Comparative analysis of complications in different combinations of immunosuppressive therapy after kidney transplantation

Author: Ashimov Zhamalbek, Gaibyldaev Zhanybek, Abibillaev Damirbek, Kocyigit Fuat
Journal: Бюллетень науки и практики @bulletennauki
Section: Медицинские науки
Article in issue: 2 т.7, 2021.
Free access
In the length of time, a wide variety of drug combinations emerged in the management of post-transplantation therapy in order to improve the survival of the recipient and graft. However, the efficacy and safety of the applied combinations regarding the rejection and other complications are continuing to be the subject of research. In our study, our aim is to compare the effects of various combinations, namely cyclosporine with mycophenolate mofetil/mofetil mycophenolic acid with prednisolone and tacrolimus with mycophenolate mofetil/mofetil mycophenolic acid with prednisolone in a length of time. Methods. A total of 204 patients included into the study who received post-renal transplantation treatment in Scientific-Research Institute of Heart Surgery and Organs Transplantation and followed-up over a 10-year period. The estimated survival probabilities in the study were determined by the Kaplan-Meier method; whereas intragroup comparisons were evaluated by Log-rang, Breslow, and Tarone-Ware tests. Complications occurred in patients with combinations were analyzed by Chi-square and its alternatives. Hazard risk factors were tested by Cox regression analysis. Results. Of these 204 patients, 36 received Cyclosporin combination (CCG) and 168 Tacrolimus combination (TCG). The estimated life expectancy of the patients of TCG was significantly longer than the CCG ones. Furthermore, gender and age did not have a significant effect on survival depending on time, however, gender and age-related hazard factor showed a significant difference in the groups. It was determined that chronic rejection was significantly different in patients who used tacrolimus combinations, the difference was close to the significant value in acute rejection analysis. Other adverse events, namely, infection, tumour and organ damage were statistically less common in the patient group treated with tacrolimus combinations. Conclusion. In general, TCG showed better results in contrast to CCG.
Post-transplantation therapy, survival estimates, drug combinations, acute rejection, chronic rejection, hazard factor
Short address: https://sciup.org/14120900
IDR: 14120900 | UDC: 615.2:[616.24-002:616.98:578.834.1]-036-074/-078 | DOI: 10.33619/2414-2948/63/13
Сравнительный анализ осложнений при разных комбинациях иммуносупрессивной терапии после трансплантации почки
В данное время для контроля посттрансплантационной иммуносупрессии появилось большое разнообразие комбинаций препаратов, направленных на улучшение выживаемости реципиента и трансплантата. Однако эффективность и безопасность применяемых комбинаций в отношении отторжения и других осложнений продолжают оставаться предметом исследований. Цель исследования состоит в том, чтобы сравнить эффекты различных комбинаций, а именно циклоспорин А, микофенолат мофетил, микофеноловая кислота, преднизолон с такролимусом, микофенолатом мофетила, микофеноловой кислотой, преднизолоном в течение длительного времени.
Text of the scientific article Comparative analysis of complications in different combinations of immunosuppressive therapy after kidney transplantation
Бюллетень науки и практики / Bulletin of Science and Practice
The aim of post-transplantation treatment (PTT) primarily relies on the preventing of graft rejection in order to maintain of the proper renal function. As a rule, the primary goal of PTT is to create an immunosuppressive effect on the patient to prevent graft rejection. If the immunosuppressive effect exceeds safe levels, the patient is prone to adverse events. As well as prevention of possible drug toxicity and other adverse effects remains one of the key purposes of PTT [1]. In order to achieve these objectives in a balance, the treatment is applied via combination modes.
Frequently applied drugs in combinations include corticosteroids, calcineurin inhibitors and antiproliferative agents. As long as the PTT prescribed, patients undergo maintenance phase following the induction phase. Literature studies have been concentrated on both intragroup and intergroup interactions of the components of drug combinations [2]. The primary objectives of those studies are examining the nature of the graft rejection, life expectancy and predispositions to complications on the background of drug combinations during the maintenance phase.
Nevertheless, different drug combinations require more detailed and complex tests to find out their direct relationship to the survival of a patient and the transplant, as well as the complications in the causal relationship. Furthermore, studies on the drugs that have an immunosuppressive effect are still ongoing. One of these tests is the comparison of the effects of different combinations, including Cyclosporine (CsA) and Tacrolimus (TAC) drugs from the calcineurin inhibitor group.
Based on this rationale we aimed to conduct comparative analysis on two combinations of the calcineurin inhibitors in renal recipients within the time frame of the maintenance phase of posttransplantation therapy.
Materials and methods
A total of 204 patients who received post-transplantation treatment and followed-up in the Scientific-Research Institute of Heart Surgery and Organs Transplantation were enrolled in our study. The study is a retrospective study in which patient mortality and complications encountered over a period of 10 years are evaluated. Further, patients were categorized into two groups according to treatment options: 36 patients treated by Cyclosporine combination, CsA+Mycophenolate mofetil (MMF) +Prednisolone (P) (CCG); 168 patients managed by Tacrolimus combination, TAC+MMF + P (TCG).
Statistical analysis
Continous variables were depicted by mean, median, standard deviation, whereas categorical were shown by absolute count and percentages.
We compared TCG and CCG survival differences and calculated relationship between groups and survival status and other complications and risks.
The Mann-Whitney U test was applied for calculation of the differences between groups.
The Kaplan-Meier analysis was conducted for comparing the survival estimates, further Logrank; Breslow, and Tarone-Ware tests were applied to calculate survival factor differences.
We evaluated hazard ratios treatment combination group by Cox regression analysis. Then we applied Logistic regression for calculation of the hazard ratio to find out risk estimates of treatment options on complications [3].
Last, we used Chi-square statistical techniques for calculation of the relations between treatment combinations and acute-chronic rejections, infections, organ damages and neoplasia. We considered P<0.05; CI 95% for all statistical techniques as the statistical significance [4–8].
Results
Descriptive data of the patients in the treatment groups, the average age, gender, survival status and the life years are shown in Table 1.
DESCRIPTIVE DATA ON BASELINE VARIABLES
Table 1.
|
Groups |
N (%) |
Age |
Gender Male (%) |
Survival status, dead (%) |
Distribution of mortality by year |
|
si |
st ^ |
||||
|
TCG |
168(82,4) 38.30 |
34.0 12.8 0,32 |
115(68.5) |
8(4.8) |
2.25 1.5 1.58 5 |
|
CCG |
36(17,6) 39.41 |
36.0 10.9 |
27(75) |
8(22.2) |
3.87 5 2.47 6 |
|
Total |
204(100) |
142 (69.6) |
16(7.8) |
TCG — tacrolimus combination group, CCG — cyclosporine combination group, SD — standard deviation.
MORTALITY AND COMPLICATIONS FOLLOW-UP DATA
Table 2.
|
Years |
CCG |
TCG |
|||||||
|
M |
% |
SE sdeE |
comp |
M |
% |
SE |
sdeE |
Comp |
|
|
1 |
3 |
37 |
0.917 0.46 |
2 AR, 1 CR |
4 |
50 |
0.976 |
0.012 |
2 AR, 2 CR |
|
2 |
0 |
2 TBS |
1 |
12.5 |
0.969 |
0.014 |
1 CR, 1 HP |
||
|
Years |
CCG |
TCG |
||||||||
|
M |
% |
SE |
sdeE |
comp |
M |
% |
SE |
sdeE |
Comp |
|
|
3 |
0 |
1 |
12.5 |
0.957 |
0.018 |
|||||
|
4 |
0 |
1 |
12.5 |
0.941 |
0.024 |
1 CR, 1 LF |
||||
|
5 |
3 |
37 |
0.720 |
0.107 |
1 LF, 1 TBS, 1 HP, 1 CR |
1 |
12.5 |
0.907 |
0.040 |
1 MI |
|
6 |
1 |
12,5 |
0.630 |
0.126 |
1 LF |
0 |
||||
|
7 |
1 |
12.5 |
0.473 |
0.166 |
1 MI, 1 CMV, |
0 |
1 CD
|
8 |
0 |
0 |
|
9 |
0 |
0 |
|
Total |
8 100 |
8 100 |
M — mortality, SE — survival estimate, AR — acute rejection; CR — chronic rejection; HP — herpes virus infection; LF — liver failure; MI — myocard infarction; CMV — cytomegaloviral infection; TBS — tuberculosis; CD — candidosis.
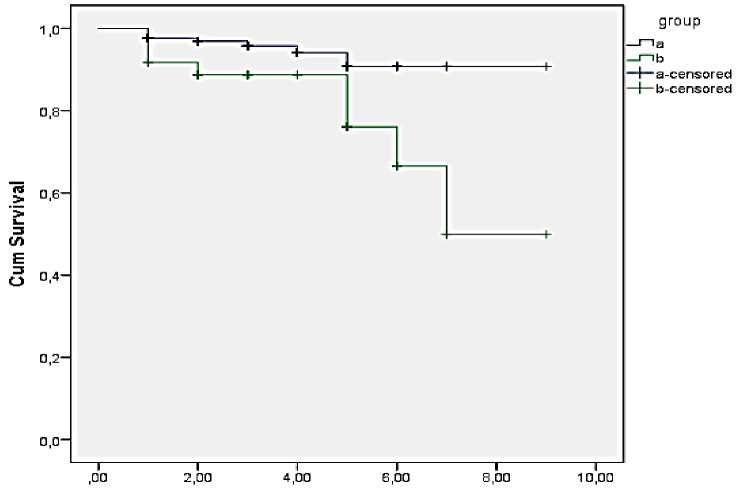
The Kaplan-Maier survival analysis revealed a statistically significant difference between the two groups: P <0.05 (Log-Rank 0.014; Brestlow 0.38; Tarone-Ware 0.26). The survival curves of the groups are shown in Figure.
Survival Functions
liveyear
Figure. Kaplan-Meier curves of combination groups.
The mortality cases in the CycA and TAC groups is shown in the table below. Accordingly, patient loss in both groups, as of the first year CCG 3; TCG 4 patients were lost. At the end of the follow-up period, the survival probability in the CCG was 0.473, Mean: 6.962: median 7.00 years, and the survival in TCG was 8.471 year.
The age variable of the treatment groups were grouped as 0-27; 28-39; 40-59 and 60-78 and independently, those on mortality were examined by Log-Rank test and found to be ineffective P> 0.05 (Log-Rank, CCG 0.418 TCG 0.214) The striking issue regarding the age groups is that there are 13 patients aged 60 and over, although there was no mortality in this age group.
The effect of gender on mortality in the treatment groups was examined using the Log-Rank test and no significant relationship was found for both groups (P>0.05, log-rank CCG=454; TCG=204).
The effect and hazard ratios of treatment combinations, age and sex variables within a time analyzed by Cox regression analysis. According to results age and gender did not show impact, whereas treatment groups revealed significant differences. Mortality risk ratio in CCG was found 3.26-fold higher than those in TCG (P<0.021; 95% CI 1.192-8.918).
Table 3. SURVIVAL ESTIMATES AND HAZARD RISK ANALYSIS
|
Variables |
Analyzed factor |
Analysis result (p value) |
Statistical technique |
|
Drug groups: TCG(a) and CCG(b) |
Survival estimates |
˂0,05 |
Log-rank |
|
Gender: Male and Female |
Survival estimates |
˃0,13 |
Log-rank |
|
Age groups: 9-27; 28-39; 40-59; 60-78 |
Survival estimates |
˃0,05 |
Log-rank |
|
Drug groups |
Hazard risk |
˂0,05 |
Cox regression |
|
Gender |
Hazard risk |
˂0,05 |
Cox regression |
|
Age groups |
Hazard risk |
˂0,05 |
Cox regression |
Drug combinations and complications
In the 10-year follow-up of CCG and TCG groups, complications with/without mortality were analyzed. Complications were categorized according to developed rejections, infections and other toxicity events. Table 4, 5 and 6 highlighted these complication categories.
|
REJECTION COMPLICATIONS |
Table 4. |
||||
|
Complications |
CCG |
TCG |
R ratio |
P value |
Total |
|
Acute rejection |
5/36 = .16 |
8/168=.048 |
3.226 |
057 |
|
|
Chronic rejection |
3/36= . 083 |
10 /168= . 0 595 |
705 |
||
|
Total rejections |
8/36=.22 |
18/168=.107 |
2.78 (CI |
030 |
|
|
INFECTIOUS COMPLICATIONS |
Table 5. |
||||
|
Complications |
CsA |
Tacrolimus |
R. ratio |
P value |
Stat. test |
|
Tuberculosis |
4(0.11) |
0/168= |
- |
033 |
Manthel-Haetsel |
|
CMV |
5(0,13) |
16/168=.095 |
- |
.544 |
Manthel-Haetsel |
|
Herpes virus |
6(0.16) |
18/168=.107 |
- |
.390 |
Fisher’s exact test |
|
Pneumonia |
2(0.05) |
0/168 100 |
- |
.030 |
Manthel-Haetsel |
|
Candidosis |
2(0.05) |
8/168 ... 0476 |
- |
.691 |
Fisher’s exact test |
|
Total infec. |
10(0.27) |
22/168= .13 |
2.55(CI |
.028 |
Chi-square test |
|
MI — myocardial infarction, CVE — cerebrovascular event. |
|||||
Discussion
We believe that analyzing the frequency of events in different combinations with statistical results will be useful in directing further studies on the subject.
As is known, with the introduction of CsA on humans (1978), the life span of the graft or the patient was significantly prolonged. Later, TAC was started to be used, although both drugs are calcineurin inhibitors, the different intracellular molecular action pathways may be the reason for the different effects to some extent in various combinations.
In the studies where different combinations of both drugs were used, the differences in rejection and complications were reported. Two other drugs used in combinations with calcineurin inhibitors are Mycophenolate Mofetil (MMF) and Prednisolone (P). Since both other drugs were dosed according to their blood concentrations, we looked for the difference in the use of CsA and TAC. In the literature, as well as comparisons between different groups, some studies revealed the cross-effect of this drug group by changing it [9]. We think that our study will also contribute to the subject, as each patient group studied has its own distinctive feature.
In our study survival and complication data of 204 kidney transplant recipients who received immunosuppressive treatment with two different calcineurin inhibitors were analyzed retrospectively. Results showed that mortality was statistically lower in the patient group treated with Tacrolimus combination (P = 0.034, long-rank). Moreover, the estimated life expectancy in patients treated with TAC at the end of 10 years was also longer than in the CsA group (90.7% vs 47%). On the contrary, some of the studies reported the lack of survival difference between TAC and CsA treatment groups (7, 11, 12, 13, 30 ...).
On the other hand, some studies reported the association of the decreased mortality risk and graft rejection rate with tacrolimus administration. According to them, the mortality rate in patients treated after transplantation was 13.375% in TAC arm vs 15,778% in the CsA arm (28), In another study, the 1-year survival rates for TAC and CsA were registered equally: 95.6% for both arms. Our study revealed these values as 97.6% for TAC and 91.7% for CsA. Furthermore, according to studies from developed countries mortality rate in patients treated with TAC was at the level of 4.8%, and 22.2% in those using CsA. These results confirmed the higher survival rate of TAC in contrast to CsA.
When the distribution of mortality by years was examined, patients who underwent TAC had 4 losses (2.38) in the first year, while this number was found to be 3 in the CsA group (8.33). Comparedly 3% mortality in 1st year after transplantation was registered in one medical center of England [10]. Accordingly, patient survival rate in the first year of TAC group can be evaluated as a positive outcome with 97%. Acute rejection and chronic rejection mortality causes were similar in both groups in the first year. For the ensuing years, mortality in the TAC group clustered in the first 5 years, while the mortality in the CsA group clustered in 5, 6, 7 years after the 1st year of transplantation. Causes of patient loss in the first year were similar or different. In general, it was observed that age and gender did not have a different effect on mortality and life expectancy in both treatment groups showed similar and different results in their study.
When the complications were examined which developed in the treatment combinations, the incidence of acute rejection was found to be lower in the TAC group, but this difference was not statistically significant (P = .057). Studies conducted in the same direction reported that TAC use gave similar results [11–14]: no difference was seen when chronic rejection was compared separately, however, overall rejection improvement showed a result in favor of tacrolimus (P = 0.030). In studies on the subject, although chronic rejection is not different, it has been reported that TAC application in general has a positive effect on graft rejection [15].
Development of cytomegaloviral (CMV), herpes viral (HV) and candidal infections did not differ between the combination groups. Tuberculosis and pneumonia were not occurred in the TAC group, while there were 2 cases in both infection types in the CsA group. One of the striking issues in the study results is that it showed a low incidence with tuberculosis (0,98%), and also that tuberculosis and pneumonia were not developed in patients who were administered tacrolimus, which was assumed to have a stronger immunosuppressive effect than CsA. In a study conducted in Belgium on the subject, the incidence of tuberculosis was shown as 0.35% for 2502 patients and it was concluded that the incidence of mycobacterial infection after kidney transplantation did not increase with the use of newer and more powerful immunosuppressive drug [16]. This recommendation seems consistent with our results. In addition, some studies have reported that there is no difference between the two calcineurin groups in terms of infectious complications. One study emphasizes the increased likelihood of tuberculosis development in young patients on the background of TAC prescription [15] ... reported that the reason for the difference between TAC and CSA infection has not yet been explained at the molecular level. On the other hand, CMV, herpes virus, candidose did not differ between the two drug groups. In addition, the data obtained have shown that infectious complications such as CMV, candidose and Herpes virus mostly seen combinedly in patients [9, 17]. Another crucial finding is that infectious complications developed together with acute and chronic rejection in the same patients, mostly in the CsA group. It has been observed that these cases mostly resulted with mortality.
When we looked at the volume of organ damage between combinations, myocardial infarction (MI), liver failure and cerebrovascular diseases were found in lower rates in both groups with insignificant difference. However, urethral stenosis was proportionally higher in the CsA group. Generally, the development of significant organ damage in patients treated with CsA suggests that the toxicity of the CsA combination is more dictating. According to the literature findings, TAC administration is associated with less development of hypertension, hypercholesterolemia and dyslipidemia in transplant patients compared to CsA [18]. We know that these factors increase the development of MI. In our study, no difference was found in terms of MI in both groups (p=1). Due to lack of the data on other factors no results were obtained. The development of malignancy revealed the 1 case in the TAC group (.006), 5 cases in the CsA group [11] and the difference was statistically significant (p <.001). Although findings showed no difference between the two drug applications in studies on the malignancy issue [19], CsA has been found with higher malignancy occurrence. Despite the opinions that TAC has a stronger immunosuppressor effect, it was found worth studying on the superiority of the TAC in terms of cancer safety. Considering that malignancy development may be related to immune balance, we can say that this issue can be supported by more detailed studies.
As a result, we can say that the combination with TAC shows less complications such as mortality rate, total rejection, infection and malignancy compared to CsA. However, the small number of patients in the CsA combination group may result in higher case rates. In addition, complications that could not be included in the study during post-transplantation maintenance therapy constitute a limitation for generalizing the results achieved.
References Comparative analysis of complications in different combinations of immunosuppressive therapy after kidney transplantation
- Vandermarliere A., Audenhove A. V., Peetermans W. E., Vanrenterghem Y., Maes B. Mycobacterial infection after renal transplantation in a Western population // Transplant infectious disease. 2003. V. 5. №1. P. 9-15. DOI: 10.1016/j.ejogrb.2004.06.033
- Atasever A., Bacakoglu F., Toz H., Basoglu O. K., Duman S., Basak K.,.. Sayiner A. Tuberculosis in renal transplant recipients on various immunosuppressive regimens // Nephrology Dialysis Transplantation. 2005. V. 20. №4. P. 797-802. DOI: 10.1093/ndt/gfh691
- Luuk Hilbrands. Strategies to improve patient outcomes in kidney transplantation health europe, chair DESCARDESBN working group, ERA-ETA. 1 August 2018. http://web.era-edta.org
- Arend S. M., Westendorp R. G. J., Kroon F. P., Van't Wout J. W., Vandenbroucke J. P., Van Es L. A., Van Der Woude F. J. Rejection treatment and cytomegalovirus infection as risk factors for Pneumocystis carinii pneumonia in renal transplant recipients // Clinical infectious diseases. 1996. V. 22. №6. P. 920-925. DOI: 10.1093/clinids/22.6.920
- Weir M. R., Burgess E. D., Cooper J. E., Fenves A. Z., Goldsmith D., McKay D.,.. Taler S. J. Assessment and management of hypertension in transplant patients // Journal of the American Society of Nephrology. 2015. V. 26. №6. P. 1248-1260. DOI: 10.1681/ASN.2014080834
