Causes and factors promoting the expansion of cardiovascular diseases in the Vologda oblast (according to the research in epidemiology of cardiovascular disease)
")
Author: Shabunova Aleksandra Anatolevna, Fakhradova Leila Natigovna
Journal: Economic and Social Changes: Facts, Trends, Forecast @volnc-esc-en
Section: Economics and sociology of public health and healthcare
Article in issue: 1 (37) т.8, 2015.
Free access
The article focuses on the analysis of risk factors for cardiovascular diseases. The data of the research in epidemiology of cardiovascular disease (ESSE-2013), carried out in the Vologda Oblast, and the materials of the state statistics service comprise an information base. The ESSE-2013 questionnaire included several thematic blocks corresponding to the main factors influencing the development of cardiovascular diseases. The distribution of respondents' answers reveals that there is a connection between cardiovascular diseases and effects of such factors as gender, age, heredity, and the body mass index. Of all the respondents who had infarction, 40% mention that their close relatives suffer from this disease as well. Of those who had a stroke, 30% have relatives with such a disease. The comparison of the respondents' age and gender characteristics by the presence of cardiovascular diseases shows that men and women over60 belong to the risk groups of such diseases as stroke, stenocardia and cardiac arrhythmia; the risk of heartattack is very high for men over 60; heart rhythm disorders - for women under 60...
Cardiovascular disease, risk groups, risk factors, health
Short address: https://sciup.org/147223687
IDR: 147223687 | UDC: 316.728+314.4(470.12) | DOI: 10.15838/esc/2015.1.37.9
Text of the scientific article Causes and factors promoting the expansion of cardiovascular diseases in the Vologda oblast (according to the research in epidemiology of cardiovascular disease)
Public health is one of the main factors in successful functioning of the society. Creation of the conditions to preserve and improve public health is a priority of any state. The Long-Term Program for Development of Healthcare of the Russian Federation contains 6 targets of public health1, the similar program for the Vologda Oblast2 – 12. The negative trends in the mentioned targets actualize the development and adoption of effective measures in healthcare, aimed primarily at disease prevention.
In the Russian Federation cardiovascular diseases are the key cause of mortality3, despite its 13 percent decrease in 2000– 2012. In the same period the morbidity rate for this cause increased by 55% and amounted to 2663 cases per 100 thousand population; the primary disability rate decreased by 29% ( tab. 1 ).
The situation is similar at the regional level: morbidity, disability and mortality from cardiovascular diseases are very high. In the Vologda Oblast diseases of the cardiovascular system continue to maintain the leading position among most frequent causes of death and disability of the adult population ( tab. 2 ). In 2012 the morbidity rate was by 32% higher that in 2000
The state of people’s health is affected by different factors, such as living conditions, lifestyle and hereditary. The conditions, circumstances and causes, increasing the probability of health problems, are defined as risk factors and combined into two groups: endogenous and exogenous. Health risk is considered as the possibility of development of harmful effects for a person (a group of people) in the presence of any danger4.
Depending on the source of origin all the risk factors are divided into four groups: lifestyle and socio-economic conditions, hereditary background, quality of the external environment and healthcare (according to the World Health Organization classification). The degree of their impact
Table 1. Morbidity, disability and mortality from cardiovascular diseases in the Russian Federation
|
Indicator |
Territory |
Year |
2012 to 2000, % |
||||
|
2000 |
2003 |
2006 |
2009 |
2012 |
|||
|
Mortality from cardiovascular diseases |
RF |
846.1 |
927.5 |
864.7 |
801.0 |
737.1 |
87 |
|
EU |
310.39 |
295.25 |
252.2 |
226.37 |
– |
||
|
Number of people firstly recognized as disable aged 18 and over, cardiovascular diseases (per 10,000 population) |
RF |
35.4 |
35.9 |
53 |
33.3 |
25.1 |
71 |
|
EU |
No data |
No data |
No data |
No data |
No data |
No data |
|
|
Incidence of cardiovascular diseases, per 100,000 population |
RF |
1718 |
2058.3 |
2647.1 |
2634.3 |
2663.1 |
155 |
|
EU |
2390.09 |
2473.38 |
2415.26 |
2416.09 |
– |
– |
|
Sources: Rossiiskii statisticheskii ezhegodnik 2010, 2013 [Russian Statistical Yearbook 2010, 2013]. Available at: wcm/connect/rosstat_main/rosstat/ru/statistics/publications/catalog/doc_1135087342078; Tsentral’naya baza statisticheskikh dannykh [Central Statistics Database]. Available at: ; Evropeiskaya baza dannykh “Zdorov’e dlya vsekh” [European Health for All Database]. Available at:
Table 2. Morbidity, disability and mortality from cardiovascular diseases in the Vologda Oblast
The factors’ impact on health can be assessed by comparing the person’ susceptibility to certain diseases, taking into account the presence of risk factors for their development.
The causes of cardiovascular diseases are often the following: poor diet (the body mass index (BMI) is higher a normal range), smoking, alcohol abuse, sedentary lifestyle, genetic predisposition. At the present time, there are more than 200 different risk factors for cardiovascular diseases [11].
The epidemiological study of cardiovascular diseases was conducted by ISEDT
Table 3. Grouping of risk factors affecting the health of the population
|
Factor groups |
Share, % |
Components |
|
1. Lifestyle and socio-economic conditions |
49 – 53 |
Smoking, poor diet, excessive alcohol consumption, harmful working conditions, stress, physical inactivity, poor living conditions, drug abuse, fragility of families, loneliness, low educational and cultural levels, excessive urbanization |
|
2. Hereditary background |
18 – 22 |
Hereditary predisposition to diseases |
|
3. Quality of the external environment |
17 – 20 |
Environmental pollution, hazardous working conditions, sudden change of weather; elevated levels of radiation, solar and magnetic radiation |
|
4. Healthcare |
8 – 10 |
Ineffectiveness of preventive measures, low quality of medical care and time-lag in its provision |
|
Source: Lisitsyn Yu.P. Obshchestvennoe zdorov’e i zdravookhranenie: uchebnik [Public Health and Healthcare: Textbook]. Moscow: GEOTAR-Media, 2009. p. 45. |
||
RAS in 2013 in the Vologda Oblast under contract with the Federal State Institution the National Research Center for Preventive Medicine of the Ministry of Healthcare of the Russian Federation.
The region participated in the allRussian project “Epidemiology of cardiovascular disease” (“ESSE – RF”). The work was aimed at carrying out a screening survey of the Vologda Oblast and forming a database to evaluate the epidemiological situation of cardiovascular diseases (CVD) and its risk factors in the RF subject.
The survey was conducted at the field stage of the research. The research questionnaire included 12 thematic blocks to assess the main factors influencing the person’s health. The sample size was 1650 urban and rural people. The respondents were aged 25–64. It provided an objective view of the epidemiology of cardiovascular diseases among the adult population. The gender structure of the sample corresponded to the gender structure of the adult population.
The next research stage included the measurement of blood pressure and the blood draw to identify biochemical markers that accompany the development of pathologies of the cardiovascular system. The database was formed at the final stage of the laboratory research and the questionnaires processing [7].
This paper considers correlation of several factors with cardiovascular diseases. The results of the “ESSE – RF” project is an empirical basis for the analysis. As it was shown above (see tab. 3), the human health is primarily influenced by lifestyle and only then by hereditary factors.
The impact of the latter can be demonstrated by comparing the incidence of cardiovascular diseases in several generations of the same family. It is difficult to identify the correlation between the presence of negative lifestyle factors and the development of certain diseases. Sociological information is characterized by subjectivity, thus it is possible to consider just potential relationship between the studied phenomena.
Therefore, to clarify the nature of the relationship between the risk factor and disease, we calculated corresponding correlation coefficients (the Pearson criterion χ 2, allowing us to identify the presence or absence of correlation and the criterion φ , revealing the constraint force of variables)5.
The analytical stage of the study included the comparison of the data on people’s selfassessment of their health and their lifestyle with the objective characteristics of the state of their health, the type of professional activity and the level of education and income to identify the importance of social conditions and behavioral practices in forming the health of individuals.
Self-assessed health is a recognized method to identify the respondents’ state of health. The works of A.A. Shabunova, O.N. Kalachikova, K.N. Kalashnikov, N.A. Kondakova show the correlation of people’s behavior regarding their own health and self-esteem [1, 5]. People, highly estimating their own health, seek medical advice in time, follow the treatment regimen, and are aware of ways to prevent diseases. As a consequence, self-reported health can be considered as indicator and regulator of self-preservation behavior.
The distribution of the participants’ responses in the sample is a quantitative measurement of assessed health of the studied group. At the individual level, self-reported health is determined according to the scale, which can have a different gradation. In the “ESSE – 2013” questionnaire the respondents were given two scales. The first scale consisted of five levels: excellent, very good, good, satisfactory and bad. The second scale was graded from 0 to 100 (EuroQooL method, 1990); zero points corresponded to the worst possible health conditions, 100 points – the best.
The distribution of the respondents’ answers, according to both methods, has revealed a significant difference in selfreported health when using 5-point and 100-point grading scales. The study participants tended to give more positive, perhaps inflated, assessment of their health when using the 100-point grading scale and more pessimistic assessment when using the conventional 5-point scale. In the latter case, more than half of the respondents rated their health as satisfactory (51.6%) and 8% as poor ( fig. 1 ).
Perhaps, the differences are caused by various visual representations of the answer choices: the scale of the EuroQooL method was presented graphically in the form of a “thermometer”, where the respondent was supposed to put a mark, the five-point scale was presented verbally.
The consideration of endogenous uncontrollable factors includes the evaluation of the impact of gender, age and genetic predisposition on the development of cardiovascular diseases.
These studies demonstrate the existence of some correlation between cardiovascular diseases and age and gender characteristics of the respondents.
Figure 1. Distribution of the respondents’ assessments of their health according to the 5- and 100 point systems (in % of respondents number)
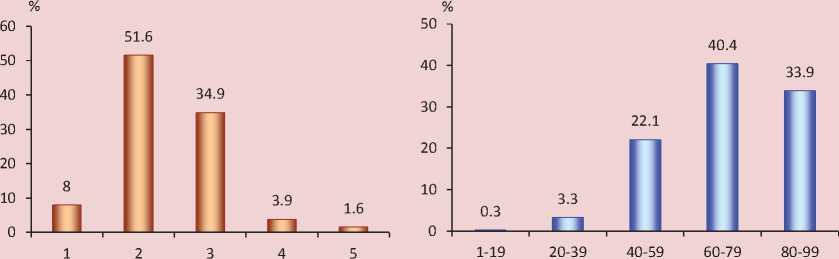
Note. Nomenclature on the left: 1 – poor state of health, 2 – satisfactory; 3 – good; 4 – very good; 5 – excellent.
Among men aged 60 and over the incidence of heart attack is by 10% higher than among women of the same age category ( fig. 2 ).
In the category of people aged 60 and over there are widespread diseases of the cardiovascular system, such as angina, stroke and heart rhythm disorder. Men of this age group are more prone to strokes (see fig. 2) and coronary heart disease ( fig. 3 ). The prevalence of cardiac arrhythmias in the group of people under 60 is higher among women; in the group of people aged 60 and over, the difference is smoothed.
The distribution illustrates diseases that prevail in the older age group. Cardiovascular diseases are less widespread among women of this age group due to the fact that within 10 years after the end of the fertile period they maintain resistance to the disease.
It is important to consider the presence of genetic predisposition, since this factor reduces the effectiveness of preventive measures against cardiovascular diseases significantly. So, 40% of the patients with myocardial infarction noted that their closest relatives had suffered from the disease. The situation is similar with strokes – 30% of the patients mentioned closest relatives that had suffered from this disease ( fig. 4 ).
To identify the correlation between hereditary, demographic characteristics and the likelihood of developing cardiovascular diseases with the help of the standard software package SPSS we calculated the Pearson criterion χ 2. The critical value is 3.841 at the 0.05 significance level. Table 4 is used to calculate the actual number of observations.
Figure 2. Prevalence of heart attacks and strokes among the population (in % of respondents number)
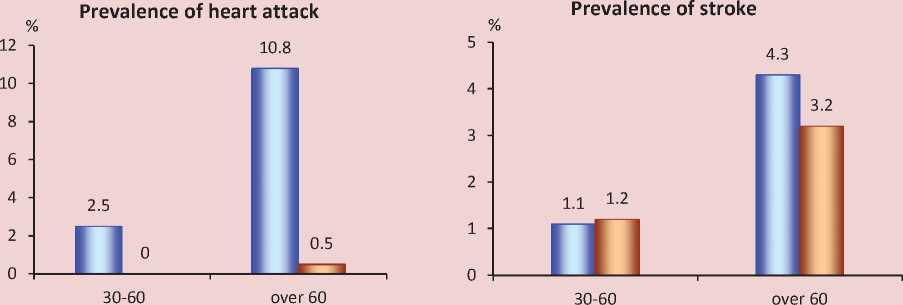
Men Women Men Women
Figure 3. Prevalence of angina and cardiac arrhythmias among the population (in % of the number of respondents)
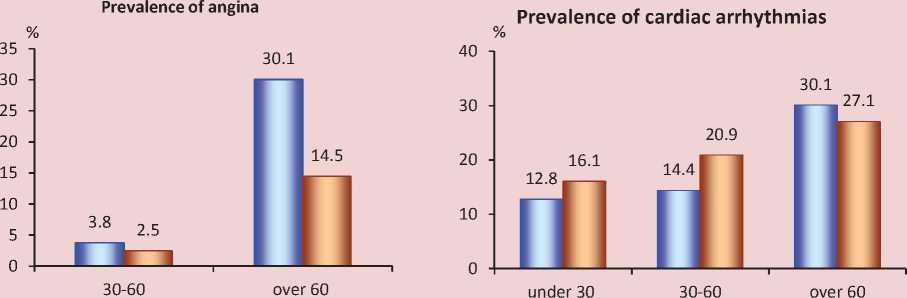
Men Women Men Women
Figure 4. Distribution of answers to the question: “Did/Does your mother, sisters (under 65), father, brothers (under 55) suffer from the following diseases: myocardial infarction, stroke? (in % of the number of respondents suffering from a relevant disease)
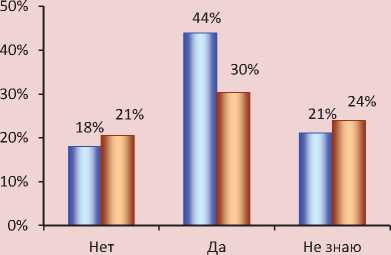
□ Cardiac infarction □ Stroke
No Yes I don’t know
Table 4. Observed occurrence
|
Risk factors |
Outcome |
||||||||||
|
stroke |
heart attack |
CHD |
heart rhythm disorder |
other heart diseases |
|||||||
|
yes |
no |
yes |
no |
yes |
no |
yes |
no |
yes |
no |
||
|
Hereditary background of myocardial infarction |
yes |
2 |
293 |
11 |
284 |
31 |
255 |
70 |
212 |
53 |
229 |
|
no |
21 |
1125 |
9 |
1140 |
51 |
1068 |
204 |
903 |
122 |
976 |
|
|
Hereditary background of cerebral stroke |
yes |
7 |
325 |
3 |
332 |
32 |
294 |
76 |
242 |
41 |
274 |
|
no |
16 |
1094 |
18 |
1094 |
52 |
1031 |
201 |
873 |
130 |
934 |
|
|
Hereditary background of arterial hypertension |
yes |
20 |
885 |
15 |
893 |
66 |
807 |
217 |
648 |
123 |
734 |
|
no |
3 |
544 |
7 |
542 |
18 |
523 |
66 |
468 |
56 |
475 |
|
|
Eldery age (retirement age) |
yes |
11 |
302 |
11 |
302 |
60 |
239 |
88 |
202 |
39 |
257 |
|
no |
13 |
1298 |
14 |
1302 |
37 |
1246 |
229 |
1041 |
155 |
1100 |
|
|
Men aged 60 and over |
yes |
4 |
88 |
10 |
82 |
28 |
61 |
28 |
61 |
11 |
78 |
|
no |
20 |
1512 |
15 |
1522 |
69 |
1424 |
289 |
1182 |
183 |
1279 |
|
|
Women aged 55 and over |
yes |
7 |
214 |
1 |
220 |
32 |
178 |
60 |
141 |
28 |
179 |
|
no |
17 |
1386 |
24 |
1384 |
65 |
1307 |
257 |
1102 |
166 |
1178 |
|
Table 5. Value of the criterion φ for the risk factors of cardiovascular diseases
|
Risk factors |
Stroke |
Other heart diseases |
Heart attack |
Heart rhythm disturbance |
CHD |
|
Eldery age (border - retirement age) |
φ = 0.082, р ≤ 0.001 |
No correlation |
φ = 0.079, р = 0.002 |
φ = 0.119, р ≤ 0.001 |
φ = 0.280, р ≤ 0.001 |
|
Men aged 60 and over |
No correlation |
No correlation |
φ = 0.186, р ≤ 0.001 |
φ = 0.068, р = 0.007 |
φ = 0.258, р ≤ 0.001 |
|
Women aged 55 and over |
No correlation |
No correlation |
No correlation |
φ = 0.091, р ≤ 0.001 |
φ =0.149, р ≤ 0.001 |
|
Hereditary background of myocardial infarction |
No correlation |
φ = 0.093, р ≤ 0.001 |
φ =0.102, р ≤ 0.001 |
φ = 0.065, р = 0.016 |
φ = 0.108, р ≤ 0.001 |
|
Hereditary background of arterial hypertension |
φ = 0.064, р = 0.014 |
φ = 0.055, р = 0.040 |
No correlation |
φ = 0.154, р ≤ 0.001 |
φ =0.087, р ≤ 0.001 |
|
Hereditary background of cerebral stroke |
No correlation |
No correlation |
No correlation |
φ = 0.055, р = 0.042 |
φ =0.089, р = ≤ 0.001 |
|
The table presents the values of the criterion φ and the value of the significance level p. |
|||||
For indicators, which relationship was confirmed by the Pearson criterion χ2, we determined constraint force by means of the criterion φ calculation. So, as for the hereditary factor, there is a weak correlation between the following diseases: the respondent who suffered from heart attack or coronary heart disease had relatives who had had heart attack, as well as the respondent who suffered from cardiac arrhythmias had relatives who had had arterial hypertension. As for the impact of gender and age characteristics, the relationship of the mean length is recorded between the factor “men aged 60 and over” and the outcome “coronary heart disease”. There is a weak correlation between the factor “women aged 55 and over” and the presence of coronary heart disease and cardiac arrhythmias (tab. 5). The mathematical analysis of the data has not revealed strong correlation between the risk factors and the presence of cardiovascular disease. The maximum constraint force is observed between the factor “retirement age” and the outcome “coronary heart disease”. The weaker impact of other causes can be caused by the fact that the joint effect of factors was not taken into account.
Lifestyle is an exogenous controllable factor. If we change it appropriately, we can reduce the risk of cardiovascular diseases significantly. Several blocks of the ESSE – RF questionnaires was devoted to this issue. We studied the following aspects: nutrition, physical activity, exposure to stressful situations and presence of harmful habits .
To characterize the impact of stress on the population’s health we compared the self-assessments of health and the degree of the respondents’ exposure to stress. Among those who assessed their own health above 90 points on the 100 point scale there was the highest proportion of those who never experienced stress (35%). The
Figure 5. Distribution of answers to the question: “How often were you nervous or how often did you experience stress during last month?” (in % of the number of respondents by groups of self-assessed health on the scale from 0 to 100 points)
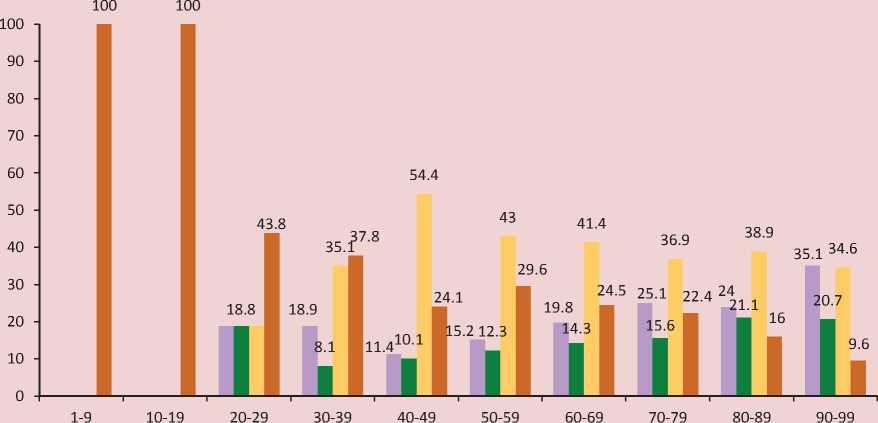
■ Never ■ Practically never Rarely ■ Rather often; very often
Note. According to the questionnaire rules, the choice of 0 or 100 points was not allowed to assess the state of health.
majority of the respondents who assessed their own health in the range from 40 to 89 points, experienced stress only sometimes (43%). When self-reported health is below 40 points there is a high exposure to stressful situations – from 37% (self-reported health between 30 and 39 points) to 100% (selfreported health less than 20 points) of the respondents often or very often felt stress ( fig. 5 ).
The dependence of the respondents’ state of health on the presence of harmful habits is weak. At the same time, the respondents are inclined to self-destructive behavior, such as alcohol consumption, though they suffer from cardiovascular diseases. Only after heart attack people refuse fortified wines and strong liquors completely; however, 56% of the group can drink vodka or brandy. Among those who had stroke, 62% drink strong alcohol, 50% – dry wine or champagne, 29% – beer, 16% – fortified wine and 8% – strong tinctures. In general, the presence of cardiovascular diseases does not lead to the refusal of alcohol consumption (fig. 6).
Diet has an indirect effect on the development of cardiovascular diseases. The differences in the diet of people with normal weight and obese people relate only to certain food groups: cheese, cereals and pasta. The respondents with obesity (third degree) often eat meat, more rarely cheese, cereals and pasta. The respondents with underweight body do not eat pickles, rarely eat cheese, but more often sour
Figure 6. Distribution of positive answers to the question: “Do you drink the following alcoholic beverages?” (in % of the number of respondents that have a specified disease of the cardiovascular system)
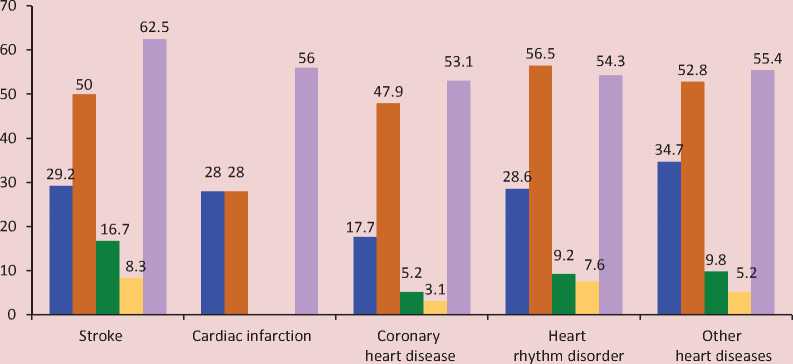
■ Beer ■ Dry wine or champagne
■ Fortified wine ■ Home-made strong tinctures
■ Vodka, brandy, other strong liquors
Table 6. Diet profiles
The ratio of the body mass index and the presence of cardiovascular diseases is different. Thus, among the respondents with class II obesity 13% suffered from angina and 24% – heart rhythm disorder. The largest share of those who had myocardial infarction was recorded among the respondents with class I obesity – 2.9%. The lower values among the respondents with class II and III obesity can be caused by the scarcity of data in the sample. Stroke prevails in the group of respondents with class II obesity and underweight. The highest share of those who suffered from heart rhythm disorders (27%) or had other heart diseases besides heart attack, stroke and angina is recorded among the respondents with class I obesity (14%; fig. 7).
According to the data presented in the work of Yu. P. Lisitsyn (2009), the adverse lifestyle factors contribute to the development of coronary heart disease by 60%,
Figure 7. Distribution of positive answers to the question: “Has a doctor ever told you that you have the following diseases?” (in % of the number of the respondents who have the appropriate body mass index)
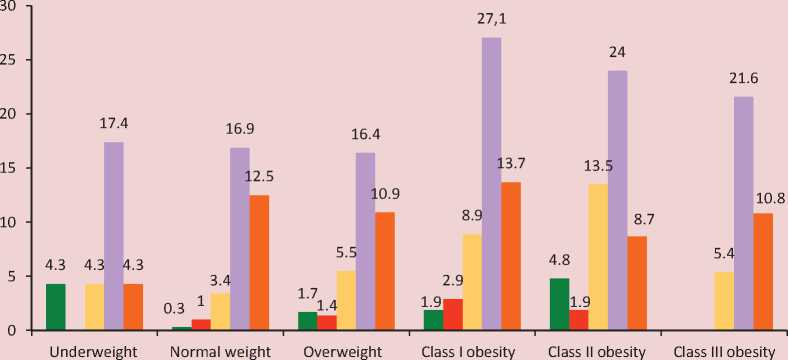
■ Stroke ■ Myocardial infarction ■ Angina ■ Heart rhythm disorder ■ Other heart diseases
Table 7. Distribution of risk factors for various chronic diseases (% of the effect)
The municipal healthcare institutions manage lifestyle factors in terms of preventive work with the population: educational, preventive, sport events. These measures can reduce the incidence of cardiovascular disease, prevent the development of complications.
The achievement of objectives to promote healthy lifestyles and reduce mortality in the region is characterized by the target indicators stipulated in the state program of the Russian Federation “Development of Healthcare” for the period up to 2020, and in the program “Development of Healthcare of the Vologda Oblast” for the period up to 20206. In accordance with these state programs in the Russian Federation the mortality rate from circulatory diseases should be reduced to 622.4 cases per 100 thousand population (by 16% compared to 2012) by 2020, in the Vologda Oblast – to 649.4 cases per 100 thousand population (by 28% compared to 2012).
Thus, the study has confirmed the significance of hereditary background and gender characteristics as risk factors of cardiovascular system. It has also revealed that the impact of the body mass index on the development of cardiovascular diseases is different. Thus, among the respondents with class II obesity 13% suffered from angina, 24% – heart rhythm disorders. The largest share of myocardial infarction was recorded among the respondents with class I obesity (2.9%), among them there was the largest share of those suffering from heart rhythm disorders (27%) and other heart disease besides heart attack, stroke and angina (14%). Stroke prevails in the groups of the respondents with class II obesity and underweight. The comparison of the lifestyle factors and the presence of cardiovascular diseases have not led to the identification of significant correlations. The reason can be the following: the study was one-time and did not assume the in-depth analysis of self-preservation behavior of people. To obtain more representative data on the impact of behavioral factors on the risk of cardiovascular diseases development it is necessary to conduct prospective studies. However, the respondents who assess their state of health as low are more often exposed to stress. Everyone who rates their health by 20 points and below (on the 100 point scale) often or very often experiences stress.
The spread of values and practices of a healthy lifestyle is the priority in combating cardiovascular diseases. Such culture should be created by the state, its competent bodies in the sphere of healthcare, the media, the society, employers and citizens. The state facilitates and regulates the actions to strengthen the population’s health. It develops strategies and programs in healthcare, distributes financial flows, determines common attitudes to health through media channels, controls and monitors the subordinate agencies’ performance. In general, the state has 2 options. In the first case the investment is directed in preventive measures, early diagnosis of diseases, strengthening the material and technological base of healthcare institutions, propaganda of a healthy lifestyle, control of working conditions in enterprises, monitoring of management effectiveness in the respective spheres. The consistent implementation of these actions leads to the minimization of GDP loss associated with poor health. The second option does not promote preventive medicine and a healthy lifestyle. In this case, the funds are supposed to compensate the negative changes in the population’s health; there are also additional costs from GDP underproduction. Obviously, the long-term effect requires the implementation of the first option.
References Causes and factors promoting the expansion of cardiovascular diseases in the Vologda oblast (according to the research in epidemiology of cardiovascular disease)
- Kalachikova O.N., Kalashnikov K.N. Analiz smertnosti naseleniya Vologodskoi oblasti ot serdechnososudistykh zabolevanii: otchet o NIR . Vologda: ISERT RAN, 2014. 59 p.
- Vvedenska y a I.I., Vvedenska y a E.S., Shilo v a L.S. Samootsenka zdoro v'y a kak pokazatel' samosokhranitel'nogo povedeniya pozhilykh . Problemy sotsial'noi gigieny, zdravookhranenie i istoriya meditsiny , no.5, 1999, pp. 12-15.
- Grzhibovskii A.M. Analiz nominal'nykh dannykh (nezavisimye nablyudeniya) . Ekologiya cheloveka , 2008, no. 6, pp.58-68.
- Zhuravleva I.V. Otnoshenie naseleniya k zdorov'yu . Moscow, 1993, p. 97.
- Shabunova A.A., Kalashnikov K.N., Morev M.V., Kalachikova O.N., Kondakova N.A. Zdorov'e i zdravookhranenie: uchebnoe posobie dlya vuzov . Under editorship of A.A. Shabunova. Vologda: ISERT RAN, 2014. 154 p.
- Lisitsyn Yu.P. Obshchestvennoe zdorov'e i zdravookhranenie: uchebnik . Moscow: GEOTAR-Media, 2009. 512 p.
- Boitsov S.A., Chazov E.I., Shlyakhto E.V., Shal'nova S.A., Konradi A.O., Karpov Yu.A., Muromtseva G.A., Zhernakova Yu.V., Oshchepkova E.V., Rotar' O.P., Balanova Yu.A., Balakhonova T.V., Baranova E.I., Gomyranova N.V., Deev A.D., Dobrovol'skii A.B., Dotsenko A.N., Evstifeeva S.E., REganyan.A., Kapustina A.V., Kontsevaya A.V., Kostareva A.A., MMamedov.N., Masenko V.P., Metel'skaya V.A., Meshkov A.N., Panchenko E.P., Postnov A.Yu., Potemkina R.A., Pustelenin A.V., Rogoza A.N., Ryabykina G.V., Skripnikova I.A., Titov V.N., Tkacheva O.N., Khudyakov M.B., Gutnova S.K., Toguzova Z.A., Tolparov G.V., Nevzorova V.A., Kulakova N.V., Nedogoda S.V., Chumachek E.V., Ilyin V.A., Kasimov R.A., Shabunova A.A., Furmenko G.I., Minakov E.V., Nazarova O.A., Romanchuk S.V., Belova O.A., Grinshtein Yu.I., Petrova M.M., Libis R.A., Isaeva E.N., Duplyakov D.V., Gudkova S.A., Karpov R.S., Trubacheva I.A., Medvedeva I.V., Shava V.P., Efanov A.Yu. Nauchno-organizatsionnyi komitet proekta ESSE-RF. Epidemiologiya serdechno-sosudistykh zabolevanii v razlichnykh regionakh Rossii (ESSE- RF). Obosnovanie i dizain issledovaniya [Epidemiology of Cardiovascular Diseases in Different Regions of Russia (Esse-Rf). The rationale for and Design of the study]. Profilakticheskaya meditsina [Preventive Medicine], 2013, no. 6, pp. 25-34.
- Yakushin S.S., Shal'nova S.A., Potemkina R.A., Filippov E.V., Balanova Yu.A., Boitsov S.A. Opyt organizatsii epidemiologicheskogo issledovaniya faktorov riska neinfektsionnykh zabolevanii v Ryazanskoi oblasti (po rezul'tatam pilotnogo proekta MERIDIAN-RO) . Profilakticheskaya meditsina , 2012, no.6, pp. 20-24.
- Razvitie zdravookhraneniya: gosudarstvennaya programma RF . Available at: http://ww w.rosminzdra v.ru/new s/2014/01/30/1686-gosudarstvennaya -programma-razvitiya-zdravoohraneniya-rossiyskoy-federatsii
- Razvitie zdravookhraneniya Vologodskoi oblasti: gosudarstvennaya programma . Available at://vologda-oblast.ru/special/dokumenty/18329/
- Evstifeeva S.E., Shal'nova S.A., Deev A.D., Gatagonova T.M., Efanov A.Yu., Zhernakova Yu.V., Ilyin V.A., Konradi A.O., Metel'skaya V.A., Oshchepkova E.V., Romanchuk S.V., Rotar' O.P., Trubacheva I.A., Shlyakhto E.V., Boitsov S.A. Rasprostranennost' povyshennogo urovnya S-reaktivnogo belka i ego assotsiatsii s traditsionnymi faktorami riska i zabolevaemost'yu u zhitelei Rossiiskoi Federatsii (Po dannym issledovaniya ESSE-RF) . Ratsional'naya farmakoterapiya v kardiologii , 2014, no. 10 (6), pp. 597-605
- Rossiiskii statisticheskii ezhegodnik 2010, 2013 . Available at: http://ww w.gks.ru/wps/wcm/connect/rosstat_main/rosstat/ru/statistics/publications/catalog/doc_1135087342078
- Shabunova A.A., Kalashnikov K.N., Kalachikova O.N. Obshchestvennoe zdorov'e i zdravookhranenie territorii . Under editorship of A.A. Shabunova. Vologda: ISERT RAN, 2010. 284 p.
- Shal'nova S.A., Kontsevaya A.V., Karpov Yu.A., Meshkov A.N., Boitsov S.A. Epidemiologicheskii monitoring kak instrument planirovaniya programm profilaktiki khronicheskikh neinfektsionnykh zabolevanii i ikh faktorov riska . Profilakticheskaya meditsina , 2012, no. 6, pp. 64-68.
- Lakatta E.G. Age-Associated Cardiovascular Changes in Health: Impact on Cardiovascular Disease in Older Persons. Heart Failure Reviews, 2002, no.1, pp. 29-49.
- Healthcare in Russia 2013. Available at: http://www.gks.ru/bgd/regl/b13_34/Main.htm
- Tsentral'naya baza statisticheskikh dannykh . Available at: http://www.gks.ru/dbscripts/cbsd/
- Evropeiskaya baza dannykh “Zdorov'e dlya vsekh” . Available at: http://data.euro.who.int/hfadb/shell_ru.html
- Statisticheskii ezhegodnik Vologodskoi oblasti 2013: stat. sb. . Vologdastat . Vologda, 2013. 371 p.
- Statisticheskii ezhegodnik Vologodskoi oblasti 2007: stat. sb. . Vologdastat . Vologda, 2007. 363 p.
- Lisitsyn Yu.P. Obshchestvennoe zdorov'e i zdravookhranenie: uchebnik . Moscow: GEOTAR-Media, 2009. p. 45
- Lisitsyn Yu.P. Obshchestvennoe zdorov'e i zdravookhranenie: uchebnik . Moscow: GEOTAR-Media, 2009, p.46.
