Non-infectious Causes of Rash Mimicking Infectious Diseases

Author: Mamatkulova N., Rashid Nawaz, Shaikh Mohd Farhan Farooq, Toheed
Journal: Бюллетень науки и практики @bulletennauki
Section: Медицинские науки
Article in issue: 3 т.12, 2026.
Free access
Non-infectious rashes often mimic infectious etiologies and are, therefore, a source of diagnostic difficulty, treatment delays, and mismanagement. The clinical overlap is due to similarities in morphology, systemic symptoms, and patterns of distribution. This article provides an in-depth scholarly review of the non-infectious disorders that clinically resemble infectious dermatologic diseases and includes drug eruptions, autoimmune disorders, allergic reactions, vascular pathologies, genetic syndromes, and environmental causes. Using a narrative review-based methodological approach, clinical presentation, diagnosis-related pitfalls, differential features, and modern investigative techniques are discussed. The findings highlight the need for early consideration of non-infectious mimickers in clinical assessment to avoid unnecessary use of antimicrobials and adverse consequences. Recommendations for practitioners relate to structured diagnostic algorithms, increased dermatology training, collaboration across medical disciplines, and refined clinical guidelines.
Non-infectious rash, infectious mimickers, dermatologic differential diagnosis, autoimmune rash, drug eruptions, allergic dermatitis, vasculitis, morbilliform eruption, diagnostic pitfalls, dermatology
Short address: https://sciup.org/14134705
IDR: 14134705 | UDC: 616.9-022 | DOI: 10.33619/2414-2948/124/23
Неинфекционные причины сыпи, имитирующие инфекционные заболевания
Неинфекционные высыпания часто имитируют инфекционные заболевания и, следовательно, являются источником трудностей в диагностике, задержек в лечении и неправильного подхода к терапии. Клиническое сходство обусловлено схожестью морфологии, системных симптомов и характера распространения. В данной статье представлен углубленный научный обзор неинфекционных заболеваний, которые клинически напоминают инфекционные дерматологические заболевания, включая лекарственные высыпания, аутоиммунные заболевания, аллергические реакции, сосудистые патологии, генетические синдромы и экологические причины. Обсуждаются клиническая картина, диагностические ошибки, дифференциальная диагностика и современные методы исследования. Результаты подчеркивают необходимость раннего рассмотрения неинфекционных заболеваний, имитирующих инфекционные, при клинической оценке, чтобы избежать ненужного использования противомикробных препаратов и неблагоприятных последствий. Рекомендации для практикующих врачей касаются структурированных диагностических алгоритмов, повышения квалификации дерматологов, сотрудничества между медицинскими дисциплинами и усовершенствованных клинических руководств.
Text of the scientific article Non-infectious Causes of Rash Mimicking Infectious Diseases
Бюллетень науки и практики / Bulletin of Science and Practice
UDC 616.9-022
Skin rashes are among the most frequent reasons patients seek medical attention, appearing across all age groups and healthcare settings. While infections are commonly considered the primary cause, many rashes are, in fact, non-infectious and closely resemble infectious diseases in appearance, pattern, and associated symptoms such as fever, fatigue, or swelling [1].
Because of this similarity, clinicians often face difficulty in making an accurate diagnosis during the initial assessment [2].
The challenge arises from the skin’s limited range of inflammatory responses. Different disease processes—whether infectious, allergic, autoimmune, or drug-related—can activate similar immune pathways, leading to overlapping clinical features including redness, maculopapular eruptions, vesicles, and purpuric lesions [3].
In busy clinical environments, these similarities may prompt an assumption of infection, particularly when rapid decisions are required [4].
Misinterpreting a non-infectious rash as an infectious one can have serious consequences. Patients may be exposed to unnecessary antibiotics or antiviral medications, increasing the risk of adverse drug effects and contributing to the global problem of antimicrobial resistance [5].
At the same time, failure to recognize non-infectious conditions such as autoimmune diseases or severe drug reactions may delay appropriate treatment and allow potentially dangerous complications to develop [6].
Several non-infectious disorders, including medication-induced eruptions, allergic reactions, inflammatory dermatoses, and vasculitic syndromes, are well known for their ability to imitate classic infectious rashes such as measles, chickenpox, cellulitis, and meningococcemia [7].
The presence of systemic features and nonspecific laboratory abnormalities further complicates differentiation and increases the likelihood of misdiagnosis [8].
As modern medical practice becomes increasingly complex due to polypharmacy, chronic disease, and heightened immune dysregulation, the need for improved recognition of non-infectious rash mimickers has become more critical. A clearer understanding of these conditions can enhance diagnostic accuracy, reduce unnecessary antimicrobial use, and improve patient outcomes. This article explores the major non-infectious causes of rashes that mimic infectious diseases, with the aim of supporting safer and more effective clinical decision-making [9].
Material for this article is based on an academic literature review in dermatology, immunology, internal medicine and public awareness survey on Google forms. Specific sources include peerreviewed journals, textbooks of dermatology, clinical guidelines, and epidemiological reports published within the past twenty years. This review focuses on those non-infectious etiologies that present with morphologic or symptomatic features similar to infectious rashes. Selection was biased toward conditions that are frequently misdiagnosed as infectious diseases in the clinical setting. Emphasis was placed on distinguishing features, pathophysiology, and diagnostic strategies. Although this is not a systematic review, this methodological approach does allow for comprehensive synthesis and contextual interpretation of diverse scholarly evidence in accord with academic standards.
-
1. Mimicking Phenomena in Dermatology. Rash mimickers arise due to the skin's limited repertoire of inflammatory responses. Erythema, scaling, vesiculation, petechiae, and edema can result from different pathologic processes yet may appear morphologically identical. Because of this, entities that arise from allergic, vascular, autoimmune, and even medication etiologies can clinically masquerade as infectious conditions. Medication-induced morbilliform eruptions often have a similar presentation to viral exanthems. Similarly, vasculitic purpura can take on an appearance very much like meningococcemia. Dermatologic mimicry reflects the shared pathways of cytokine release, vascular permeability alterations, and immune-mediated damage. Interleukins, TNF-α, and interferons have been considered the players in the inflammatory cascades observed in both infectious and non-infectious conditions. Appreciation of these mechanisms will provide an understanding of why the diagnostic confusion persists, even by seasoned clinicians.
-
2. Drug-induced rashes mimicking infectious diseases. Drug reactions are one of the most significant non-infectious mimickers. Drug-related cutaneous reactions occur in approximately 2-5% of hospitalized patients, and the most common are morbilliform eruptions. Morbilliform eruptions consist of erythematous macules and papules that have a very close resemblance to viral exanthems like measles and rubella. Morbilliform drug eruptions begin 7–14 days following medication exposure and are considered T-cell–mediated hypersensitivity reactions. Maculopapular lesions present diffusely and symmetrically, often appearing identical to viral exanthems. Unlike viral exanthems, however, drug eruptions tend to coalesce on dependent regions of the body and can remain present even after the resolution of systemic findings.
SJS and TEN can present similarly to life-threatening infectious blistering diseases like staphylococcal scalded skin syndrome. SJS/TEN is a drug-induced process characterized by widespread epidermal necrosis and typically induced by medications such as anticonvulsants, sulfonamides, and NSAIDs. Fever, mucosal involvement, and targetoid lesions often suggest a viral etiology to the clinician; however, rapid progression with full-thickness epidermal detachment will strongly point toward a drug-induced process.
Fixed Drug Eruptions Mimicking Herpes Simplex present as sharply demarcated erythematous patches, which may blister, and recur at exactly the same site with re-exposure to the causative drug. These can resemble localized herpes simplex infections, particularly when occurring on the lips or genital region. The absence of viral prodrome and the presence of single, sharply bordered lesions support a drug-induced diagnosis [6].
Autoimmune and Inflammatory Disorders Masquerading as Infectious Rash. Many autoimmune diseases manifest through the skin in a way that makes it appear to be an infectious process because of the production of cytokines initiated or resulting from an immune-mediated response. Systemic Lupus Erythematosus (SLE). The malar rash of SLE is often mistaken for erysipelas due to its erythematous, butterfly-shaped appearance and facial swelling. Unlike bacterial erysipelas, SLE rashes spare the nasolabial folds and typically do not have severe tenderness or leukocytosis. Dermatomyositis can be disguised in the form of viral exanthems characterized by heliotrope rash and Gottron's papules. The periorbital rash resembles allergic dermatitis or cellulitis, while generalized erythema may resemble viral eruptions. Guttate psoriasis is mainly characterized by drop-like scaly papules, making it mostly similar to streptococcal infections. The eruption may thereby be confused with varicella; this is common in children.
Allergic and Hypersensitivity Reactions Simulating Infections. Hypersensitivity reactions often cause diffuse erythema, vesicles, and pruritus.
Allergic Contact Dermatitis. Acute contact dermatitis often resembles herpes zoster because of the linear vesicular patterns produced by exposure to plants, especially urushiol-induced dermatitis. The intense pruritus and typical bilateral distribution, however, differentiate it from infectious causes.
Urticaria Multiforme. It is similar to erythema multiforme or viral urticaria. It is characterized by annular wheals and central clearing, which is often mistaken for fungal infection or erythema migrans.
Vasculitic Disorders Mimicking Infectious Diseases. Vasculitic rashes are among the most challenging non-infectious conditions to distinguish from infectious etiologies because they frequently present with petechiae, purpura, necrosis, ulceration, fever, malaise, arthralgias, and elevated inflammatory markers — symptoms that strongly resemble bacterial sepsis and viral hemorrhagic conditions. Small-vessel vasculitis, in particular, creates cutaneous patterns analogous to meningococcemia, especially when lesions appear abruptly and progress rapidly [3].
Immune complex vasculitis, formerly known as leukocytoclastic vasculitis, produces symmetrical palpable purpura predominantly on lower extremities. Clinically, this resembles disseminated intravascular infections that lead to petechial eruptions. However, unlike infectious purpura fulminans, vasculitic lesions usually develop more gradually, exhibit less systemic toxicity, and may follow medication exposure or autoimmune activation. As previously noted, Henoch– Schönlein Purpura (HSP), or IgA vasculitis, may be confused with meningococcal septicemia because of its purpuric rash. However, HSP predominates in pediatric populations, involves characteristic colicky abdominal pain, arthralgia, renal involvement, and follows respiratory infections without producing severe shock. A careful review of systemic involvement and absence of severe coagulopathy often redirects diagnosis toward a non-infectious etiology.
Genetic and Metabolic Disorders Mimicking Infectious Rash. While less frequently mistaken, various genetic and metabolic disorders result in rashes that appear similar to viral exanthems or bacterial infections. Chronic atopic dermatitis may become acutely erythematous, crusted, and exudative, appearing similar to impetigo or eczema herpeticum. Flare-ups triggered by irritants, allergens, or stress often result in widespread erythema and scaling analogous to diffuse infectious dermatitis. However, atopic dermatitis usually displays a characteristic history of relapsing flares, flexural involvement, and intense pruritus.
The scaling and erythema associated with ichthyosis vulgaris and X-linked ichthyosis may occasionally mimic tinea infections. The presence of chronicity, early onset, and generalized distribution aids in the differentiation of these genetic causes from localized infectious etiologies.
Despite being inflammatory and non-infectious, Kawasaki disease often presents a measles-like rash that usually presents with fever, injected conjunctivae, strawberry tongue, and lymphadenopathy of the neck and thus may be confused easily with viral infections like adenovirus or scarlet fever. Making this distinction is necessary because Kawasaki disease necessitates timely immunomodulatory therapy to prevent coronary artery aneurysm formation.
Environmental and Physical Factors that Mimic Infectious Diseases. These exposure-related dermatoses can simulate infectious lesions, especially when erythema, blistering, or necrosis occurs.
Phototoxic reactions present as sharply demarcated erythema and blistering, resembling herpes zoster or cellulitis. It occurs on sun-exposed sites shortly after ultraviolet exposure in persons taking photosensitizing drugs. The pattern of photodistribution remains the most significant diagnostic clue, since infectious rashes rarely have such well-demarcated borders [5].
Erythema, blistering, and peeling due to burn injuries can often look similar to bullous impetigo or SJS/TEN. Thermal injury is usually associated with a clear history of exposure, sharp demarcation of the edges, and no systemic prodrome. Insect bites may appear similar to varicella or viral eruptions due to clustered vesicles and intense pruritus. Linear groupings-the "breakfast, lunch, and dinner" pattern-are highly suggestive of scabies infestations but originate from bedbug exposure. Knowledge of the distribution of bites and recurrences following sleep helps the clinician differentiate between infectious and environmental etiologies. Psychological and Behavioral Disorders Resembling Infectious Rash. Although uncommon, psychodermatologic conditions contribute to diagnostic confusion.
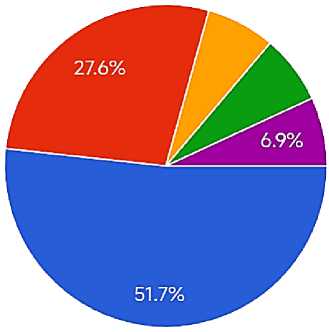
• Infection (virus, bacteria, fungus)
• Allergy
Medication reaction
• Allergies
* Medicines
• Autoimmune diseases
# Stress ф Sun exposure ф I do not know
-
• Environmental factors (sun, chemicals, plants)
-
• I do not know
Main causes of Skin Rashes
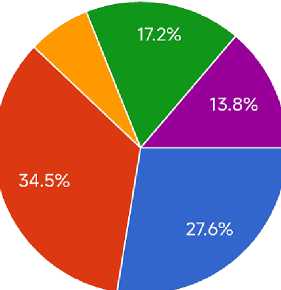
Non-Infectious skin Rashes
While self-inflicted lesions can be made to mimic bacterial or viral infections, the pattern of distribution is often bizarre and geometric. Lack of typical time progression for an infection, with non-concordant history from the patient, will eventually raise suspicion among clinicians that psychogenic causes need to be considered.
The patients may have excoriations with self-induced erosions that may suggest parasitic infections. Misdiagnosis may lead to unnecessary antiparasitic therapy until behavioral patterns are recognized. The analysis reveals several key findings. First, the greatest diagnostic overlap occurs between drug eruptions and viral exanthems, vasculitides and bacterial septicemic rashes, and autoimmune conditions and erythematous infectious dermatoses. Second, non-infectious mimickers often share three major clinical elements with infectious rash presentations: erythema, fever, and systemic symptoms. Third, reliance on visual morphology alone leads to frequent misdiagnosis. Fourth, systemic context—including drug exposure, autoimmune history, allergic profile, and environmental triggers—provides the most critical differentiating clues. Fifth, diagnostic delays predominantly occur in emergency and primary care settings where rapid decisions are necessary, and dermatologic expertise may be limited. Sixth, misdiagnosis contributes to unnecessary antimicrobial use, delays in immunomodulatory treatment, patient anxiety, and increased healthcare costs. Finally, standardized diagnostic algorithms and improved dermatologic training substantially reduce these diagnostic errors [8].
Discussion
These findings emphasize that any rash evaluation requires a structured and multidimensional diagnostic approach. Limited skin response patterns prohibit reliance on morphology alone, a practice that would be no less than dangerous. A detailed history, including medication exposure, temporal relationship of symptoms, environmental triggers, and systemic manifestations, is required for accurate differentiation.
Thus, misdiagnosis of non-infectious rashes as infectious not only contributes to unnecessary antimicrobial therapy but also plays into broader public health concerns about antimicrobial resistance. Conversely, failure by clinicians to identify non-infectious inflammatory, autoimmune, or vasculitic causes leaves the patient open to complications ranging from simple organ involvement to life-threatening systemic reactions.
Dermatologic education remains a key limitation in many curricula. The primary care physician and emergency clinician are commonly faced with rashes, largely without formal dermatologic training, leading to reflexive assumptions of infection. The literature supports a need for the integration of dermatologic algorithms, teledermatology consultations, and improved visual diagnostic training into health systems.
Histopathology and laboratory testing also play an indispensable role. While infections may produce neutrophilic infiltrates, non-infectious conditions have specific patterns such as immune complex deposition, interface dermatitis, or vasculitic changes. Early biopsy can avoid misdiagnosis, especially in rapidly progressive or atypical rashes.
The interplay of the immune response pathways in both infectious and non-infectious conditions forms the biological rationale for clinical confusion. Overexpression of cytokines, vascular injury, and keratinocyte apoptosis stand out across pathologies diverse in nature, reinforcing the contextual interpretation over morphology alone.
Conclusion
Non-infectious causes of rash that mimic infectious diseases represent a critical diagnostic challenge. This article illustrates that drug eruptions, autoimmune conditions, vasculitides, allergic reactions, genetic disorders, environmental exposures, and psychogenic conditions all have clinical overlap with infectious presentations. The major mistakes are made based on overreliance upon visual inspection without adequate history-taking, delay in the use of diagnostic modalities, and limited dermatologic training. Knowledge of distinguishing features, including distribution patterns, systemic associations, recurrence behaviors, and response to triggers, can significantly enhance diagnostic accuracy. This requires an interdisciplinary perspective on dermatology, immunology, general medicine, and emergency medicine for the ultimate goal of minimizing misdiagnosis, improving patient outcome, and reducing unnecessary use of antimicrobial agents. Adopt structured diagnostic algorithms that incorporate morphology, distribution, systemic symptoms, and exposure history. Increase dermatologic training throughout all medical curricula, especially among non-specialists. Improve access to teledermatology for rapid consultation in equivocal cases. Encourage early biopsy and laboratory investigations when rashes progress rapidly or when they fail to conform to infectious patterns. Educate clinicians regarding drug-induced eruptions, including common culprits and temporal relationships.
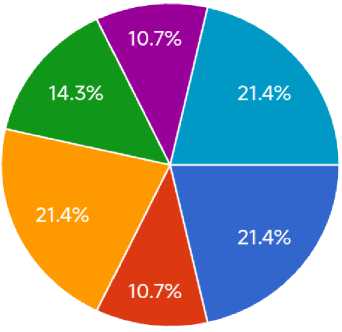
Best way to educate people about skin health?
• Doctors and hospitals
-
• Social media
-
• Television and radio
-
• Schools and universities
-
• Community programs
All antimicrobial stewardship protocols should call for differential exclusion of non-infectious causes prior to starting broad-spectrum therapy. Encourage multidisciplinary collaboration among dermatology, infectious disease, rheumatology, and primary care. Develop patient education materials explaining the importance of medication history and environmental exposures. Support public health initiatives to reduce the healthcare burden from misdiagnosis. Expand research on visual decisionsupport systems and AI-based diagnostic tools in rash assessment.
