Atrial fibrillation in patients with chronic obstructive pulmonary disease in Eastern Afghanistan

Author: Shams A., Ahmadzai H., Ibrahimi I., Shams S.Ja.
Journal: Международный журнал гуманитарных и естественных наук @intjournal
Section: Медицинские науки
Article in issue: 2-1 (89), 2024.
Free access
Chronic obstructive pulmonary disease is the leading respiratory disease which not only bears complications in the lungs but also in other systems of the body including heart which for example complicates to atrial fibrillation. The aim of the study was to investigate the incidences of atrial fibrillation in patients with chronic obstructive pulmonary disease. It was a retrospective cross sectional study conducted on the data of two years from patients admitted under the diagnosis of chronic obstructive pulmonary disease in multiple centers in Nangarhar. The study included both male and female patients aging 18 years and over based on purposive sampling. The study included 296 patients of whom 158 (53.6%) were males and 138 (44.4%) were females. Mean age of the study population was 59.5±11.6 years. 51 out of 296 (17.2%) patients had atrial fibrillation: 26 (16.3%) males and 25 (18.1%) females. There was no case in age group 18-28 years but increased further on such as 3 cases (5.9%) in 29-39 years, 5 (9.8%) cases in 40-49 years, 14 (27.5%) cases in 50-59 years, and 27 (56.8%) cases in age group 60 and over. Atrial fibrillation was more prevalent in smokers 27 (20.3%) compared to non-smokers 14 (14.1%). Mean pulse deficit across atrial fibrillation patients was 23 ± 7 beats per minute. Atrial fibrillation was more prevalent in patients with chronic obstructive pulmonary disease especially in females, old age, smokers, and physically inactive patients. Awareness programs should be designed to early detect cases and precision should be made in selecting medicine for chronic obstructive lung disease taking atrial fibrillation into consideration.
Atrial fibrillation, arrhythmia, copd, chronic bronchitis, emphysema
Short address: https://sciup.org/170203811
IDR: 170203811 | DOI: 10.24412/2500-1000-2024-2-1-60-64
Фибрилляция предсердий у пациентов с хронической обструктивной болезнью легких в Восточном Афганистане
Хроническая обструктивная болезнь легких является ведущим респираторным заболеванием, которое вызывает осложнения не только в легких, но и в других системах организма, включая сердце, что, например, приводит к фибрилляции предсердий. Целью исследования было изучение частоты возникновения фибрилляции предсердий у пациентов с хронической обструктивной болезнью легких. Это было ретроспективное перекрестное исследование, проведенное на основе данных за два года от пациентов, поступивших с диагнозом хронической обструктивной болезни легких в несколько центров в Нангархаре. В исследование были включены пациенты мужского и женского пола в возрасте 18 лет и старше на основе целенаправленной выборки. В исследование были включены 296 пациентов, из которых 158 (53,6%) были мужчинами и 138 (44,4%) - женщинами. Средний возраст исследуемой популяции составил 59,5±11,6 лет. У 51 из 296 (17,2%) пациентов наблюдалась фибрилляция предсердий: у 26 (16,3%) мужчин и у 25 (18,1%) женщин. В возрастной группе 18-28 лет не было ни одного случая, но в дальнейшем число случаев увеличилось: 3 случая (5,9%) в возрасте 29-39 лет, 5 (9,8%) случаев в возрасте 40-49 лет, 14 (27,5%) случаев в возрасте 50-59 лет и 27 (56,8%) случаев в возрастной группе 60 лет и старше. Фибрилляция предсердий была более распространена у 27 курильщиков (20,3%) по сравнению с 14 некурящими (14,1%). Средний дефицит пульса у пациентов с фибрилляцией предсердий составил 23 ± 7 ударов в минуту. Фибрилляция предсердий чаще встречалась у пациентов с хронической обструктивной болезнью легких, особенно у женщин, пожилых людей, курильщиков и физически неактивных пациентов. Следует разработать программы повышения осведомленности для раннего выявления случаев, а также обеспечить точность при выборе лекарств от хронической обструктивной болезни легких с учетом фибрилляции предсердий.
Text of the scientific article Atrial fibrillation in patients with chronic obstructive pulmonary disease in Eastern Afghanistan
Chronic obstructive pulmonary disease (COPD) is the leading respiratory system disease known for airflow limitation to the lungs. In fact, the American Thoracic society included two diseases in the definition of COPD: Chronic bronchitis known for productive cough and emphysema known for chronic dyspnea due to terminal bronchiole alveolar dilatation and destruction (1). The overall prevalence of COPD is 10% worldwide (2) although criteria for its diagnosis varies. Global initiatives for lung disease (GOLD) defined COPD case by spirometry as the ratio of forced expiratory volume in one second divided by forced vital capacity less than 0.7 (1) though there is physiology variation in the aforementioned ration regarding age as being lower in old ages without disease and normal despite disease in young people (3). COPD not only bears complications in lungs but also in other parts of the body such as heart which for example causes atrial fibrillation (4). Responsible mechanisms for the development of atrial fibrillation in COPD patients include hypoxemia, hypercapnia, inflammation, aging, increased thoracic pressures (5) and medicines used for COPD such as beta agonists (6), steroids, anticholinergics (7), theophylline (8), and etc. Several scoring systems have been developed to predict prognosis in the comorbid COPD and atrial fibrillation patients including BODE index which stands for body mass index, airway obstruction, dyspnea scores and exercise. Literature has implicated mechanical changes in both right and left sides of the heart in the base of increased
BODE score (9). In fact, every five-millimeter increase in the diameter of left atrium increases atrial fibrillation incidences by 39% (10). In addition, Atrial fibrillation worsens COPD clinic specifically dyspnea and cyanosis.
Despite many researches on the topics, our hospitals still lack data on the incidences of atrial fibrillation in COPD patients so we aimed to conduct this study to find out the incidences of atrial fibrillation in COPD patients.
Methodology
It was a retrospective cross – sectional study conducted on the two years data of COPD patients at multiple centers in Nangarhar, Afghanistan including both male and female patients aging 18 years and over based on purposive sampling. Patients who had other causes of atrial fibrillation such as thyrotoxicosis, valvular heart disease, and etc. were excluded from the study.
COPD diagnosis was already made and written in the files based on GOLD criteria.
Data was collected through pre-structured questionnaire from the medical files of the patients after getting formal authorization. Patients’ identity was hidden for ethical purpose and medical record numbers were added instead.
Data was analyzed in SPSS (Statistical Program for Social Sciences). Mean ± standard deviation was used for continuous variables after data being check for normality through Kolmogorov-Smirnov test and frequencies and percentages were used for categorical variables.
Results
There were 296 patients with known diagnosis of COPD 158 (53.4%) of whom were males and the rest 138 (46.6%) were females. Table 1 Shows demographics of the study population.
Table 1. Demographic information of the study population
|
Parameters |
Frequency |
Percentage |
|
|
Gender |
Male |
158 |
53.4% |
|
Female |
138 |
46.6% |
|
|
Age Groups |
18-28 |
2 |
1% |
|
29-39 |
21 |
7% |
|
|
40-49 |
34 |
11% |
|
|
50-59 |
71 |
25% |
|
|
≥ 60 |
168 |
57% |
|
|
Job |
Jobless |
149 |
50.3% |
|
Shopkeepers |
68 |
23% |
|
|
Farmers |
26 |
8.8% |
|
|
Other jobs |
53 |
17.9% |
|
Mean age of the patients was and the rest of the descriptive statistics are shown in table 2.
Table 2. Descriptive statistics
|
Parameter |
Mean ± SD |
Minimum |
Maximum |
|
Age |
59.5 ± 11.6 |
34 |
105 |
|
Weight |
60 ± 13.6 |
33 |
95 |
|
Systolic BP |
120.5 ± 27.3 |
60 |
180 |
|
Diastolic BP |
101.1 ± 12.7 |
40 |
135 |
|
Heart rate |
104.5 ± 15.4 |
68 |
154 |
|
Oxygen saturation |
101.1 ± 12.7 |
68 |
96 |
In fact, only 51 out of 296 (17.2%) COPD patients had atrial fibrillation. The rest of the patients were in sinus rhythm as shown in figure 1.
CORD Patients
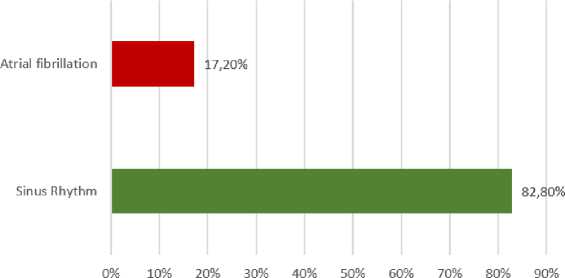
Figure 1. Atrial fibrillation in COPD patients
In addition, atrial fibrillation was more prevalent in females compared to males i.e. 25 (18.1%) versus 26 (16.3%).
Interestingly, atrial fibrillation cases in patients with chronic obstructive pulmonary disease increased with increasing age. In fact, we did not notice any atrial fibrillation case in the lowest age group, 18-28 years, however, more than half of the cases happened in the age group of 60 years and over as shown in table 3.
Table 3. Atrial fibrillation prevalence across age groups
|
Age groups (years) |
Sinus rhythm |
Atrial fibrillation |
|
18-28 |
2 (0.8%) |
0 (0%) |
|
29-39 |
18 (7.3%) |
3 (5.9%) |
|
40-49 |
29 (11.8%) |
5 (9.8%) |
|
50-59 |
57 (23.3%) |
14 (27.5%) |
|
>=60 |
139 (56.7%) |
29 (56.9%) |
|
Total |
245 (100%) |
51 (100%) |
Furthermore, atrial fibrillation prevalence was more in smokers (current smokers, past smokers or restarters) compared to those who had not ever smoked i.e. 20.3% versus 14.1%.
In addition, we found out atrial fibrillation across the findings of chest plain radiographs (chest X rays); atrial fibrillation was more prevalent in patients having dirty lungs and cardiomegaly respectively i.e. 66.7% and 43.1%.
Mean pulse deficit across atrial fibrillation was 23 ± 7 beats/minute.
Discussion
The major finding of the study revealed that atrial fibrillation was more prevalent in patients with chronic obstructive pulmonary disease (17.2%) being more prevalent in males compared to females. In fact, atrial fibrillation incidences increased with increasing age. It is because patients with advanced age have other risk factors for the develop- ment and maintenance of atrial fibrillation such as hypertension, atherosclerosis, and etc. Similarly, studies by Arya et al., Manuti et al., and Terzano et al. (11-13) demonstrated atrial fibrillation prevalence 9%, 8%, and 20.2% respectively in patients with chronic obstructive pulmonary disease. However, sample size in the studies by Arya et al. and Manuti et al., was very small, including around fifty patients. And Terzano included patients aging over 40 years. The aforementioned studies have also shown increased atrial fibrillation prevalence in females and in patients with advanced age. In fact, 52% of patients having atrial fibrillation were in the advanced age group in the study by Terzano (13).
More than half of the patients were smokers in our study; the interesting thing about smoking was that all smokers were male patients and we did not notice any female case. It is because females in country traditionally do not smoke or the hide their smoking habit because of the social values and personal dignity. However, smoke other than that of the tobacco such as dusts and smoke from combustion materials have been shown to increase COPD (14). In fact, smoking itself increases the incidence of atrial fibrillation (15).
According to x ray findings in patients with comorbid atrial fibrillation and chronic obstructive pulmonary disease, most patients had cardiomegaly. In fact, literature has shown that every 5-millimeter increase in the diameter of left atrium increases atrial fibrillation by 39% (10).
Despite the great findings of the study, there were a few limitations that might have affected the results some way. First, the study was retrospective and we could not have some variables from the patient files; for example, computed tomographic reports to know about the extent of lungs involvement and atrial fibrillation incidences. Second, we did not have Holter monitor so we may have missed some atrial fibrillation cases happening at time other than that for electrocardiogram. Otherwise, we may have had more than the current cases of atrial fibrillation.
Conclusion
Our study concluded that atrial fibrillation was more prevalent in patients with chronic obstructive pulmonary disease especially in females, old age, smokers, and physically inactive patients. Awareness programs should be designed to early detect cases and precision should be made in selecting medicine for chronic obstructive lung disease taking atrial fibrillation into consideration.
Acknowledgement
The authors express their warm gratitude to all the staff of hospitals in facilitating data collection.
References Atrial fibrillation in patients with chronic obstructive pulmonary disease in Eastern Afghanistan
- American Thoracic Society. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease // Am J Respir Crit Care Med. - 1995. - № 152. - P. 78-3.
- Buist A.S., McBurnie M.A., Vollmer W.M., Gillespie S., Burney P., Mannino D.M.,.. & Nizankowska-Mogilnicka, E.International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study // The Lancet. - 2007. - № 370(9589). - P. 741-750.
- Chapman K.R., Mannino D.M., Soriano J.B., Vermeire P.A., Buist A.S., Thun M.J.,.. & Beasley R. Epidemiology and costs of chronic obstructive pulmonary disease // European Respiratory Journal. - 2006. - № 27(1). - P. 188-207.
- Divo M., Cote C., de Torres J.P., Casanova C., Marin J.M., Pinto-Plata V.,.. & BODE Collaborative Group. (2012).Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease // American journal of respiratory and critical care medicine. - 2012. - № 186 (2). - P. 155-161.
- Hiram R., Naud P., Xiong F., Al-u'datt D.A., Algalarrondo V., Sirois M.G.,.. & Nattel S. Right atrial mechanisms of atrial fibrillation in a rat model of right heart disease // Journal of the American College of Cardiology. - 2019. - № 74 (10). - P. 1332-1347.
