Factors of cancer diagnosed family and medical system for delay in diagnosis and treatment of esophageal cancer

Author: Majeed Khan I., Hussain M., Latif A., Sarwar A.
Journal: Сибирский онкологический журнал @siboncoj
Section: Опыт работы онкологических учреждений
Article in issue: 3 т.23, 2024.
Free access
Introduction. The esophagus cancer patients needs early diagnosis to achieve better prognosis. The delay barriers increase progression of diseases to higher stages. The aim of work was to identify and explore the barriers in diagnosis of esophagus cancer and chart the time duration in this process. Material and Methods. The study was conducted in Jinnah Hospital Lahore (JHL), a teaching care hospital of Allama Iqbal Medical College, during a period of one year from July 2019 to July 2020. There were 49.42 % female and 50.57 % male patients.
Esophageal cancer, late diagnosis, cancer alertness
Short address: https://sciup.org/140305916
IDR: 140305916 | UDC: 616.329-006.6-07 | DOI: 10.21294/1814-4861-2024-23-3-106-114
Влияние социального статуса больного и организации системы здравоохранения на задержку диагностики и начала лечения рака пищевода
Введение. Выявление рака пищевода на ранней стадии позволяет добиться благоприятного прогноза. Причины, препятствующие ранней диагностике рака, ускоряют прогрессирование заболевания. Цель исследования - изучить причины несвоевременной диагностики рака пищевода и составить график продолжительности этого процесса. материал и методы. Исследование проводилось в больнице имени Джинна, Лахор, в больнице Медицинского колледжа Аллама Икбал, с июля 2019 по июль 2020 г. Среди пациентов было 49,42 % женщин и 50,57 % мужчин.
Text of the scientific article Factors of cancer diagnosed family and medical system for delay in diagnosis and treatment of esophageal cancer
Esophageal cancer impacts around 450000 men over the world and the rate of incidence is growing rapidly. Esophageal cancer demonstrates an epidemiologic pattern discrete from all other malignancies. Cancer grows with time and its early detection is crucial for curative treatment. Delays in diagnosis and treatment of cancer and lead to high mortality of cancer patients [1–12]. For SCC, transition models have defined squamous epithelium suffering inflammatory fluctuations that develop the changes lead to malignancy [13]. On the other hand, most adenocarcinomas form in the distal esophagus from columnar-lined metaplastic epithelium, usually known as Barrett esophagus, which switches the squamous epithelium to dysplasia. Barrett esophagus is caused by GERD (gastro-esophageal reflux disease), which damages the outer layer of the esophagus [13–14]. SCC of esophagus is the well recognized type of worldwide. The overall rate rises as people get older, peaking in the 1970 [14]. It is more familiar in black in comparison with white men. The main risk factors of SCC are heavy usage of alcohol [15]. The risk factor of esophageal adenocarcinoma may be impacted by esophageal metaplasia. The more extended the section of esophagus impacted the higher the risk of adenocarcinoma [16].
Related Work
-
F. Cavallin et al. has studied delay time to diagnosis on esophagus cancer patient. Total 3613 patients with esophageal were reported from 1980 to 2011. By raising the awareness of esophageal cancer among population and by providing the health care may have limited effect on clinical outcome [17].
351 patients with esophageal cancer were reported at the University of Medical Center, Utrecht from
2003–2014. The effect of delay time on a patient’s survival rate was investigated by constructing the short (<8 weeks) and long (≥8 weeks) delay times by E. Visser et al. [18].
Total 238 Patients with esophageal malignancy were enrolled in the Qilu hospital in 2007. In comparison with lower SES (socio economic status), Surgical resection was used less in the higher SES group. Patients with a higher SES had a great chance of receiving chemotherapy as compared to lower SES [19].
The effect of radiotherapy (RT) delay on patients with esophageal cancer had been examined on its survival rate by Y. Wang et al. Time duration between surgery and radiation therapy was investigated. Total 316 cases were included who received radiation therapy in 5 different hospitals in china [20].
-
E. Visser et al. studied the waiting time impact on survival of patients diagnosed with esophageal cancer. Out of 3839 patients: 2589 cases received multimodality treatment and 1250 cases were undergone surgery only. In both types of patients either treated by multimodality or surgery only, pN-status, pT-status, resection rates and overall survival were not significantly impact on waiting time [21].
The aim of work was to identify and explore the barriers in diagnosis of esophagus cancer and chart the time duration in this process.
Material and Methods
Data of 87 esophageal cancer patients has been collected in the Department of Radiation Oncology, Jinnah Hospital Lahore since January 2018 to May 2022.The main purpose of the study is how multiple factors affect the delay time to diagnose and treat the esophageal carcinoma patients. The clinical and personal data of the patients have been used in this study and it is collected directly from the files and by detailed interview of the patients (Table 1). The Table 1. shows that a total of 87 patients were reported with esophageal cancer during the time period from 2018–2022. Out of which 44 patients are male and 43 patients are female. Ages 40–60 are more affected by this disease. The table shows that socio-economic factors i.e. residential area, education, marital status and total household income significantly affect the cause of having esophageal cancer.
Data was carefully analyzed after taking the history of each patient. To analyze the data, many questions and files were viewed. Multiple factors and patient’s history were researched. Delay time is classified into four sorts of postponement: patient deferral, doctor delay, framework postponement and treatment delay. Patient postponement is characterized as time from appearance of the first side effect to the first visit to a specialist. Doctor delay is characterized as the time from first advisor to conclusion of esophageal disease. Reference delay, the time from first specialist to the first reference doctor, is considered as a piece of doctor delay. Framework delay is characterized as the time from biopsy to medical procedure, from medical procedure to chemotherapy or from medical procedure to radiation treatment. The time from determination of infection to beginning of treatment is characterized as treatment delay. All of this information was analyzed carefully and found out the total delay from 1st symptom shown to the beginning of medical process.
Results
Results have shown that socio-economic factors i.e. age, education, marital status, initial symptoms, active employment, residential area and total household income are the main factors that cause the delays. Barium swallow, endoscopy, biopsy and CT scan are used as diagnostic tests to locate the cancer cells.
After diagnosis, surgery was performed to remove the tumor of patients whose cancer is a primary cancer. Larger tumors are difficult to remove, so patients were 1st given Chemotherapy treatment in order to decrease the size of tumor. Then, surgery was performed. In the last, radiations were given by 60Co units. Radiotherapy helps to prevent the spread of cancer.
Total delay
Total delay from the 1st symptom shown to end of treatment is categorized into four steps from patient delay (PD) to Treatment delay (TD) with considering physician delay (Phy D) and system delay (SD).
Gender and age factor
It is seen that esophageal carcinoma is not a gender based cancer. Both males and females are almost affected equally. Age factor of the patients is very relatable to the cancer type because the immune system of the human body has gone weak with increasing the age factor. So, the ability of the body to fight against the cancer carcinogens is going to be slower with age. Results have been plotted by using origin software. Graph between patients age and delay is shown in Fig. 1. Different delay times re found for multiple age groups. Shortest delay time, mean 60 days, was found in the youngest patient (<20 years) and longest delay time, mean 135 days, was found at the age from 51–60 years. It is observed from the Table 2. as well as from the graph that physician delay, system delay and treatment delay was much less than patients delay.
Marital status related to cancer patients
The pattern observed by comparing married versus unmarried women shows minimum total delay in unmarried women (Fig. 2). However almost same physician, system and treatment delay were observed.
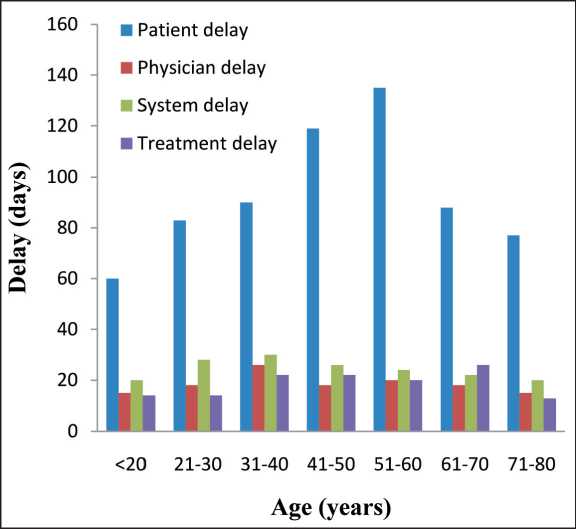
Fig. 1. Graph related the delay time with age. Note: created by the authors.
Рис. 1. Зависимость времени задержки от возраста пациента. Примечание: диаграмма выполнена авторами
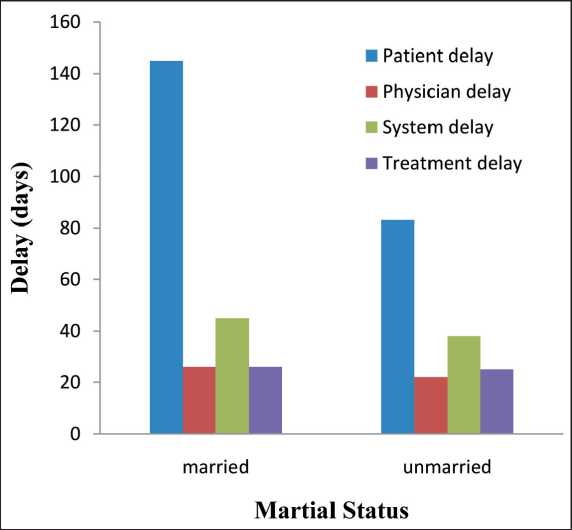
Fig. 2. Graph between marital status and delay time.
Note: created by the authors
Рис. 2. Зависимость времени задержки от семейного положения пациента. Примечание: диаграмма выполнена авторами
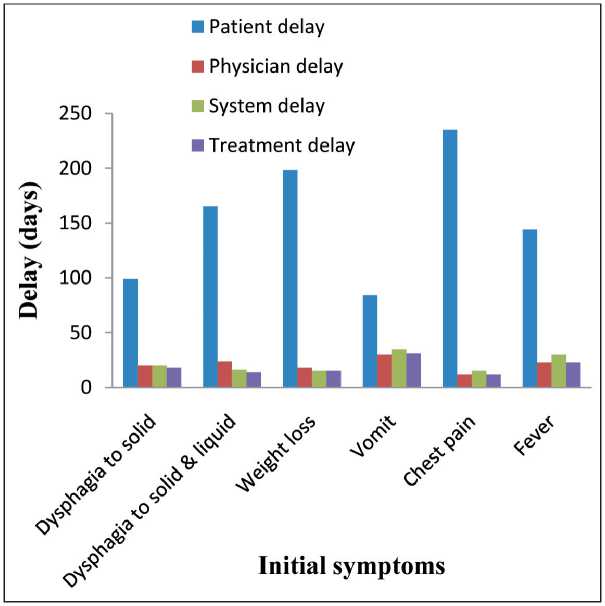
Fig. 3. Graph between initial symptoms and delay time. Note: created by the authors.
Рис. 3. Зависимость между начальными симптомами и временем задержки.
Примечание: диаграмма выполнена авторами
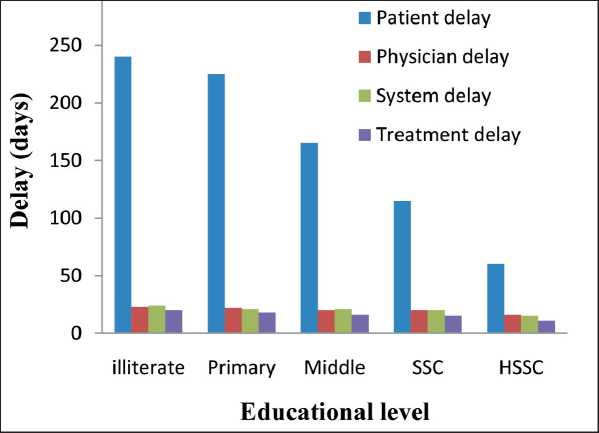
Fig. 4. Graph between educational level of patient and delay time. Note: created by the authors
Рис. 4. Зависимость времени задержки от уровня образования пациента. Примечание: диаграмма выполнена авторами
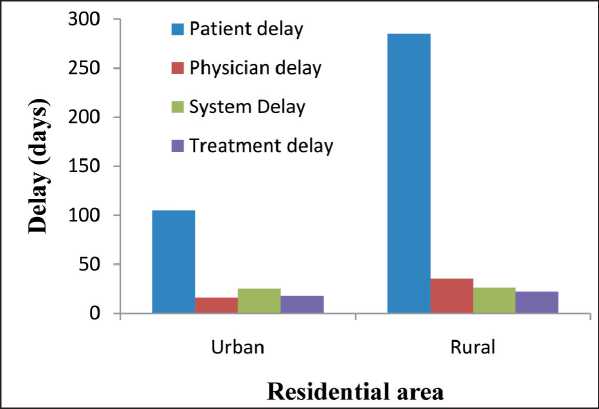
Fig. 5. Graph between area of residence and delay time. Note: created by the authors
Рис. 5. Зависимость времени задержки от места проживания пациента. Примечание: диаграмма выполнена авторами
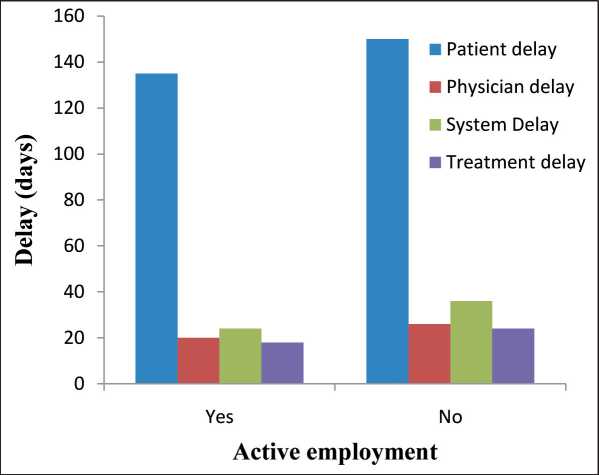
Fig. 6. Graph between active employees and delay time. Note: created by the authors
Рис. 6. Зависимость времени задержки от вида рабочей занятости пациента. Примечание: диаграмма выполнена авторами
It has been observed that patient delay significantly affects the diagnosis of this disease. Married patients remains unable to work for a diagnosis although they suspect to initial symptoms because they have not enough time to visit the Doctor regularly.
Initial symptoms related to esophageal cancer
Initial symptoms i.e. dysphagia, weight loss, heartburn and chest pain are faced by almost all patients. Most of the patients experience chest pain. Patients were ignoring the very initial symptoms like chest pain, fever for about 2–3 months (Fig. 3). When they experience the heavy dysphagia to solid and liquid, then they visit the referral physician. It has been observed that only patient delay causes an advanced stage of cancer.
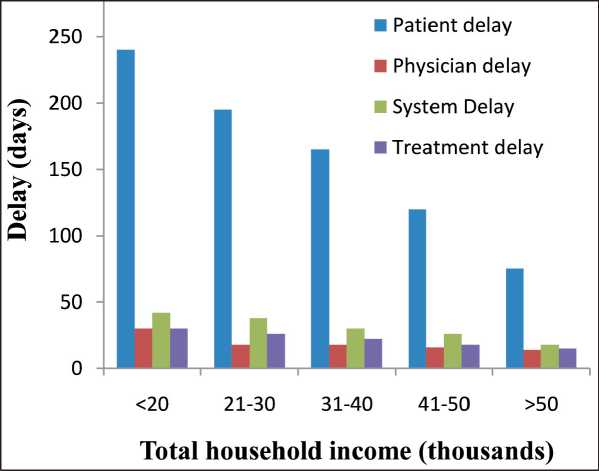
Рис. 7. Зависимость времени задержки от ежемесячного дохода семьи. Примечание: диаграмма выполнена авторами
Educational importance in cancer diagnosis
The research emphasis the importance of education in early diagnosis and treatment of cancer. Educated patients showed a short delay in diagnosis of cancer compared with less educated and illiterate people. The graph between educational level and delay time has been given in Fig. 4. It has been also observed from the graph that educated patients saw system delay and physician delay as compared with illiterate patients.
Residential area of cancer patients
The majority of population of Pakistanis lives in rural areas. Rural areas are usually not well aware of major diseases. The rural people also have to travel long distances to see a medical person (Fig. 5). It is also observed from the graph that urban residents come
to minimum system and physician delay as compared with rural residents. But overall, the graph shows the longer patient delay as compared with others.
Active employees
There is not such a huge difference found in active and non-active working patients. Both have almost equal delays. Active employment makes cancer patients unable to attend a medical facility due their duties. Non-working patients who are dependents on their families do not get examined at the initial stages due to their financial problems (Fig. 6).
Total household income
The total household income is an important factor in early diagnosis and treatment of cancer. The graph between monthly household income and delay factors
table 1/Таблица 1
characteristics of esophageal cancer patients, 2018–2022Характеристика больных раком пищевода, 2018–2022 гг.
|
Factors/Факторы |
Frequency/ Частота |
|
Total patients/Всего больных |
87 |
|
Gender/Пол |
|
|
Male/Муж |
44 (50.6 %) |
|
Female/Жен |
43 (49.4 %) |
|
Age, years/Возраст, лет |
|
|
<20 |
1 (1.1 %) |
|
21–30 |
6 (6.9 %) |
|
31–40 |
14 (16.1 %) |
|
41–50 |
25 (28.7 %) |
|
51–60 |
26 (29.9 %) |
|
61–70 |
11 (12.6 %) |
|
71–80 |
4 (4.6 %) |
|
Status/Семейное положение |
|
|
Married/Женатый, замужем |
83 (95.4 %) |
|
Unmarried/Неженатый, не замужем |
4 (4.6 %) |
|
Initial symptoms/Первоначальные симптомы |
|
|
Dysphagia to solid/ Дисфагия при приеме твердой пищи |
12 (13.8 %) |
|
Dysphagia to liquid/ Дисфагия при приеме жидкой пищи |
33 (37.9 %) |
|
Weight loss/Потеря веса |
55 (63.2 %) |
|
Vomit/Рвота |
9 (10.3 %) |
|
Chest pain/Боль в груди |
80 (91.9 %) |
|
Fever/Гипертермия |
26 (29.9 %) |
|
Education/Образование |
|
|
Illiterate/Неграмотный |
26 (29.9 %) |
|
Primary/Начальное образование |
22 (25.3 %) |
|
Middle/Среднее образование |
25 (28.7 %) |
|
SSC/Аттестат о среднем образовании |
11 (12.6 %) |
|
HSSC/Аттестат о полном среднем образовании |
3 (3.4 %) |
|
Residential area/Место проживания |
|
|
Urban/Город |
18 (20.7 %) |
|
Rural/Сельская местность |
69 (79.3 %) |
|
Active employment/Работа |
|
|
Yes/Да |
44 (50.6 %) |
|
No/Нет |
43 (49.4 %) |
Примечание: таблица составлена авторами.
|
Factors/Факторы |
Frequency/ Частота |
|
Monthly household income/Ежемесячный доход |
|
|
<20,000 |
18 (20.6 %) |
|
20,000–30,000 |
27 (31.0 %) |
|
31,000–40,000 |
30 (34.4 %) |
|
41,000–50,000 |
10 (11.5 %) |
|
>50,000 |
2 (2.3%) |
|
Histological type/Гистологический |
тип |
|
SCC/Плоскоклеточный рак |
78 (89.7 %) |
|
Adenocarcinoma/Аденокарцинома |
9 (10.3 %) |
|
Grade of the tumor/Степень дифференцировки |
|
|
Well defined/ Высокодифференцированный рак |
23 (26.4 %) |
|
Moderately defined/ Умеренно дифференцированный рак |
35 (40.2 %) |
|
Poorly defined/ Низкодифференцированный рак |
22 (25.3 %) |
|
Not defined/ Недифференцированный рак |
7 (80.5 %) |
|
Family history/Семейный анамнез |
|
|
Yes/Да |
32 (36.8 %) |
|
No/Нет |
55 (63.2 %) |
|
Diagnostic techniques/Методы диагностики |
|
|
Barium swallow/Рентгенография с барием |
5 (5.7 %) |
|
Endoscopy/Эндоскопия |
78 (89.7 %) |
|
Biopsy/Биопсия |
67 (77.0 %) |
|
CT scan/КТ |
87 (100 %) |
|
MRI/МРТ |
1 (1.1 %) |
|
Treatment techniques/Методы лечения |
|
|
Surgery/Операция |
73 (83.9 %) |
|
Chemotherapy/Химиотерапия |
81 (93.1 %) |
|
Radiotherapy/Лучевая терапия |
87 (100.0 %) |
|
Combination of therapies/ Комбинированное лечение |
81 (93.1 %) |
Note: created by the authors.
table 2/Таблица 2
Примечание: таблица составлена авторами.
table 3/Таблица 3 correlation between selected factors and total delay
Корреляция между отдельными факторами и общей задержкой диагностики
|
Factor/Фактор |
Correlation (r)/Корреляция |
р-value |
|
Initial symptoms/Первоначальные симптомы |
0.94 |
0.004 |
|
Education/Уровень образования |
0.91 |
0.029 |
|
Income per month/Доход в месяц |
0.65 |
0.22 |
|
Age/Возраст |
0.96 |
0.0004 |
Note: created by the authors.
Примечание: таблица составлена авторами.
is shown in Fig. 7. It has been observed that monthly income less than 20,000 has the longest patient, physician and system delay because they have not resources to manage the cost of medical care.
Statistical Analysis to correlateFactors with Delay
The multiple factors involved in research are statistically correlated with total delay. Their significance is checked by calculation p-value and their results are presented in table below.
Discussion
Esophageal cancer is the 8th most common malignant disease and the 6th most frequent cause of malignancy related death around the world. A coherent study from Indian cancer society was reported that the mean delay from the first symptoms to diagnosis was 14.9 weeks. 82 % delay was due to the patients, 7 % was due to endoscopy and 11 % was due to histological diagnosis [22]. As the majority delay time showed patient delay which caused the high molarity rate.
In China, the mortality rate of esophageal carcinoma has decreased as socio-economic status has improved over the past 30 years [23]. However, esophageal cancer remains dominant in rural areas which cause an increase in molarity rate. In Pakistan, the mortality rate of esophageal cancer is 6541 per year [24]. The incident and mortality rate increases due to the unavailability of proper health care centers. Our research points out the same results as the majority delay time was due to illiterate and rural residents. The study is conducted at the Department of Radiation Oncology, Jinnah Hospital Lahore from January 2019 to September 2021.
This study has shown that esophageal cancer patients experienced considerable pre-hospital and hospital delays, which contributes to Pakistan's high mortality rate. Despite the fact that there have been few studies on the causes of diagnosis delays in Pakistan, it is essential to investigate this issue.
References Factors of cancer diagnosed family and medical system for delay in diagnosis and treatment of esophageal cancer
- Enzinger P.C., Mayer R.J. Esophageal cancer. N Engl J Med. 2003; 349(23): 2241-52. https://doi.org/10.1056/NEJMra035010.
- Bailar J.C. 3rd, Gornik H.L. Cancer undefeated. N Engl J Med. 1997; 336(22): 1569-74. https://doi.org/10.1056/NEJM199705293362206.
- Majeed I., Ammanuallah R., Anwar A.W., Rafique H.M., Imran F. Diagnostic and treatment delays in breast cancer in association with multiple factors in Pakistan. East Mediterr Health J. 2021; 27(1): 23-32. https://doi.org/10.26719/emhj.20.051.
- Short M.W., Burgers K.G., Fry V.T. Esophageal Cancer. Am Fam Physician. 2017; 95(1): 22-8.
- Majeed I., Rana A., Rafique M., Waheed Anwar A., Mahmood F. Time delay barriers in diagnosis and treatment of cancer. WCRJ. 2018; 5(3). https://doi.org/10.32113/wcrj_20189_1118.
- Kamangar F., Chow W.H., Abnet C., Dawsey S. Environmental causes of esophageal cancer. Gastroenterol Clin North Am. 2009; 38(1). https://doi.org/10.1016/j.gtc.2009.01.004.
- Wu S.G., Zhang W.W., Sun J.Y., Li F.Y., Lin Q., He Z.Yu. Patterns of distant metastasis between histological types in esophageal cancer. Front Oncol. 2018; 8: 302. https://doi.org/10.3389/fonc.2018.00302.
- Eslick G.D. Esophageal cancer: a historical perspective. Gastroenterology Clinics of North America. 2009; 38(1): 1-15. https://doi.org/10.1016/j.gtc.2009.01.003.
- Fujita H. History of lymphadenectomy for esophageal cancer and the future prospects for esophageal cancer surgery. Surg Today. 2015; 45(2): 140-9. https://doi.org/10.1007/s00595-014-0841-4.
- Chen T., Cheng H., Chen X., Yuan Z., Yang X., Zhuang M., Lu M., Jin L., Ye W. Family history of esophageal cancer increases the risk of esophageal squamous cell carcinoma. Sci Rep. 2015; 5. https://doi.org/10.1038/srep16038.
- Wada H., Doki Y., Nishioka K., Ishikawa O., Kabuto T., Yano M., Monden M., Imaoka, S. Clinical outcome of esophageal cancer patients with history of gastrectomy. J Surg Oncol. 2005; 89(2): 67-74. https://doi.org/10.1002/jso.20194.
- Blot W.J., McLaughlin J.K. The changing epidemiology of esophageal cancer. Semin Oncol. 1999; 26(5s15): 2-8.
- Holmes R.S., Vaughan T.L. Epidemiology and pathogenesis of esophageal cancer. Sem Radiat Oncol. 2007; 17(1): 2-9. https://doi.org/10.1016/j.semradonc.2006.09.003.
- Zhang Y. Epidemiology of esophageal cancer. World J Gastroenterol. 2013; 19(34): 5598-606. https://doi.org/10.3748/wjg.v19.i34.5598.
- Umar S.B., Fleischer D.E. Esophageal cancer: epidemiology, pathogenesis and prevention. Nat Clin Pract Gastroenterol Hepatol. 2008; 5(9): 517-26.
- Napier K.J., Scheerer M., Misra S. Esophageal cancer: A Review of epidemiology, pathogenesis, staging workup and treatment modalities. World J Gastrointest Oncol. 2014; 6(5): 112-20. https://doi.org/10.4251/wjgo.v6.i5.112.
- Cavallin F., Scarpa M., Cagol M., Alfieri R., Ruol A., Chiarion Sileni V., Rugge M., Ancona E., Castoro C. Time to diagnosis in esophageal cancer: a cohort study. Acta Oncol. 2018; 57(9): 1179-84. https://doi.org/10.1080/0284186X.2018.1457224.
- Visser E., Leeftink A.G., van Rossum P.S.N., Siesling S., van Hillegersberg R., Ruurda J.P. Waiting Time from Diagnosis to Treatment has no Impact on Survival in Patients with Esophageal Cancer. Ann Surg Oncol. 2016; 23(8): 2679-89. https://doi.org/10.1245/s10434-016-5191-6.
- Wang N., Cao F., Liu F., Jia Y., Wang J., Bao C., Wang X., Song Q., Tan B., Cheng Y. The effect of socioeconomic status on health-care delay and treatment of esophageal cancer. J Transl Med. 2015; 13. https://doi.org/10.1186/s12967-015-0579-9.
- Wang Yu., Guan S., Bi Ya., Lin S., Ma J., Xing Q., Liu C., Zhang R., Qu Z., Jiang P., Chen X., Cheng Yu. Survival Impact of Delaying Postoperative Radiotherapy in Patients with Esophageal Cancer. Transl Oncol. 2018; 11(6): 1358-63. https://doi.org/10.1016/j.tranon.2018.08.007.
- Visser E., van Rossum P.S., Leeftink A.G., Siesling S., van Hillegersberg R., Ruurda J.P. Impact of diagnosis-to-treatment waiting time on survival in esophageal cancer patients - A population-based study in The Netherlands. Eur J Surg Oncol. 2017; 43(2): 461-70. https://doi.org/10.1016/j.ejso.2016.10.017.
- Ganesan S., Sivagnanganesan S., Thulasingam M., Karunanithi G., R K., Ravichandran S., Saxena S.K., Ramasamy K. Diagnostic delay for head and neck cancer in South India: A Mixed-methods Study. Asian Pac J Cancer Prev. 2020; 21(6): 1673-8. https://doi.org/10.31557/APJCP.2020.21.6.1673.
- He F., Wang Ju., Liu L., Qin X., Wan Z., Li W., Ping Z. Esophageal cancer: trends in incidence and mortality in China from 2005 to 2015, Cancer Med. 2021; 10(5): 1839-47. https://doi.org/10.1002/cam4.3647.
- Qureshi S., Khan S., Quraishy M.S., Zaheer S. Esophageal cancer patient survival: A retrospective study from a tertiary care hospital in Pakistan. Pak J Med Sci. 2024; 40(5): 811-9. https://doi.org/10.12669/pjms.40.5.7582.
