Distal radial artery dimensions in different body constitutions (prakriti)- an observational study
- an observational study")
Author: Sanu Usharani S., Prasad B.S., Patil Santosh, Hiremath R.R., Vernekar Sunil S.
Journal: Журнал стресс-физиологии и биохимии @jspb
Article in issue: 1 т.18, 2022.
Free access
Background: The fundamental principle of ayurveda is the tridosha theory ( three doshas) . These dosha are the causative and governing bio-energies responsible for the formation of body constitution. The vata dosha dominant personality have classical features like a small body frame when compared to kapha with large body built and broad anatomical structures. Pittaja body constitution has medium body built with reddish colouration and sharp features. Aim: This study aimed to correlate the radial artery intima-media thickness (IMT) and luminal diameter (LD) and further study its association with different body constitution ( prakriti ) and check the difference between the groups of prakriti . Methods: This observational cross-sectional study was done between May 2021 and June 2021 in the Department of Radiology, KLE Prabhakar Kore Charitable Hospital, Belagavi. Non-randomly selected volunteers ≥23 ±5years (n = 35) were divided into body constitution ( prakriti ) groups and evaluated for the IMT, LD (luminal diameter) of the radial artery using B-mode ultrasonography. Pearson’s co-relation was used to test the co-relation between the luminal diameter and intimae media thickness of distal radial artery. Chi-square test of independence was used to check the association between luminal diameter and intimae media thickness of distal radial artery with body constitution. One-way ANOVA was used to study the difference between the groups of prakriti . Results: The mean luminal diameter (LD) in vataja body constitution (5%) was 1.450 ± 0.495 mm, pittaja body constitution (11%) was 1.750±0.10 mm, kaphaja constitution (11%) was 1.70± 0.30 mm, vatapittaja body constitution (11%) was 4.15±0.47 mm, vatakaphaja body constitution (26%) was 1.64±0.83 mm, pittakaphaja constitution (23%) as 2.3±0.15 mm and samadhatuja constitution (11%) had 1.8±0.189 mm. The mean intima media thickness (IMT) in vataja body constitution (5%) was 0.05± 0 mm, pittaja body constitution (11%) was 0.03±0 mm, kaphaja constitution (11%) was 0.05± 0.014 mm, vatapittaja body constitution (11%) was 0.107±0.09 mm, vatakaphaja body constitution (26%) was 0.83±0.07 mm, pittakaphaja constitution (23%) was 0.313±0.006 mm and samadhatuja constitution (11%) had 0.350 ± 0.012 mm. As per the analysis a low positive Pearson’s correlation was found between IMT and LD (r = 0.254) between the luminal diameter (LD) and intima medial thickness (IMT) of distal radial artery. Chi square test of independence has shown significant association between DRA dimensions (IMT, LD) and body constitution ( prakriti) , palpatory blood vessel consistency. Among the observed values the v atakaphaja body constitution (0.83±0.07 mm) had increased intima media thickness (IMT). Among all the observed values the vatapittaja body constitution had broadest DRA luminal diameter (LD) of 4.15±0.47mm. One way ANOVA showed no significant difference between the groups of prakiti and IMT, LD of distal radial artery. Conclusion: As per the observations of the present study different body constitution (prakriti ) did not show any significant impact on distal radial artery dimensions (IMT and LD) as there are various factors like hormones, neural, blood volume regulators involved in vascular constriction and dilation. The prakriti assessment is a strong marker for prediction and the early diagnosis of diseases. This body constitution ( prakriti ) of an individual is the basic constituent on which the pulse wave variability of distal radial artery (DRA) acts.
Distal radial artery, intima-media thickness, luminal diameter, naadi pariksha, prakriti, ultrasonography
Short address: https://sciup.org/143178333
IDR: 143178333
Text of the scientific article Distal radial artery dimensions in different body constitutions (prakriti)- an observational study
Arterial pulse examination is the most ancient practices in the history of traditional medicine practiced all over the globe. Many superficial palpated arteries are listed in this examination. Among all arteries, the distal radial artery is the best for the pulse examination hence this is named as “ Jeeva Naadi ( represents life)” (Murthy, 1997).
In Ayurveda the panchamahabhoota theory, three doshas theory - vata, pitta, kapha (representing the transport functions, metabolic functions, accumulation functions of the body respectively), are the fundamentals of body functioning. The arterial pulse wave variability (P V) signifies the physiological components like doshas ( various bio-chemical regulatory factors ). Various naadi features like feeble pulse, a thin, low-pressure pulse is seen in vataja naadi , high pressure, warm pulse felt in pittaja naadi , medium pressure and volume with slow pulse felt in kaphaja naadi (Pandey, 2019) .The pulse wave variability is represented through many factors like pulse rate, rhythm, pulse wave amplitude, arterial luminal diameter, arterial intima media thickness. The perception of pulse waves depends on the blood vessel consistency. The blood vessel consistency in vataja body constitution as per classical text has increased the number of blood vessel networks, with small arterial lumen, pittaja body constitution will have a medium arterial lumen, kaphaja body constitution had broad arterial lumen (Govindaraj et al. , 2015). In Ayurveda, body constitution (Prakriti) is a thoughtful phenotype that is determined on the basis of physical, physiological, psychological, and behavioural traits. There are seven types of Prakriti mentioned in the classics (Bhushan, et al. , 2005). Earlier studies have reported association of Prakriti with various single nucleotide polymorphisms in HLA-DRB1, inflammatory and oxidative stress-related genes (Juyal et al. 2012), CD markers for blood cells (Rotti et al. 2014; Rotti et al. 2014a). Studies have reported the risk of cardiovascular risk factors associated with vatakapha and kapha body constitution (Mahalle, Kulkarni 2012). The Prakriti (genetic body constitution) of an individual was determined using Naadi vijyana (pulse-based diagnosis) by age-old Ayurveda physicians (Dey,
Pahwa, 2014).
The objective of this study is to study the co-relation between LD (luminal diameter) and IMT (intima-media thickness) of the distal radial artery, study the association between the distal radial arterial luminal diameters, intimae media thickness with the different body constitution ( Prakriti ), and study the difference of LD,IMT of distal radial artery between the groups of Prakriti in healthy middle-age volunteers.
MATERIALS AND METHODS
Study design and site:
This observational cross-sectional study was done between May 2021 and June 2021 in the Radiology Department of Radiology, KLE Prabhakar Kore Charitable Hospital Belagavi. This institutional ethical clearance was obtained and CTRI registration was done for his study (CTRI /2021/04/032940). The non-randomly selected volunteers ≥23 ±5years old (n = 35) were divided into body constitution ( Prakriti) groups and evaluated for the body constitution ( Prakriti ) using a questionnaire, IMT (intimae medial thickness), LD(luminal diameter) of the radial artery were measured by B-mode ultrasonography.
Prakriti evaluation:
The body constitution ( Prakriti ) of the healthy volunteers was assessed using a validated questionnaire based on physical, physiological, and psychological characteristics by an expert Ayurveda physician (Rastogi, 2012; Ghodke et al. , 2011). The Prakriti features were given a score of one each and the total % (percentage) was considered, if any specific Prakriti was allotted a score ≥of 60 %, then dominance of single dosha was considered. If there is a predominance of two dosha score of each ≥40% then the combination of two dosha was considered. The volunteers were recruited only after 80% concordance of questionnaire results with clinical evaluation by Ayurveda physician (Table 1).
Participants screening and study population:
Total of 40 healthy volunteers was screened for Prakriti assessment and USG for distal radial artery.
Inclusion criteria: Healthy volunteers of both male and female gender ≥23±5years, whose Prakriti assessment was done without any bias, whose distal radial artery parameters were obtained with USG were included in the study.
Exclusion criteria : The volunteers whose blood vessel wall had very thin consistency, which got compressed in B-mode ultrasonography, and unhealthy volunteers with or without medications were excluded from the study.
Ultrasound Doppler to obtain DRA (distal radial artery) Pulse data:
The apparently healthy volunteers fulfilling the inclusion criteria were asked to relax for 10 minutes and later pulse examination was done using 3hz B-mode ultrasonography probe at 3 sites on the distal radial artery. The standard three finger examination method (index finger for vata sthana , middle finger for pitta sthana , ring finger for kapha sthana ) explained in the classics was followed which states that the pulse data must be collected from the three consecutive sites from 2.1 ± 0.5cm (1 angula ) (Shirodkar, Mehmod, 2014) from the wrist joint representing vata (the distal part near the wrist joint examined by index finger), pitta (middle finger), kapha sthana (ring finger). As per the classical guidelines male volunteers radial pulse was examined in the right hand and female volunteers pulse was examined in the left hand. The volunteers were palpated manually for pulse parameters like pulse rate, pulse rhythm, blood vessel consistency (elastic thin, elastic soft with a medium consistency, and elastic thick and broad in palpation). The volunteer’s distal radial arterial pulse data namely IMT, LD (luminal diameter) was captured through a B-mode ultrasound Doppler probe by an expert radiologist. The probe was specially positioned transversely such that individual data from 3 consecutive sites can be captured. The data obtained was statically analyzed using the chi-square test of independence for testing the association between the IMT, LD (luminal diameter) of distal radial artery and body constitution ( prakriti ) of the same individual.
Statistical analysis:
The observed data was statically analysed using SPSS software. The Pearson’s Co-relation test was used to study the co-relation of IMT and LD of the distal artery in a 2X2 table. Further Chi-square test of independence was used to study the association of different body constitution with IMT and LD of the distal radial artery. One-way ANOVA test was used to test the difference between the means of luminal diameters and means of IMT (intima-media-thickness) in between different groups of prakriti.
OBSERVATIONS
Distribution of volunteer’s in different body constitution (prakriti):
Total 35 volunteers fulfilled the inclusion criteria were distributed in 7 categories of prakriti 6% vataja, 11 % in pittaja, 11% in kaphaja, 11% in vatapittaja, 26% in vatakaphajaprakriti, 22% in pittakaphaja and 11% samadhatuja prakriti. (Table 2)
Among 35 volunteers selected for the study the intimae medial thickness (IMT) of distal radial artery for vata prakriti is 0.05±0 mm, pitta prakriti is 0.03±0 mm, kapha prakriti is 0.05±0.014 mm. Vatapitta prakriti has 0.107±0.09 mm, Vatakapha prakriti has 1.6±0.083 mm, Pittakapha prakriti has 0.313±0.006 mm, Samadhatuja Prakriti has 0.350 ± 0.012 mm.
Among 35 volunteers selected for the study the luminal diameter (LD) of distal radial artery for vata prakriti is 1.450±0.049 mm, pitta prakriti is 1.750±0.010 mm, kapha prakriti is 1.70±0.03 mm. Vatapitta prakriti has 4.15±0.048 mm, Vatakapha prakriti has 1.6±0.083 mm, Pittakapha prakriti has 2.313±1.5 mm, Samadhatuja Prakriti has 2.0 ±0.189 mm.
RESULTS
Association between different body constitution (prakriti) and Distal Radial arterial diameter
Among 35 healthy volunteers 2 volunteers of vataja prakriti had average diameter of 0.14cm, 4 volunteers pittaja prakriti had average diameter of 0.57cm, 4 volunteers kaphaja prakriti had average diameter of 0.15cm, 4 volunteers vatapittaja prakriti had average diameter of 0.41cm, 9 volunteers vatapittaja prakriti had average diameter of 0.16cm, 8 volunteers pittakaphaja prakriti had average diameter of 0.23cm, 4 volunteers samadhatuja prakriti had average diameter of 0.17cm. (Table 3).
The Pearson chi-square test of independence for analysing the association between palpatory blood vessel consistency type and arterial diameter on USG is 0.35 with degree of freedom 180 at 5% level of significance. The obtained chi-square value is less than the α-value, hence shows significant results. Thus rejecting the null hypothesis. This shows there is association between the body constitution ( prakriti ) and distal radial arterial luminal diameter on USG (Fig. 1)
Association between Prakriti and IMT(intima media thickness) of distal radial artery
A mong 35 healthy volunteers, 2 volunteers of vataja prakriti had an average IMT of 0.05mm, 4 volunteers pittaja prakriti had an average IMT of 0.03mm, 4 volunteers kaphaja prakriti had an average IMT of 0.05mm, 4 volunteers vatapittaja prakriti had an average IMT of 0.1mm, 9 volunteers vatakaphaja prakriti had an average IMT of 0.08mm, 8 volunteers pittakaphaja prakriti had an average IMT of 0.03mm, 4 volunteers samadhatuja prakrati had average IMT of 0.03mm. (Table 4)
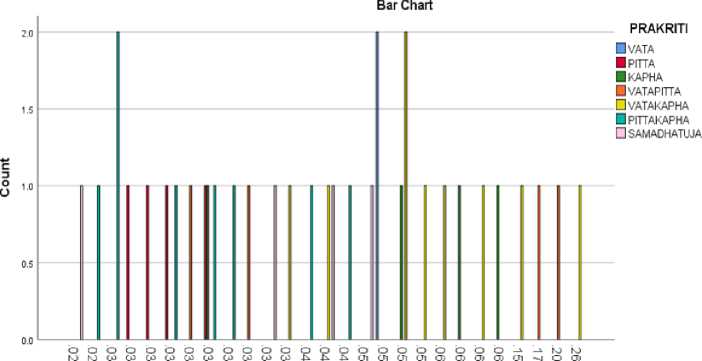
The Pearson chi-square test of independence for analysing the association between palpatory blood vessel consistency type and arterial diameter on USG is 0.153 with degree of freedom 156 at 5% level of significance. The obtained chi-square value is less than the α-value, hence shows significant results. Thus rejecting the null hypothesis. This shows there is association between the prakriti type and arterial intima media thickness (IMT) in USG (Fig.2)
Co-relation between luminal diameter (LD) and intima medial thickness (IMT) of distal radial artery.
Pearsons’s Co-relation shows low positive corelation (r = 0.254) between the luminal diameter (LD) and intima medial thickness (IMT) of distal radial artery. Testing difference between and within the groups:
A one-way ANOVA revealed that there was not a statistically significant difference in [luminal diameter of DRA] between at least two groups of F [between groups df(degree of freedom) =6, within groups df= 28 ] = [F-1.099, p = 0.05). The one-way ANOVA for IMT of DRA revealed that there was not a statistically significant difference in [ IMT of DRA] between the at least two groups F (between groups df =26, within groups df= 32 ) = [F- 2.919, p = 0.05). Thus One way ANOVA shows no difference seen in LD, IMT of distal radial artery with different prakriti .
Table. 1. Prakriti evaluation questionnaire (Rastogi, 2012)
|
Body Constitution |
|||
|
Vata d ominant |
Pitta dominant |
Kapha dominant |
|
|
Inspection ( Darshana Pariksha ) |
1.Emaciated,
3.Cracked skin
|
|
|
|
Palpation ( Sparshana Pariksha ) |
|
|
|
|
Interrogation ( Prashna Pariksha ) |
15.Talkative
19.Restless
|
|
18.Determined
|
Table 2. Distribution of volunteer’s in different body constitution ( prakriti )
|
Body constitution(prakriti) |
No. of volunteers |
Mean LD* ±SD# |
Mean IMT˥ ±SD |
|
Vata prakrati |
2 |
1.450±0.049 mm |
0.050±0.000 mm |
|
Pitta prakrati |
4 |
1.750±0.010 mm |
0.030±0.000 mm |
|
Kapha prakriti |
4 |
1.700±0.030 mm |
0.050±0.014 mm |
|
Vatapitta prakrati |
4 |
4.150±0.048 mm |
0.107±0.090 mm |
|
Vatakapha prakriti |
9 |
1.600±0.083 mm |
0.830±0.070 mm |
|
Pittakapha prakriti |
8 |
2.313±1.500 mm |
0.313±0.006 mm |
|
Samadhatuja prakriti |
4 |
2.000±0.189 mm |
0.350±0.012 mm |
*LD-luminal Diameter, #-S.D- standard deviation, ˥- IMT-intima-media thickness
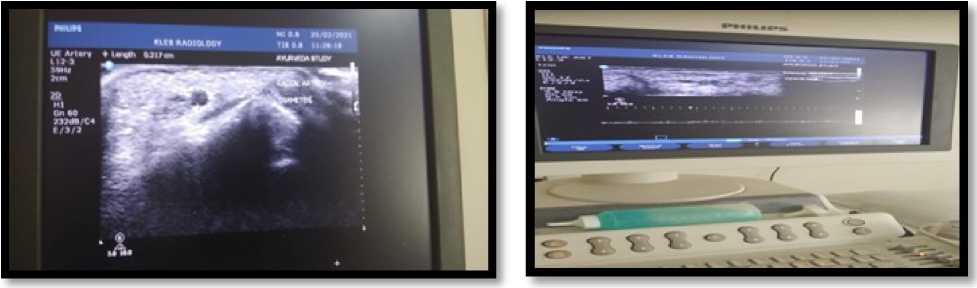
Figure1. USG distal radial artery
Table 3. Chi-square test to check the association b/w Prakriti and LD.
|
Value |
Df |
Asymptotic Significance (2-sided) |
|
|
Pearson Chi-Square |
186.991a |
180 |
0.345 |
|
Likelihood Ratio |
121.281 |
180 |
1.000 |
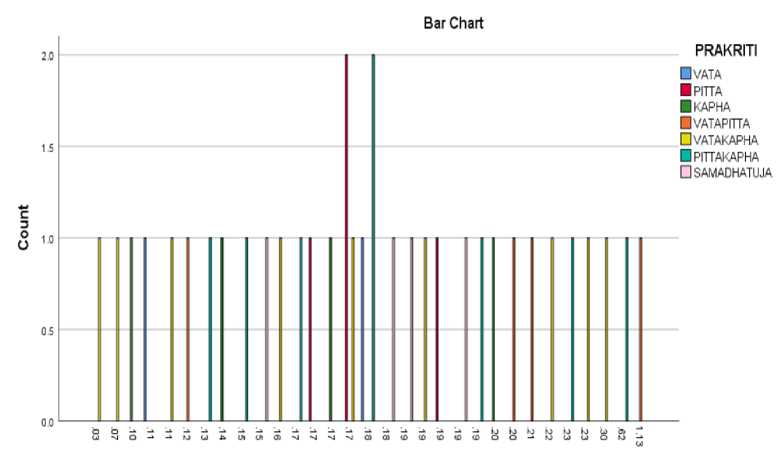
Graph 1 : Association b/w Prakriti and LD.
Table 4. Chi-square test to check the association b/w Prakriti and IMT
|
Value |
df |
Asymptotic Significance (2-sided) |
|
|
Pearson Chi-Square |
174.109a |
156 |
0.153 |
|
Likelihood Ratio |
112.963 |
156 |
0.996 |
∆ Intima media thickness
VAR00004
Graph 2: Association b/w Prakriti and IMT
DISCUSSION
In the present study, distal radial artery dimensions were observed using B–mode ultrasonography. The correlation of luminal diameter (LD) and intimae media thickness (IMT) of the artery was studied and further, the association between body constitution (Prakriti) and DRA luminal diameter (LD) and intima-media thickness (IMT) was analysed in this study. Earlier studies by Norimastu et al. (2019) on measurement of distal radial artery (DRA) with ultrasonography stated that the distal radial artery (DRA) vessel diameter in the anatomical snuffbox (2.6 ± 0.5 mm) was significantly smaller than that of the proximal radial artery (PRA) which is the conventional puncture site (3.1 ± 0.4 mm) of the radial artery (Norimatsu et al., 2019). Some difference in vessel luminal diameter between the DRA and PRA was 0.5 ± 0.4 mm, and the DRA/PRA ratio was 0.8 ± 0.1. Although the vessel diameter of the DRA was positively correlated with that of the PRA (r = 0.66, p < 0.0001). Takayuki et al 2019 studied the ultrasonography of the distal radial artery (DRA) on male and female volunteers before angiography on 120 patients. In male patients, the conventional puncture (CRA) site of the radial artery had diameters of 2.62 ± 0.60 mm and DRA was 2.04 ± 0.43 mm. In females, these diameters at CRA were 2.44 ± 0.51 mm and DRA was 1.96 ± 0.44 mm (Takayuki et al., 2019).
Tarif et al. (2010) studied the size of the radial artery with a mean diameter of the right artery of 2.3±0.4mm and a left radial artery was 2.2±0.4mm. The factors which influence the size of radial artery dimensions like male sex, diabetes mellitus, and smoking were enlisted. The other factors like body size parameters height, weight, body mass index have low positive correlation with the radial arterial dimensions (r=0.28, r-= 0.07, r=0.30) respectively (Tarif et al., 2010). The present study focuses on the association between the body constitution and IMT, LD of the Distal Radial artery. The mean luminal diameter observed in vataja Prakriti with small and narrow blood vessel (alpa) was smaller (1.450 ± 0.495 mm) than the pittaja body constitution with medium blood vessel diameter (2.050±0.1mm), kaphaja constitution with broad blood vessel lumen didn’t show marked results (2.0± 0.3mm). Among all the vatapittaja body constitution had a more luminal diameter of 4.15±0.47mm, vatakaphaja body constitution was 1.64±0.83mm, pittakaphaja constitution was 2.3±0.15mm and samadhatuja constitution had 1.8±0.189mm.
The mean intima-media thickness (IMT) in vataja body constitution which is believed to have narrow blood vessels had 0.05±0 mm of thickness, pittaja body constitution with soft elastic blood vessels had IMT of 0.03±0 mm, kaphaja constitution with thick elastic blood vessel had thicker IMT of 0.05± 0.014 mm, v atapittaja body constitution had 0.107±0.09 mm, vatakaphaja body constitution had 0.83±0.07 mm, p ittakaphaja constitution was 0.313±0.006 mm and samadhatuja constitution had 0.350±0.012 mm. Among the observed values, the vatakaphaja body constitution was 0.83±0.07 mm had increased thickness. Earlier studies have shown that obese volunteers had increased IMT and decreased pulse wave velocity as felt in kaphaja naadi (pulse) (Dangardt, 2008). The One-way ANOVA has shown no significant difference in luminal diameter, IMT of DRA in different prakriti. But as per the observation the values of F (ANOVA) for IMT are nearing significance, which shows that there may be some difference seen in IMT of distal radial artery between the prakriti. Thus the further scope of study is to conduct the same study with more sample size.
CONCLUSION
The study had observed that high resolution ultrasonography is the convenient tool that can be adapted to study the IMT and LD of the distal radial artery. Further the observations have shown that vatapittaja body constitution had more luminal diameter of 4.15±0.47mm, v atakaphaja body constitution was 0.83±0.07mm had increased intimae media thickness (IMT) One way ANOVA shows prakiti (body constitution of an individual) had a no significant role in judging the luminal diameter, intima-media thickness of the distal radial. As per the observations of the present study, there is a scope of difference of IMT (intima-media thickness) between the prakriti , which can be further scope of study with more sample size.
CONFLICTS OF INTEREST
The authors declare that they have no potential conflicts of interest.
References Distal radial artery dimensions in different body constitutions (prakriti)- an observational study
- Bhushan, P., Kalpana J., and Arvind C. (2005). Classification of human population based on HLA gene polymorphism and the concept of Prakriti in Ayurveda. J. Altern. Complement Med. 11, 349353.
- Dangardt F., (2008). Obese children show increased intimal wall thickness and decreased pulse wave velocity. Clin Physiol Funct Imaging. 28, 287-293
- Dey S., Pahwa P., (2014). Prakriti and its association with metabolism, chrionic diseases, and genotypes: possibilities of new born. Journal of Ayurveda integrative medicine. 5(1), 15-24.
- Ghodke Y., Joshi K., Patwardhan B., (2011). Traditional Medicine to Modern Pharmacogenomics: ayurveda Prakriti type and CYTP2c19 Gene Polymorphism associated with the metabolic variability, Hindawi Publishing Corporation Evidence based complementary and alternative medicine, 1, 5.
- Govindaraj P., Nizamuddin S., Sharath A., et al. (2015). Genome-wide analysis correlates Ayurveda Prakriti. Scientific Reports, 5, 15786
- Juyal R., et al. (2012). Potential of ayurgenomics approach in complex trait research: leads from a pilot study on rheumatoid arthritis. PloS. one. 7, pp.45752
- Mahalle N., Kulkarni M., (2012). Association of constitutional type of ayurveda with cardiovascular risk factors, inflammatory markers and insulin resistance. Journal of Ayurveda integrative medicine. 3, 150-157
- Murthy K. (1997). "Examination of Pulse" in Sarngadhara- Samhita: A Treatise on Ayurveda. Chaukhamba Orientalia Press, New Delhi, 14-16.
- Norimatsu K., Kusumoto T., Yoshimoto K., Tsukamoto M., Kuwano T., Nishikawa H., Matsumura T., (2019). Importance of measurement of the diameter of the distal radial artery in a distal radial approach from the anatomical snuffbox before coronary catheterization. SI. Heart Vessels. 34(10), 1615-1620.
- Pandey R. (2019). A complete Treatise on Ayurveda Yogaratnakara- Priyasiddida Hindi commentary. Chaukhambha Vishvabharati Press, Varanasi, 810.
- Rastogi S., (2012). Development and validation of prototype Prakriti Analysis Tool (PPAT): inferences from a pilot study, Ayu. 33(2), 209-218
- Rotti H., et al. (2014). Immunophenotyping of normal individuals classified on the basis of human dosha prakriti. Journal Ayurveda Integr. Med. 5, 43-49.
- Rotti, H. et al. (2014a). Determinants of prakriti, the human constitution types of Indian traditional medicine and its correlation with contemporary science. Journal of Ayurveda Integr. Med. 5, 167-175
- Shirodkar J., Mehmod S., (2014). Anguli Parimana in ayurveda and its association with adiposity and diabetes, Journal of Ayurveda Integr. Med. 5(3), 177-184
- Takayuki N., Takayuki S., Kota S., Kazutaka I., Sachiko S., Keiko Y., Haruna S., Maki S., Emiko Okamura., Takashi H., and Fuminobu Y. (2019). Evaluation of the diameter of the distal radial artery at the anatomical snuff box using ultrasound in Japanese patients. European pub. 7, 312-316.
- Tariq A., Panhwar Z., Sultana H., (2010). Size of radial and ulnar artery in local population. Journal of Pak Med Association. 60(10), 817-9.
