Comprehensive Review of Acute Respiratory Viral Infection: Influenza and the Efficacy of Vaccination Strategies

Author: Abzhaparova A., Choudari Ashwath, Rajnish Kumar, Arjun Yadav, Akash Jaiswal
Journal: Бюллетень науки и практики @bulletennauki
Section: Медицинские науки
Article in issue: 2 т.12, 2026.
Free access
Seasonal influenza remains a persistent global health challenge, characterized by the virus’s rapid evolution through antigenic drift and the complex human behaviors that drive transmission. This study provides a comprehensive analysis of the 2024–2025 influenza season, anchored by a cross-sectional Knowledge, Attitudes, and Practices (KAP) survey of 578 respondents. The research aims to evaluate public understanding of influenza virology, assess vaccination uptake, and identify barriers to effective prevention. Results indicate a significant “knowledge-behavior gap.” While 84.2% of participants correctly identified the influenza virus and 82% understood respiratory transmission, these insights did not translate into consistent best practices. A critical “Antibiotic Paradox” was observed: although 69.9% of respondents knew antibiotics are ineffective against viral flu, 25.1% reported self-medicating with them immediately upon symptom onset. Vaccination coverage in the cohort was 51.6%, with hesitancy primarily driven by fear of side effects (18.3%), needle phobia (18.3%), and a lack of provider recommendation (16.6%). This review concludes that while health literacy regarding the biological nature of influenza is high, public health strategies must pivot from pure education to behavioral intervention—specifically targeting antibiotic stewardship and addressing the physical and psychological barriers to vaccination.
Influenza, vaccination strategies, antibiotic resistance (amr), antigenic drift, vaccine hesitancy, health behavior
Short address: https://sciup.org/14134447
IDR: 14134447 | UDC: 616.9-053.2-06:616.24-008.6 | DOI: 10.33619/2414-2948/123/35
Комплексный обзор острых респираторных вирусных инфекций: грипп и эффективность стратегий вакцинации среди студентов-медиков
Сезонный грипп остается серьезной глобальной проблемой здравоохранения, характеризующейся быстрой эволюцией вируса посредством антигенного дрейфа и сложным поведением человека, которое способствует передаче инфекции. В данном исследовании представлен всесторонний анализ сезона гриппа 2024–2025 годов, основанный на поперечном исследовании знаний, отношения и практики (KAP), проведенном среди 578 респондентов. Цель исследования — оценить понимание общественностью вирусологии гриппа, оценить охват вакцинацией и выявить барьеры для эффективной профилактики. Результаты указывают на значительный «разрыв между знаниями и поведением». Хотя 84,2% участников правильно определили вирус гриппа, а 82% понимали передачу инфекции респираторным путем, эти знания не привели к последовательному внедрению передовых методов. Была отмечена критическая «антибиотико-парадоксальная ситуация»: хотя 69,9% респондентов знали о неэффективности антибиотиков против вирусного гриппа, 25,1% сообщили о самолечении ими сразу после появления симптомов. Охват вакцинацией в когорте составил 51,6%, при этом нерешительность в основном была вызвана страхом перед побочными эффектами (18,3%), боязнью игл (18,3%) и отсутствием рекомендаций врача (16,6%). Этот обзор приходит к выводу, что, несмотря на высокий уровень медицинской грамотности в отношении биологической природы гриппа, стратегии общественного здравоохранения должны перейти от чисто образовательной работы к поведенческому вмешательству — в частности, к рациональному использованию антибиотиков и устранению физических и психологических барьеров на пути к вакцинации.
Text of the scientific article Comprehensive Review of Acute Respiratory Viral Infection: Influenza and the Efficacy of Vaccination Strategies
Бюллетень науки и практики / Bulletin of Science and Practice
UDC 616.9-053.2-06:616.24-008.6
This research relies on a dual-source data strategy to ensure both local relevance and scientific accuracy:
-
1. Primary Data (The Survey). Instrument: A structured Knowledge, Attitudes, and Practices (KAP) questionnaire distributed digitally.
-
2. Secondary Data (Literature & Guidelines). Epidemiological Data: Surveillance reports from the World Health Organization (WHO) and CDC regarding the 2024–2025 circulating strains (e.g., H1N1, H3N2 subclade K).
Sample Size: N = 578 valid responses. Demographics: The cohort included a mix of age groups (29.2% aged 18–24; 23.2% aged 50+), with a significant portion (53.8%) reporting chronic health conditions.
Timeframe: Data was collected during the active 2024–2025 influenza season.
Clinical Guidelines: Protocols on vaccination composition and antimicrobial stewardship.
Summary of Findings
The study yielded four major findings regarding how the population interacts with the threat of influenza:
-
1. High Theoretical Knowledge The population demonstrates strong "textbook" knowledge of influenza. 84.2% correctly identified the pathogen as a virus (not bacteria). 82.0% correctly identified coughing/sneezing (respiratory droplets) as the primary mode of transmission. 71.6% understood the complex concept of "Antigenic Drift"—that the virus mutates frequently, necessitating annual vaccines.
-
2. The "Antibiotic Paradox" Despite high knowledge, there is a dangerous disconnect in practice regarding antibiotic use. 69.9% of respondents correctly answered "False" to the statement that antibiotics treat the flu. 25.1% of respondents stated their first course of action upon getting flu symptoms is to "Self-medicate with antibiotics immediately."
-
3. Vaccination Barriers are Emotional and Structural With a vaccination rate of 51.6%, the unvaccinated population cited specific, actionable barriers. Fear: Combined, 36.6% of non-vaccinated individuals cited fear as their primary reason (18.3% fear of side effects + 18.3% fear of needles/pain). Systemic Failure: 16.6% of people did not get vaccinated simply because "The doctor did not recommend it," highlighting a missed opportunity for healthcare providers to intervene.
-
4. Risk Perception. Red Flags: The public is generally astute regarding severe symptoms; 72.5% correctly identified shortness of breath as a critical emergency warning sign.
Implication: This behavior confirms that antibiotic misuse is driven by a cultural reliance on "strong medicine" or a desire for quick relief, rather than a lack of knowledge.
Symptom Confusion: However, 40.3% incorrectly believed high fever was not a typical flu symptom, suggesting some confusion between the flu, the common cold, and other respiratory viruses.
The Perpetual Challenge of Influenza.
Influenza is more than just a bad cold; it is a serious Acute Respiratory Viral Infection (ARVI) with a global footprint. Every year, seasonal epidemics result in 3 to 5 million cases of severe illness and hundreds of thousands of respiratory deaths worldwide. Unlike many other stable viruses, influenza is a moving target . Its ability to mutate ensures that our immune systems are constantly playing catch-up, creating a perennial burden on hospitals and economies alike. The 2024–2025 season has been characterized by high transmission rates, driven by the cocirculation of Influenza A(H1N1) and A(H3N2) strains. This resurgence serves as a reminder that despite advancements in medical technology, the interaction between viral evolution and human behavior dictates the severity of any given flu season [1-8].
Why We Need a New Shot Every Year: Antigenic Drift. One of the most common questions from patients is, "Why do I need a flu shot every year?" The answer lies in a biological process called Antigenic Drift. Influenza viruses are sloppy replicators. When they copy their genetic material, they make small mistakes. Over time, these small mutations accumulate, changing the virus's surface proteins (antigens) just enough that the antibodies we developed from a previous infection or vaccine no longer recognize the virus. This "drift" is why a person can get the flu multiple times over their lifetime and why vaccines must be reformulated annually to match the currently circulating strains. The Primary Defense. Vaccination remains our best tool for preventing severe disease. For the current season, health authorities like the WHO recommend "trivalent" vaccines, which protect against three specific viral strains: two Influenza A subtypes and one Influenza B lineage. While the goal is to prevent infection entirely, the vaccine's secondary role is equally vital: damage control. Even if a vaccinated person gets sick (perhaps due to a drift in the virus), the vaccine often acts as a buffer, turning what could be a life-threatening hospitalization into a manageable illness. However, the success of any vaccination program depends on the public's willingness to roll up their sleeves — a decision heavily influenced by psychology and access.
The "Antibiotic Paradox". Perhaps the most alarming trend in respiratory health is the misuse of antibiotics. Antibiotics kill bacteria, not viruses. Using them for the flu is like trying to unlock a door with a credit card — it doesn't work, and it might damage the card.
Despite widespread educational campaigns, cultural habits around "self-medication" persist. Many individuals view antibiotics as a "strong cure-all" for any fever. This behavior accelerates Antimicrobial Resistance (AMR), a global crisis where essential drugs stop working against common infections. This study pays special attention to this disconnect: why do people take medicines they know won't work?
To understand the human side of the flu season, we conducted a cross-sectional Knowledge, Attitudes, and Practices (KAP) survey. The goal was to move beyond infection statistics and understand the mindset of the population during the 2024–2025 influenza season.
Participants: The study analyzed responses from 578 individuals. Format: A structured digital questionnaire.
The survey focused on four key areas:
Who are they? (Demographics: Age, profession, health status).
What do they know? (Knowledge of viral transmission, antibiotic utility, and why vaccines change).
How do they feel? (Attitudes toward vaccine safety and necessity).
What do they do? (Practices regarding vaccination, hygiene, and treatment seeking).
The respondents represented a diverse mix of ages and backgrounds, providing a good snapshot of the general population.
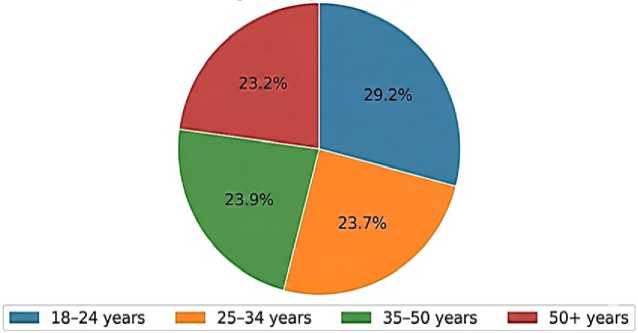
Figure 1. Age Distribution of Respondents’(N=578)
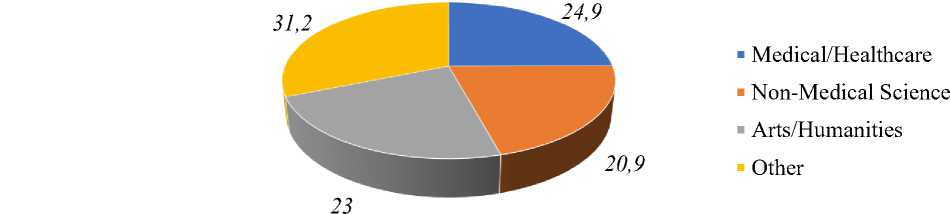
Figure 2. Professional Background
Primary Survey Data. The high number of participants with chronic conditions (53.8%) makes the findings particularly relevant, as these individuals are clinically considered "high-risk" for flu complications. Medical Knowledge: High Theoretical Understanding. Generally, the public understands the basics of the flu. 84.2% correctly identified the Influenza Virus (A, B, C) as the cause. Only 8.3% incorrectly thought it was a bacteria. 82% knew that the virus spreads primarily through respiratory droplets (coughing/sneezing). 71.6% understood that annual shots are needed because the virus mutates ("Antigenic Drift"). The "Antibiotic Paradox": Knowledge vs. Practice. Despite high knowledge scores, behaviors tell a different story. While nearly 70% of people know antibiotics don't work for the flu, a quarter of them use them anyway as a first response.

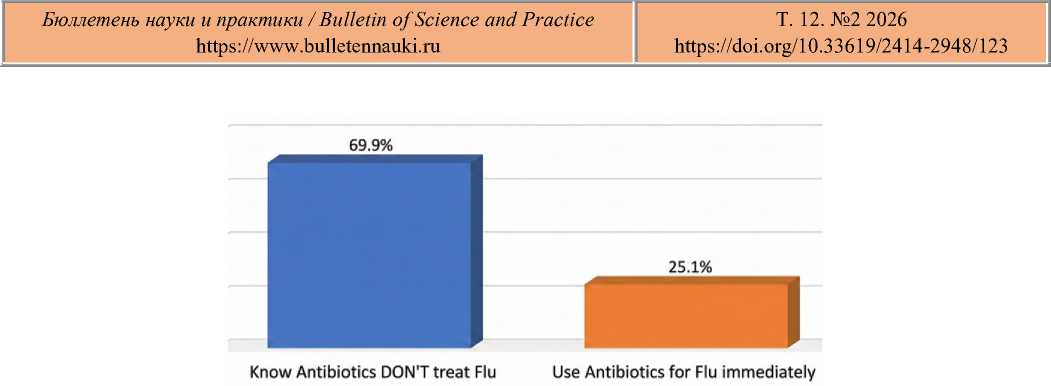
Figure 3. The Gap Between Knowledge and Action
Figure 3 shows the dissonance: 69.9% correctly identified antibiotics as ineffective, yet 25.1% self-medicate with them immediately upon symptom onset. Vaccination Uptake and Hesitancy. For the 2024–2025 season, the group was split almost evenly between vaccinated and unvaccinated individuals.
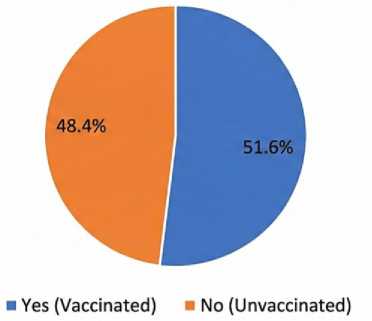
Figure 4. Vaccination Status (2024–2025 Season)
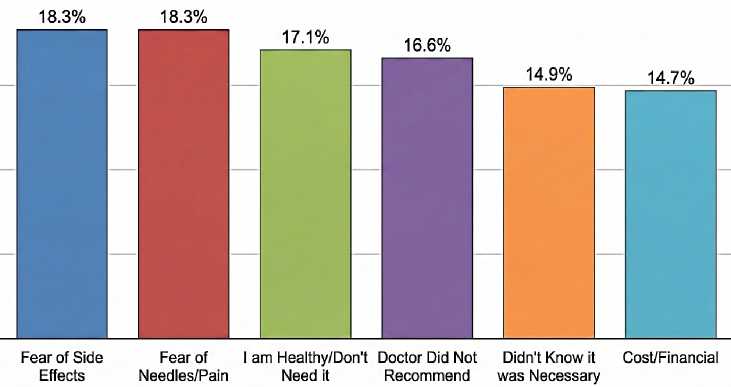
Figure 5: Main Reasons for Non-Vaccination (Primary Survey Data)
Why People Don't Vaccinate: Among those who opted out, the reasons were varied. Fear and a lack of provider recommendation were the top barriers. Bridging the Knowledge-Behavior Gap. The data exposes a classic public health dilemma: education alone isn't enough. People know the facts (flu is a virus), but under the stress of illness, they revert to "quick fixes" like antibiotics (Figure 3).
This suggests that the use of antibiotics is less about ignorance and more about a cultural reliance on "strong medicine" to feel better faster. To fix this, we don't just need more information brochures; we need better diagnostics. Rapid testing (like CRP point-of-care tests) at clinics can prove to a patient instantly that their infection is viral, reducing the demand for unnecessary drugs.
The "Silent" Doctor Problem. A crucial missed opportunity identified in this study (Figure 5) is the 16.6% of people who didn't vaccinate because "the doctor didn't recommend it." In medicine, silence is often interpreted as indifference. If a primary care provider doesn't actively bring up the flu shot, patients assume it isn't important for them. Healthcare systems need to shift from a passive "available if asked" model to a proactive "presumptive recommendation" model, where vaccination is the default standard of care. Addressing Fear and Hesitancy. Vaccine hesitancy is often framed as an intellectual debate, but our data shows it's largely emotional and physical. Nearly 20% of refusals were due to needle phobia or fear of pain. This is a very human barrier that is rarely addressed in public health campaigns. Promoting alternative delivery methods (like nasal sprays or microneedle patches) or simply acknowledging and managing procedural anxiety could convert a significant portion of the unvaccinated population. Additionally, the skepticism about vaccine efficacy (often linked to the "it doesn't work anyway" narrative) can be countered by explaining Antigenic Drift more clearly. When people understand that the virus changes—like a lock changing its key—they are more forgiving of the vaccine's variable effectiveness and more likely to see it as an annual update rather than a failed product.
Conclusion
The 2024–2025 influenza season offers a clear lesson: we have successfully taught the public what the flu is, but we haven't successfully changed how they respond to it.
The "Antibiotic Paradox"—where people use drugs they know are ineffective—poses a severe risk to global health by fueling drug resistance. Simultaneously, our vaccination rates are capped not just by anti-vaccine sentiment, but by simple barriers like fear of needles and a lack of provider enthusiasm.
Recommendations
Activate Providers: Doctors must proactively recommend the vaccine to every eligible patient, every season. Humanize the Experience: Address physical fears (pain, needles) directly in campaign messaging. Stewardship: tighten access to antibiotics to prevent self-medication and use rapid testing to reassure patients when antibiotics aren't needed. By addressing the human behaviors behind the statistics, we can build a more resilient defense against the ever-evolving threat of influenza.
