Impact of Updated COVID-19 Methodological Guidelines on Case Detection and Management in India (Kerala and Tamil)
")
Author: Mamatkulova N., Adarsh Gopalakrishna Pillai, Ashique Sariful, Chavhal Gayatri Mahadeo
Journal: Бюллетень науки и практики @bulletennauki
Section: Медицинские науки
Article in issue: 2 т.12, 2026.
Free access
COVID-19 guidelines in India significantly influenced case finding, contact tracing, and clinical management. Kerala and Tamil Nadu, two states with strong public health systems, implemented modified strategies that resulted in distinct epidemiological outcomes. This article reviews the impact of updated guidelines nationally and at the state level, highlighting topics valuable for the undergraduate medical education system.
COVID-19, clinical management, Kerala, Tamil Nadu
Short address: https://sciup.org/14134451
IDR: 14134451 | UDC: 616.9-053.2-06 | DOI: 10.33619/2414-2948/123/39
Влияние обновленных методических рекомендаций по COVID-19 на выявление и лечение случаев заболевания в Индии (штаты Керала и Тамилнад)
В Индии рекомендации по борьбе с COVID-19 оказали значительное влияние на выявление случаев заболевания, наблюдение за больными и клиническое лечение. Керала и Тамилнад, два штата с развитыми системами здравоохранения, внедрили модифицированные стратегии, которые привели к различным эпидемиологическим результатам. В данной статье рассматривается влияние обновленных рекомендаций на национальном и региональном уровнях, освещаются вопросы, имеющие важное значение для системы медицинского образования студентов.
Text of the scientific article Impact of Updated COVID-19 Methodological Guidelines on Case Detection and Management in India (Kerala and Tamil)
Бюллетень науки и практики / Bulletin of Science and Practice
COVID-19 necessitates continuous updates on national guidelines for diagnosis, treatment, and public health response. Kerala and Tamil Nadu are showing good approaches in contact tracing, containment, and clinical care. Population context: Kerala – 35 million, Tamil Nadu – 72 million. Both states have high urban density, significant elderly populations, and large numbers of returning migrants. COVID-19 burden: high confirmed cases due to extensive testing. Relatively lower case fatality rates compared with many northern states (Figure 1, 2).
Methods
Both states tried their best to administer an effective implementation for the control of COVID-19. Both states also followed the narrative review of national guidelines (MoHFW, ICMR, AIIMS
COVID Task Force) and state guidelines (Kerala DHS, Tamil Nadu Health). This led to the most effective implementation and planning for the management of the pandemic.
Both states also included reviewed studies, government bulletins, and surveillance reports (2020–2024).
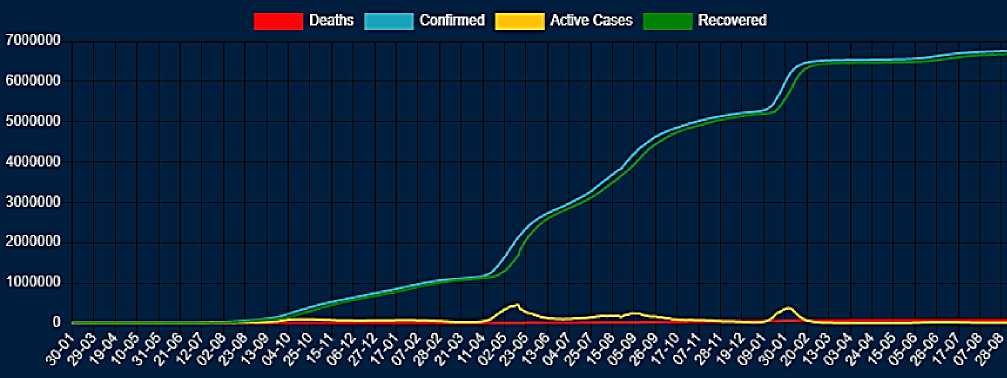
Fugure 1. Fatality rates compared
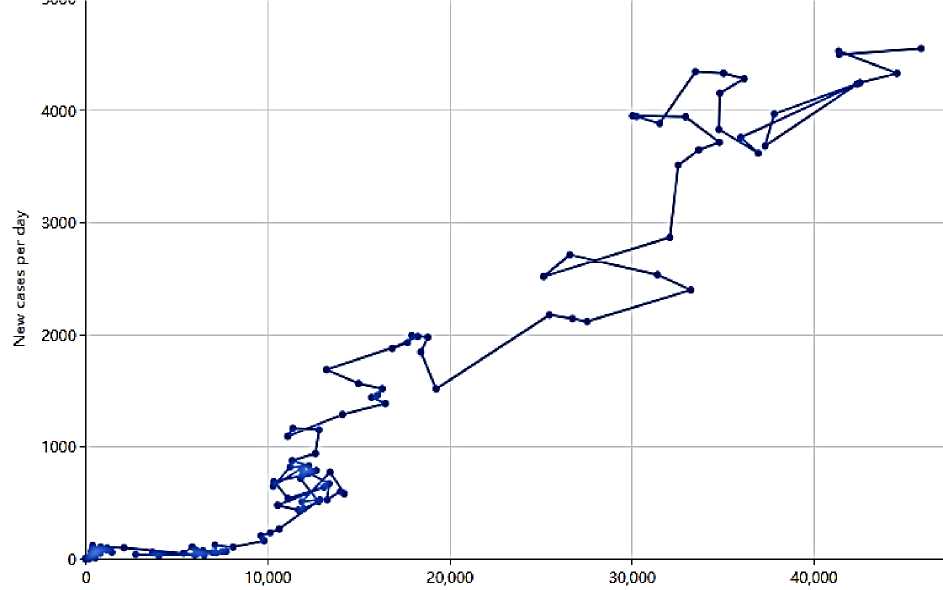
New tests per day
Fugure 2. COVID-19 Pandemic in Tamil Nadu
Results
National Case Detection was expanded to include RT-PCR and Rapid Antigen Testing, as well as home-testing kits for asymptomatic cases. INSACOG genomic surveillance was performed to monitor emerging variants (Delta, Omicron). Kerala-specific developments included a triple-lock mechanism for monitoring at the household, ward, and district levels. Aggressive contact tracing was conducted using ASHA workers and local field staff, and a high rate of testing per million population was achieved. This was well-executed and helped in the early detection of returning people from abroad, as Kerala reported the first case. Home isolation monitoring and telephone medicine support also played an important role in management.
Table MORBIDITY
|
Year |
Kerala |
Tamil nadu |
|
2019 |
0 |
0 |
|
2020 |
3073 |
12122 |
|
2021 |
44368 |
36612 |
|
2022 |
24219 |
60930 |
|
2023 |
403 |
38086 |
|
2024 |
76 |
405 |
|
2025 |
2 |
5 |
During the first phase and later waves, the situation was exacerbated due to population density and the return of migrants. Tamil Nadu-specific developments included ward-level fever camps in Chennai and other urban areas for early case detection, and COVID Care Centres (CCCs) were implemented for mild/asymptomatic patients. Telemedicine and district-level dashboards for realtime reporting were also very important. High early vaccination coverage and oxygen demand were managed using a real-time allocation system during the Delta wave, as there was a major oxygen shortage. Clinical Management included severity classification (mild, moderate, severe) based on SpO₂ and respiratory rate, which were used for medical triage and classification of affected patients. Limited use of hydroxychloroquine, ivermectin, and plasma therapy was implemented, with an emphasis on corticosteroids and anticoagulation.
Discussion
Kerala’s strength was its early preparedness; they were ready for what was coming. They implemented aggressive tracing, migrant management, and transparent communication. Tamil Nadu’s strengths include its triage efficiency, ward-level screening, and vaccination logistics. Challenges are variant surges, urban density, resource strain, and misinformation. Local adaptation of national guidelines enhances pandemic response and reduces mortality. We should also discuss why revisions were necessary after initial pandemic waves. The evolving nature of SARS-CoV-2 variants and clinical presentations caused major problems in solving the cases. Key updates in COVID-19 guidelines are as follows:
-
A) Changes in case definitions (suspected, probable, confirmed).
-
B) Modifications in testing methods such as RT-PCR, RAT, and pooled testing.
-
C) Algorithm for screening and triage in outpatient and emergency settings.
-
D) Protocols for monitoring mild, moderate, and severe classifications.
The main points we should discuss are the impact of clearer definitions on early detection and reporting, and the practical challenges in implementation at primary healthcare levels. We should also review case detection and surveillance methods, including a revised contact tracing approach, integration of digital tools, community surveillance, and core sites. We need to assess effectiveness in rural versus urban settings, as well as data quality challenges and the implications of underreporting. Furthermore, clinical management protocols are updated treatment guidelines, covering indications for antiviral therapy, corticosteroids, and anticoagulants; criteria for home isolation versus facility-based care; oxygen therapy protocols and escalation of care; comparison with WHO and NIH treatment recommendations; and implications for triage in resource-constrained settings.
On the other hand, the state-level experiences of Kerala and Tamil Nadu were noticeable.
In the case of Kerala, high testing rates and robust contact tracing were implemented, along with early adoption of home isolation protocols and the use of community health workers for followup. Whereas Tamil Nadu implemented large-scale population management and public health mobilization for case management.
Conclusion
Updated national COVID-19 guidelines improved case detection, clinical management, and public-health outcomes. Kerala and Tamil Nadu successfully implemented state-specific innovations alongside national guidance. Key takeaways for medical undergraduates: early detection, community engagement, structured triage, and integration of evidence-based policy with local adaptation. Both states did a magnificent job, and we should also remember the lives lost in this fight. One thing we can say for sure is that doctors and healthcare workers are the true superheroes of this world. This review provides strong evidence on how updated COVID-19 methodological guidelines were applied in real-world settings. For organizations such as the WHO, such state-level analyses are valuable in understanding how global recommendations translate into sub-national action. The experiences of Kerala and Tamil Nadu highlight practical strengths and limitations that can inform future policy. The study reflects how guideline-based communication influenced public behavior, testing uptake, and compliance with isolation measures. Such observations are useful for WHO and state health departments to improve risk communication, especially in addressing misinformation and public fatigue during health crises.
