p.
- Figeras Zh., Makki M., Mossialos E. et. al. Reforma bol’nits v novoi Evrope . Translated from English, Moscow: Ves’ mir, 2002, 320 p.
- Semenova V.G. Obratnyi epidemiologicheskii perekhod v Rossii . Moscow: TsSP, 2005. 235 p.
- Shabunova A.A., Kalashnikov K.N., Kalachikova O.N. Obshchestvennoe zdorov’e i zdravookhranenie territorii . Supervised by A.A. Shabunova. Vologda: ISERT RAN, 2010. 284 p.
- Shilova L.S. Resursy modernizatsii zdravookhraneniya. . GosBuk . Available at: http://www.gosbook.ru/node/65985
- Blizzard R. Healthcare System Ratings: U.S., Great Britain, Canada. Gallup. Available at: http://www.gallup.com/poll/8056/healthcare-system-ratings-us-great-britain-canada.aspx
