Influence of socio-economic factors on the suicide type of behavior

Author: Molchanova Ekaterina Vladimirovna, Bazarova Ekaterina Nikolaevna
Journal: Economic and Social Changes: Facts, Trends, Forecast @volnc-esc-en
Section: Social development
Article in issue: 4 (16) т.4, 2011.
Free access
The given research was carried out for estimating the structure of suicide emotional frustration (by the example of Karelia Republic), in its interrelation with the socio-economic and climatic factors, so as to develop the algorithms of diagnosing and preventing this negative phenomenon. The clinical data of Petrozavodsk Republican Psychiatric Clinic’s patients, who made one or more suicide attempts within the last 5 years, served as the material for this research. By means of application of mathematical methods there were revealed the general features of the persons who had committed suicide and the factors influencing suicide behavior.
Suicide behavior, socio-economic factors and climatic factors, region
Short address: https://sciup.org/147223282
IDR: 147223282 | UDC: 314.424.2(470.22)
Text of the scientific article Influence of socio-economic factors on the suicide type of behavior
Ekaterina N.
BAZAROVA
Assistant Professor of Petrozavodsk State University psychiatrist of the highest category, a psychologist-psychoanalyst
According to the World Organization of Public Health Services (WOPHS), mental health is defined as a condition of well-being at which each person can realize his/her own potential, cope with usual vital stresses, productively and effectively work, and also bring some contribution to the life of the community [1]. In the middle of the twentieth century the problem of mental illnesses became one of the major one for the medical science and for the public health services of economically advanced countries.
Mental health is determined by socioeconomic, biological and ecological factors.
The World Organization of Public Health Services enumerates the basic determinants of mental health in its bulletin [2]:
-
1. Person’s mental health at each definite moment of time is determined by numerous social, psychological and biological factors. For instance, steady socio-economic pressure is considered to be a risk factor for mental health of separate people and communities. Evident facts are connected to the parameters of poverty, and to the low educational level of a person.
-
2. Mental health is also connected to fast social changes, stressful conditions at work, gender discrimination, social alienation, an unhealthy way of life, risks of violence, various illnesses, and also with infringements of human rights.
-
3. There are also specific psychological and personal factors which make people vulnerable for mental disorders. Finally, there are a number of biological reasons of mental disorders, including genetic factors and imbalance of chemical substances in a brain.
According to the experts’ opinions, by 2020 depression as a widespread phenomenon will rank second after ischemic illness of heart. Nowadays about half-billion people suffer from depression. Steady despondency and loss of interest to life alongside with psychological, behavioral and physical symptoms are characteristic for depression. It is one of the principal causes of physical inability of people all over the world. The increase of suicides’ number takes place in connection with the fast growth of depression in the world.
It is necessary to pay attention to two important features of the definition of suicide. Suicide can be defined as both the conscious actions resulted in death, and the actions which led to the attempt of deprivation of life, but by virtue of circumstances didn’t lead to a fatal end.
According to the data of the World Organization of Public Health Services, on the average, annually about 800 000 people commit suicide, 86 % of them commit suicide in the countries with a low and an average level of the income. More than a half of self-murderers are of age from 15 to 44 years old. The highest parameters of suicides are registered among the man’s population of the countries in the Eastern Europe. Mental disorders are one of the suicides’ reasons which can be treated rather successfully [1].
For the comparative analysis of suicides’ frequency in different countries the parameter “suicides’ level” is used, it shows the number of the committed suicides for 100 thousand people. In the beginning of 2000 the average world-wide parameter was 14 or 15 cases. Among the countries, which inform the World Organization of Public Health Services about the quantity of suicides, the highest parameters of “suicides’ level” are observed in the countries of the Eastern Europe, and the lowest ones are observed in the Muslim countries.
Russia is included into the number of the countries which occupy the leading position according to the number of suicides. The parameters on suicides in Russia 3 or 4 times exceed the average world-wide parameter (from 10 to 20 cases for 100 thousand people) (tab. 1) [3].
Karelia Republic is one of problem regions in the Russian Federation according to the parameters of death-rate, life expectancy and diseases.
Table 1. Description of the countries according to the death rate from suicides in 2006
|
Country |
Death rate from suicides (for 100 thousand people) |
Life expectancy at birth (years) |
The general death rate (for 1 000 people) |
GNP per head (in USA $) |
|
Countries with the high level of suicides |
||||
|
Lithuania |
28.94 |
71.16 |
13.2 |
8410 |
|
Russia |
27.63 |
66.67 |
15.21 |
5810 |
|
Kazakhstan |
27.27 |
66.18 |
10.27 |
3860 |
|
Slovenia |
22.79 |
78.35 |
9.05 |
19560 |
|
Hungary |
21.77 |
73.57 |
13.07 |
11020 |
|
Countries with the low level of suicides |
||||
|
Cyprus |
2.39 |
80.59 |
6.65 |
22880 |
|
Greece |
3.05 |
79.79 |
9.42 |
23650 |
|
Italy |
5.15 |
81.58 |
9.48 |
32190 |
|
Israel |
5.65 |
80.68 |
5.47 |
21020 |
|
Malta |
6.04 |
79.59 |
7.91 |
15160 |
The negative tendencies found their reflection in the high level of the fixed suicides, which on the average exceeds the all-Russian parameter for 25% (fig. 1) . In 2009 in the structure of the death-rate reasons among the Russia’s population suicides made about 2 %, they are prevailing among the external reasons of death (tab. 2) [4, 5].
A very high level of suicides in the postSoviet Russia, as well as in some other ex-socialist countries, is one of the parameters of difficulties characteristic for the transitive economic period. Scientists state the following factors, influencing the suicides’ level [6 – 10]:
-
- characteristics of sex and age,
-
- time parameters,
-
- social features,
-
- influence of taking alcohol and drugs,
-
- easy access to the specific means of suicide,
-
- influence of the quality of life,
-
- influence of the ethnic characteristic.
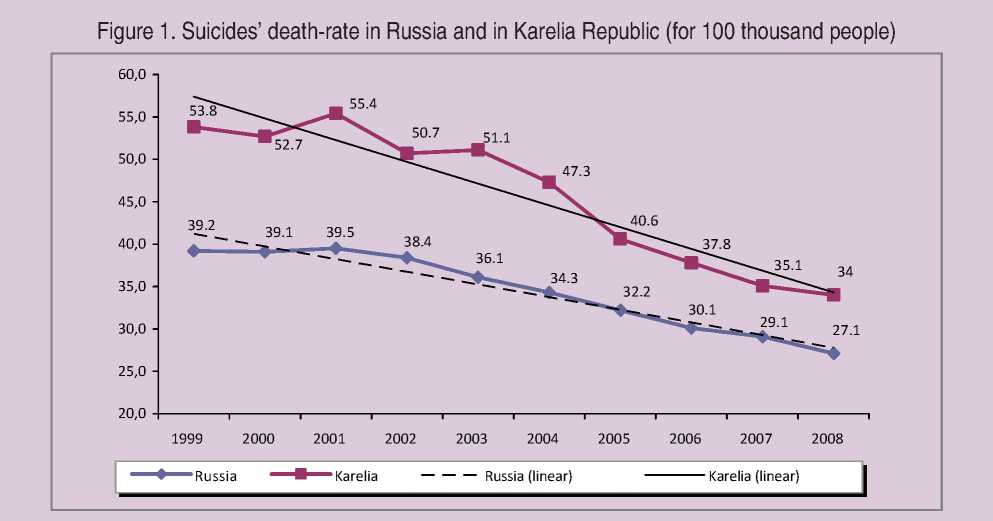
Table 2. Structure of the causes of death among the population of the Russian Federation (for 100 thousand people)
|
Cause of death |
2005 |
2006 |
2007 |
2008 |
2009 |
|
The number of people who died of different causes, for 100 thousand people |
1609.9 |
1520.6 |
1463.9 |
1462.4 |
1416.8 |
|
Of them: Some infectious and parasitic diseases |
27.2 |
25.1 |
24.2 |
24.3 |
24.0 |
|
Cancer |
201.2 |
200.9 |
203.0 |
203.8 |
206.9 |
|
Circulatory system illnesses |
908.0 |
864.7 |
833.9 |
835.5 |
801.0 |
|
Respiratory system illnesses |
66.2 |
58.1 |
54.8 |
56.0 |
56.0 |
|
Digestion organs’ illnesses |
65.5 |
62.8 |
61.7 |
63.7 |
62.7 |
|
Other causes of death |
220.7 |
198.5 |
182.5 |
172.2 |
158.3 |
|
Of them: Accidental alcoholic poisonings |
28.6 |
23.1 |
17.7 |
16.9 |
15.0 |
|
Transport accidents |
28.1 |
26.8 |
27.5 |
25.0 |
21.2 |
|
Road accidents |
- |
17.5 |
18.2 |
16.5 |
14.5 |
|
Suicides |
32.2 |
30.1 |
29.1 |
27.1 |
26.5 |
|
Murders |
24.9 |
20.2 |
17.9 |
16.7 |
15.1 |
The purpose of this research is estimating the structure of suicide-dangerous emotional disorders (by the example of Karelia Republic), in their interrelation with socio-economic and natural-climatic factors for developing the algorithms of diagnosing and preventing this negative phenomenon.
The problem of suicides is multi-complex and multidisciplinary. In spite of the fact that there exist a lot of researches on the mentioned problem, they basically have a clinic descriptive character. In such researches the factors of suicide risk are stated, but in a very abstract view (sex, age, steady psychological characteristics). Meanwhile, the clinical data show that the presence of the emotional problems of depressive and disturbing spectrum frequently make the motive of the voluntary deprivation of life.
One of the most important problems is suicide risk forecasting. For such a small region in Russia as Karelia (with the population less than one million people), the problem of suicides remains traditionally actual. While carrying out this research we have made the mathematical processing of the survey results of those people who made one or more suicide attempts for the last 5 years (according to the data of Petrozavodsk Republican Psychiatric Clinic). 54 patients who made attempts of committing suicides were interrogated.
The information about the patients was represented as an information system including seven blocks: suicide date, general information about a patient, personal peculiarities, financial position, situation that caused the attempt of committing suicide, state of health, family status (fig. 2) .
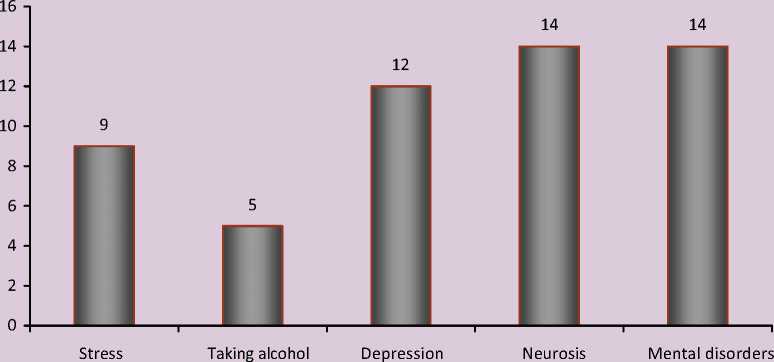
Each patient was characterized according to 19 attributes (tab. 3) .
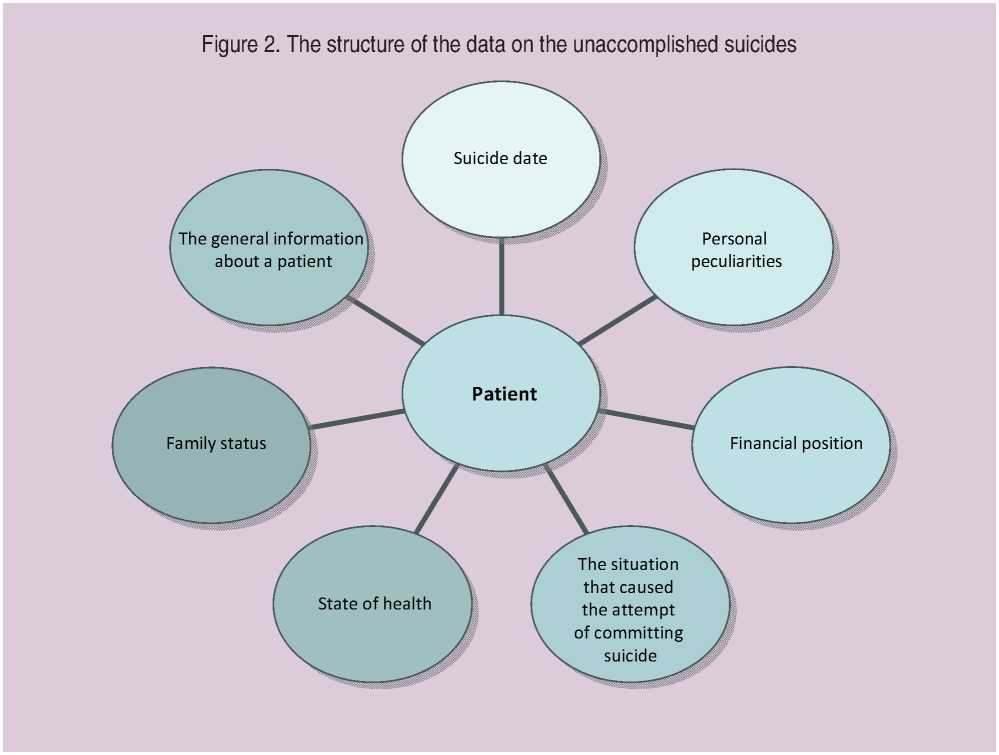
Table 3. Features describing the patients of Petrozavodsk Republican Psychiatric Clinic, who made attempts of suicide
|
Feature name |
Variants |
Cases (%) |
|
Month of the suicide’s commitment |
January |
9.3 |
|
February |
9.3 |
|
|
March |
11.1 |
|
|
April |
13.0 |
|
|
May |
13.0 |
|
|
June |
11.1 |
|
|
July |
9.3 |
|
|
August |
0.0 |
|
|
September |
7.4 |
|
|
October |
9.3 |
|
|
November |
3.7 |
|
|
December |
3.7 |
|
|
Diagnosis (cause) |
Stressful situation |
16.7 |
|
Alcoholic dependence |
9.3 |
|
|
Depression |
22.2 |
|
|
Neurosis |
25.9 |
|
|
Mental disorders |
25.9 |
|
|
Age |
From 13 to 18 |
22.2 |
|
18-30 |
27.8 |
|
|
30-40 |
22.2 |
|
|
40-50 |
16.7 |
|
|
50-60 |
5.6 |
|
|
Over 60 years |
5.6 |
|
|
Sex |
Male |
24.1 |
|
Female |
75.9 |
|
|
Environs |
Own family (spouses, children) |
48.1 |
|
Parents |
33.3 |
|
|
Other relatives |
7.4 |
|
|
Friends |
1.9 |
|
|
Neighbors |
7.4 |
|
|
No environs |
1.9 |
|
|
Occupation |
Unemployed |
14.8 |
|
Military service |
1.9 |
|
|
Student |
27.8 |
|
|
Pensioner |
9.3 |
|
|
Intellectual labour |
7.4 |
|
|
Manual labour |
38.9 |
|
|
Education |
Secondary education (school) |
35.2 |
|
Specialized secondary education |
51.9 |
|
|
Inchoate higher education |
1.9 |
|
|
Higher education |
11.1 |
|
|
Interests |
Intellectual and aesthetic |
7.4 |
|
Connected with nature |
1.9 |
|
|
Sporting |
3.7 |
|
|
Professional and household |
87.0 |
|
|
Means |
Low |
53.7 |
|
Average |
46.3 |
|
|
High |
0.0 |
Finishing table 3
|
Situation |
Interpersonal problems |
61.1 |
|
Personal problems |
35.2 |
|
|
Social problems |
3.7 |
|
|
Household проблемы |
0.0 |
|
|
Physical inability |
Not presented |
83.3 |
|
Mental illness |
7.4 |
|
|
Somatic illness |
9.3 |
|
|
Way of suicide |
Poisoning |
63.0 |
|
Injuiring |
29.6 |
|
|
Fire |
0.0 |
|
|
Hanging |
7.4 |
|
|
Drowning |
0.0 |
|
|
Other |
0.0 |
|
|
Type of suicide |
Real |
72.2 |
|
Manipulating |
27.8 |
|
|
Order of attempt |
First |
68.5 |
|
Repeated |
31.5 |
|
|
Expert’s supervising |
Was supervised before a suicide |
25.9 |
|
Was not supervised before a suicide |
74.1 |
|
|
Additional illnesses |
Therapeutic |
31.5 |
|
Neurological |
11.1 |
|
|
Narcological |
7.4 |
|
|
No illnesses |
50.0 |
|
|
Hospitalization |
Was hospitalized |
75.9 |
|
Was not hospitalized |
24.1 |
|
|
Housing |
First-class accommodation |
75.9 |
|
Not-equipped accomodation |
13.0 |
|
|
Rented |
3.7 |
|
|
Hostel |
7.4 |
|
|
No habitation |
0.0 |
|
|
Place of residence |
Petrozavodsk |
88.9 |
|
Other |
11.1 |
General characteristic of suicide attempts. As a result of the carried out research the general features of self-murderers, despite differences in age, social status and environs, were stated. We managed to analyze the clinical features and to find the key symptoms which led to the attempts of committing suicides.
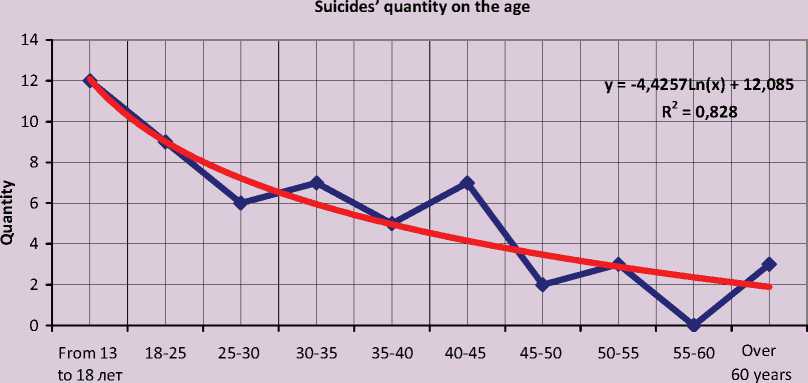
The probability of committing a suicide decreases with age (the most critical age is till 30 years) and can be described by the logarithmic function of regress (fig. 3 ):
y = -4,42 x ln( x) +12,08, R2 = 0,828, where y – is the quantity of the committed suicides;
x – is the age of committing a suicide.
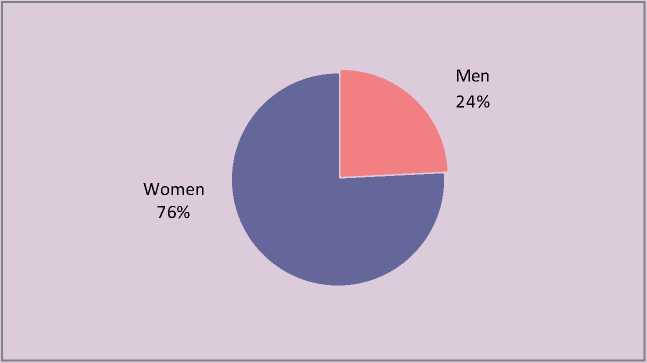
The share of women, who made attempts of committing a suicide, makes 76% and considerably surpasses the similar parameter among men (24%) (fig. 4) .
The majority of suicide attempts (72%) had true character, i.e. the serious attempts to commit an act of self-murdering were really made. The most part of suicides (63%) are poisoning with the big dozes of medical products, serious wounds make 30%, hanging makes 7%. 68% of patients made attempts of committing a suicide for the first time, 32% of patients made them again.
The material shows that there practically were not impulsive suicide attempts. Crisis situations and the condition of mental
Figure 3. Dependence of the committed suicides’ quantity on the age
Age
Figure 4. The share of the suicide attempts committed by men and by women
discomfort arose long before the attempts of committing a suicide, but no measures for solving these problems were undertaken by suicides (fig. 5) . Indirectly it can prove the absence of the valuable attitude towards self, and to health.
In overwhelming majority of cases (76%) applying for medical treatment followed the attempt of committing a suicide though the staff at Petrozavodsk Republican Psychiatric Clinic gives consultations and the help is rendered anonymously and free-of-charge.
While analyzing the clinical information it became possible to state the socio-economic and natural-climatic factors, which led to attempts of committing a suicide.
Natural-climatic conditions. Karelia republic does not join the group of large advanced industrial territories; therefore one of the factors influencing a person’s health is a natural-climatic factor. Climate as the factor forming ecologically caused diseases of a natural origin has its peculiarities in Karelia. Great variability of meteorological elements from year to year and from day to day is characteristic for it.
Figure 5. Crisis situations which led to suicide attempts
Winter usually lasts more than 5 months with the temperature reaching 30 below zero. The whole territory of the Republic is the zone with the excess moisture (the relative humidity makes >80% for 150 or 200 days in a year, 600 or 750 mm of atmospheric precipitation, frequent fogs). Sharp changes of the weather conditions cause fluctuations of the oxygen contents in the air that greatly affects a human organism.
In Karelia the natural shortcoming of the ultra-violet radiation is marked. Thus, the territory of Karelia Republic can certainly be referred to the zones with discomfort conditions for people’s habitation, and according to some parameters it even can be referred to the zone with extreme condition.
In this connection, the high level of depressions of various structure and genesis accumulates with depressive syndromes of the seasonal affective disorders (SAD).
SAD are characteristic for the countries of the Northern Europe as a whole, and for Karelia in particular. The period of the SAD clinical features is more than five months: from October to March. The combination of various depressive symptoms is an uneasy clinical problem. In this research the depressive symptoms were practically always combined with the alarm condition which is a through symptom at suicides. We should note the specificity of defying depressions: they are categorical and non-alternative; the ideas of self-deterioration, hopelessness, senselessness of life prevail. Existential emptiness logically crowns any depression even if it is not comprehended in such terminology and up is not realized completely. All these symptoms are the matrix in which the suicide ideas and plans form.
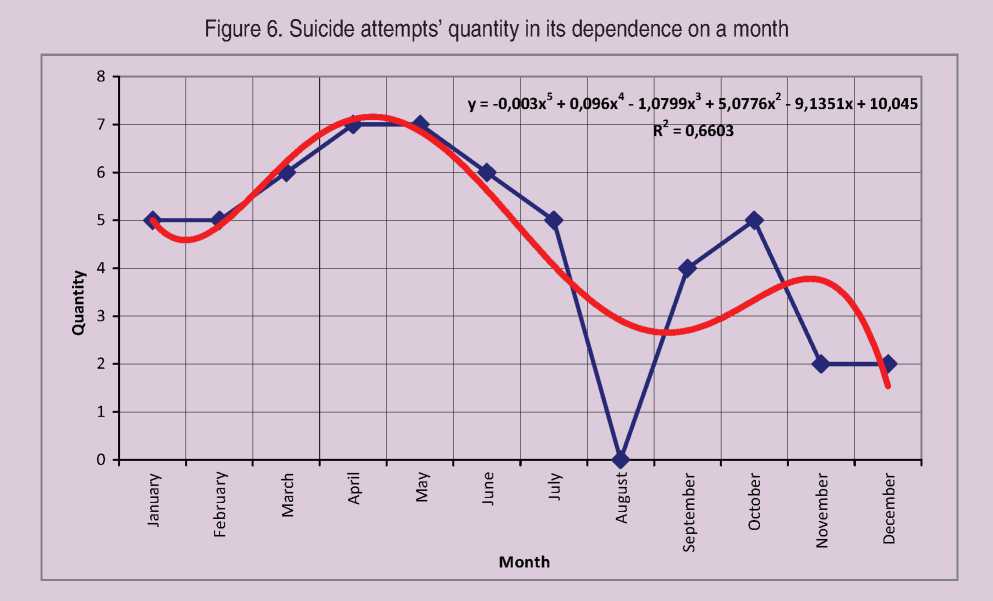
The peak of suicide attempts, as a rule, falls to the spring and some summer months (March, April, May, June). The quantity of the committed suicide attempts depending on a year’s month is represented in Figure 6 and is approximately described by the multinomial regress function:
y = -0,003 x 5 + 0,096 x 4 – 1,079 x 3 +
+ 5,077 x 2 – 9,135 x + 10,04
R2 = 0,66, where y is the quantity of the committed suicide attempts;
x is a month of a year.
One of the probable interpretations of such pattern is coincidence of this time period with the end of SAD symptoms. As we know, it is widespread in the countries of the Northern Europe from October to March and proceeds with the sub clinical depressive symptoms. Probably, the examined patients had accumulation of affective disorders and SAD simultaneously. Long-lasting condition of being in a low spirit, ambiguity of the clinical picture at remaining of the functions of declaration of will and pessimistic attitude could result in gradual formation of the suicide plan and its realization at the end of SAD.
Personal characteristics. Besides the clinical component it is necessary to mention personal characteristics. The richer is a person’s inner world, his or her values, beliefs, the more he or she is tolerant towards the crisis situations, the greater resource a person has at solving vital problems (in our case at depressive disorders). Such person forms an anti-suicide barrier against the suicide ideas and actions. A person with a weak personal structure doesn’t have the anti-suicide barrier, so the risk of committing a suicide increases.
The problem of values, to be more exact, their absence or weak share in a person’s structure, is characteristic for suicides in general.
The values of personal growth, professionalism, mutual relations with people were not developed and were not significant for the examined patients. As a rule, they had a low social status, non-creative jobs (15% are unemployed, 28% are students, 9% are pensioners, 39% – are occupied with manual labour).
Crisis situations arose mostly in families; committed suicides were addressed to family, actually suicide attempts occurred in home conditions, more often at the presence of family members (81 % of patients had families or lived in parents’ family). It is necessary to note, that not only the suicides themselves, but also the members of their families did not pay attention to the changes of the relative’s mental condition. No one appealed to the expert for consultation for this occasion.
Existential, cultural values were weakly represented in the personal structure of the examined patients. 87% of the examined patients had secondary and specialized secondary education; and only 11% got higher education. 87% of patients had no hobbies, and were involved into the decision of economic problems.
Economic factors. The features of the economic structure in Karelia Republic are a rather low level of the population’s incomes, economic opportunities’ limitation, difficulties with the professional employment, and nonproviding with the high-quality rest.
Values of the material order also could not be estimated by suicides. Money cannot give freedom itself, but it can give the feeling of this freedom. However the patients’ level of incomes was low (54%), and average (46%), no one had the high level of incomes. So, poverty and weakness of the inner world were the uniting criteria which all the patients had.
Thus, we managed to analyze the clinical features and to find the key symptoms which led to the attempt of committing a suicide. It was an affective complex of symptoms, namely: either anxiety, or depression, or even (more often), the combination of anxiety and depression. According to a rather exact definition given by Alfried L’Angle, depression is “the loss of the ability to experience the value of life”. Anxiety is a subjectively badly tolerable feeling of alarm and pressure. Either separately, or in a combination with each other alarm and depression sharply reduce the valuable experience of life in all its variety and manysidedness. Thus, even sub clinical forms of the affective pathology led to the realization of the suicide behavior.
Undoubtedly, that significant influence was rendered by the social environment in which the patients lived: low income, absence of strong family mutual relations, and scarcity of personal interests. In many respects it was determined by a complex socio-economic situation in which a person did not feel necessary for the society.
The results received during mathematical processing of the clinical supervision data proved to be true: suicide attempts were made by immature persons with weak values, with non-creative jobs, with the inability to make emotionally stable interactions with the associates, with the extremely limited range of reactions in crisis situations.
To lower the level of suicides, a serious work should be carried out. The initial features of the affective disorders can be seen by both the patients’ relatives and the doctors of the general practice, hence:
-
• Training the general practice doctors is necessary for revealing suicide-leading affective disorders, and for this purpose the diagnostic questionnaires of depression and alarm in the standard of examining are expedient to be introduced. Revealing mood disorders at early stages could lead to a timely patient’s direction to experts. All the patients, mentioned in this research, appealed for help months after the beginning of the depressive disorders.
-
• Crisis situations basically arose in the family environment. Psychotherapeutic work with families, as well as popularization of the family values can become a basis of the preventive work, both with the potential suicides, and with the real ones.
-
• It is necessary to take appropriate measures on the improvement of the socioeconomic position of the representatives of the suicide risk groups: unemployment reduction, labor motivation, creation of the specialized psychological centers.
References Influence of socio-economic factors on the suicide type of behavior
- The World Organization of Public Health Service/. -Available at: http://www.who.int
- The World Organization of Public Health Service, Bulletin № 220. Mental health: struggle against mental disorders/. -Available at: http://www.who.int/mediacentre/factsheets/fs220/ru/index.html
- The World Organization of Public Health Service’s database: Health for everybody/. -Available at: http://www.euro.who.int/hfadb?language=Russian
- The Russian statistical year-book. 2009: stat. coll./Rosstat. -М., 2010.
- Karelia Republic in figures: stat. coll./KareliaStat. -Petrozavodsk, 2009.
- Durkheim, E. Suicide/E. Durkheim. -M.: Myisl, 1994.
- Efremov, V.S. The bases of suicide-studying/V.S. Efremov. -Saint-Petersburg: Dialect, 2004.
- Morev, M.V. Socio-economic and demographic aspects of suicide behavior/M.V. Morev, A.A. Shabunova, K.A. Gulin; ed. Doctor of Economic Science, Professor V.A. Ilyin. -Vologda: Institute of socio-economic development of territories of the Russian Academy of Science, 2010. -188 p.
- Suicide-studying: past and present. The problem of suicide in the works of philosophers, sociologists, psychologist and in fiction. -M.: Kogito-Centr, 2001.
- Suicide-studying in the works of foreign scientists/ed. A.N. Mohovikov. -M.: Kogito-Centr, 2003.
