Оценка морфологических изменений твердых зубных тканей, обработанных лазером и ротационными инструментами с помощью ультразвукового электронного микроскопа

Автор: Томов Георгий
Журнал: Саратовский научно-медицинский журнал @ssmj
Рубрика: Стоматология
Статья в выпуске: 3 т.6, 2010 года.
Бесплатный доступ
Эффективные методы удаления твердых зубных тканей с помощью лазерного иттрий-алюминиевого граната (ИАГ) стали применяться сравнительно недавно с целью подготовки полости зуба и удаления кариеса. Однако ряд исследователей выявили морфологические изменения в твердых зубных тканях после лечения лазерным ИАГ. Целью настоящего научного исследования является сравнительный анализ лазерного лечения и инструментального традиционного лечения. В качестве материала для исследования были взяты 30 экстрактированных кариозных зубов пациентов, из них 10 подверглись лазерному лечению, остальные 20 - традиционному лечению с помощью стальной и алмазной пластинок. Лазерное лечение проводилось на основе неинвазивного распыления охлаждающего спрея на водяной основе с новым лазерным компонентом (ИАГ). Традиционное лечение осуществлялось с помощью низкоскоростного микродвигателя и воздушно-турбинной бормашины с охлаждением воды. Результаты каждого метода лечения оценивались ультразвуковым электронным микроскопом. Эффективность лечения лазерным ИАГ доказана при удалении кариозного дентина с минимальным термическим повреждением, окружающего интактного дентина и инфицированного и размягченного дентина в такой же степени, как и эффективность традиционного лечения. Низкая степень вибрации доказана как одно из преимуществ лазерного метода лечения. Данные, полученные при исследовании ультразвуковым электронным микроскопом, выявили микронеровности в дентине, подверженном лазерному излучению, и эмалированном покрытии зуба, требующем дальнейшего адгезивного восстановления. Результаты проведенного исследования подтверждают необходимость признания лазерного лечения ИАГ новейшим, модернизированным и эффективным методом лечения кариозных зубов
Лазерный иттрий-алюминиевый гранат, морфологические изменения, ультразвуковой электронный микроскоп
Короткий адрес: https://sciup.org/14917152
IDR: 14917152
Текст научной статьи Оценка морфологических изменений твердых зубных тканей, обработанных лазером и ротационными инструментами с помощью ультразвукового электронного микроскопа
1Introduction. The main categories of techniques for microinvasive preparation (MIP) include chemo
Address for correspondence:
Assist. Prof. Dr. Georgi Tomov.
Faculty of Dental Medicine
Department of Operative dentistry and endodontic.
-
3 Hristo Botev str.
4000 Plovdiv, Bulgaria.
mechanical cleaning with Carisolv gel, air abrasion and dental lasers [1, 2]. The trends for the replacement of the conventional method of preparation led to focus the attention of researchers on the impact of alternative techniques for MIP on hard dental tissues and underlying dental pulp. MIP techniques claim for controlled removal of infected and softened dentin while preserve healthy hard dental tissues and do it with minimal discomfort for the patient. However, currently available data provide contradictory the impact of alternative techniques of MIP on hard dental tissues compared to conventional preparation. Possible reasons for this are the variety of experimental studies and difficulties to standardize the results of clinical researches. It is striking that researchers who give the most positive evaluation of alternative methods of preparation are using mainly clinical criteria for evaluation (perception and tolerance of the patient, noise, atraumatic work, color and texture of the dentine when probing etc) which are some subjective. Oposite, the SEM and histologic evaluations are not unanimous for its benefits and advantages. On the dental market new improved versions of alternative systems for preparation are available claiming for clinical efficiency, but scientific data are still scarce (these are generally the multi-frequency high-energy lasers and air abrasion devices). For that reason periodic updates of researches in this rapidly developing and promising field of dentistry are needed.The purpose of this in vitro study was to evaluate by SEM the ultrastructural changes in the hard dental tissues treated with Er: YAG laser (LiteTouch) and conventional preparation with diamond burs/air turbine and steel burs/micromotor.
Methods. Experimental design: the study used 30 human teeth freshly extracted due to advanced periodontal disease. The preparation involved natural carious lesions on tooth surface.
According to the preparation technique the teeth were divided into 3 groups of 10 teeth (n=10):
Group 1. Laser preparation by Er: YAG laser (Lite-Touch, Syneron, Israel) (Fig. 1 a, b, c );
Group 2. Mechanical rotary preparation by diamond burs/air turbine);
Group 3. Mechanical rotary preparation by steel burs/micromotor.
Preparations are made strictly according to manufacturer’s instructions for service.
The removal of caries is proved by clinical methods – observation and probing. After preparation the teeth are immersed for 1 hour in 4% buffered fixative solution of glutaraldehyde (0.075 M, pH 7.3). Then rinsed with distilled water and placed for 90 min in cold buffer solution of sodium kakodilate (0.02M, pH 7.2, 660 mOsm) for fixation of organic matter. Subsequent dehydration is carried out in ethanol in ascending series of 30, 50, 70, 80, 95 and 100% in one hour in each series, such as drying of the teeth is based on CPD (Critical Point Drier) method in a dessicator. Dried specimens are fixed on metal stand and covered with gold layer (200-250nm) by cathode atomization under vacuum. Scanning microscopy is performed with the electron microscope of Philips (Holland) 515 model SEM with accelerating voltage of 25 kV in secondary emission mode. On each specimen were made respectively five pictures with the same magnification (x 2000) of randomly chosen areas and different numbers of photos with other magnification.
On SEM photos are rated, described and compared morphological findings and differences in enamel and dentin tissues after treating with alternative methods for caries removal and cavity preparation.
Results. Cavity forms prepared with Er: YAG laser (group 1) are characterized by a lack of definite and precise geometric configuration and outlined cavity elements. There is rough and irregular surface without presence of smear layer (Fig. 2 a ). Dentinal tubules orifices are clearly exposed. Intertubul dentin is ablated more than peritubular dentin and that made dentinal tubules appearance more prominent (Fig. 3 b ). In enamel the



с
Fig. 1. a, b, c . Laser preparation with Er: YAG laser LiteTouch (Syneron, Israel)
«Hard tissue mode» (400mJ/20Hz; 8.00W)
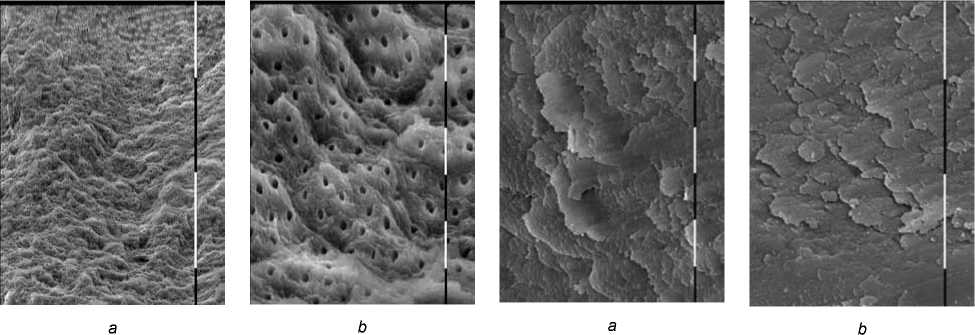
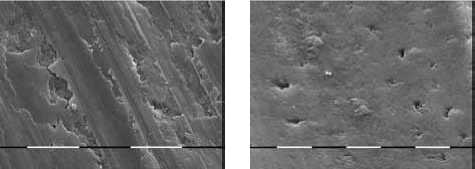
Fig. 4. a, b . SEM photomicrographies of tooth surfaces prepared with steel burs. The surface is covered with a layer of debris, dentinal tubules orifices are not visible.
(Magnification x 500, 2000)
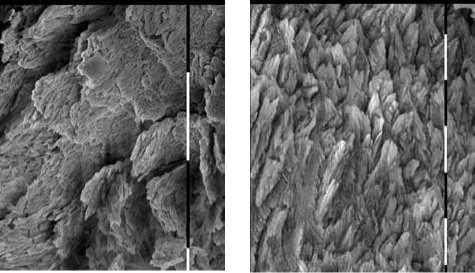
Fig. 2 a, b . Laser treated dentin. The surface is clean and free from debris, all dentinal tubules were found open. The surface is irregular, rough, which creates strong retentions. At greater magnification more effective removal of intertubular dentin is seen, and that makes dentinal tubules orifices to appear convex (Magnification x 500, 2000)
c
d
Fig. 2 c, d . Enamel surfaces treated with Er: YAG laser revealed characteristic architectonics of tufts grouped enamel prisms with differ orientation. The surface is very retentive and free from contaminants and smear layer (Magnification x 500, 2000)
typical architectonics of grouped in bundles enamel prisms is observed. Laser ablation changes enamel and the surfaces appeared strong retentive (Fig. 2 c, d ).
In group 2 (preparation with diamond burs, air turbine and water cooling) a thin, smooth and in some places missing smear layer was observed (Fig. 3 a ). In the area of water turbulence marked dentinal tubules orifices can be seen, but without having a clear outline of both tubules lumens and peri-and intertubular dentin (Fig. 3 b ). The boundary between enamel and dentin is unclear and the cavity forms heve smooth contours.
ab
Fig. 3. a, b . Smooth and thin smear layer covers tooth surfaces prepared with diamond burs and air turbine. In the area of water turbulence partially removed contaminants and single dentinal tubules lumena were observed. (Magnification x 500, 2000)
When analyzing the SEM photomicrographies of the specimens examined, it is found that the conventional method of cavity preparation with steel burs and micromotor at low speed without water cooling (group 3) leaves contaminated surface covered with smear layer of dentin debris without visible dentinal tubules orifices. (Fig. 4 a, b ). Thick smear layer covers all treated surfaces. The walls of the cavities are smooth and rounded and the border between enamel and dentin is not perceptible.
Discussion. The philosophy of minimally invasive cavity preparation approach is based on several main principles – to remove only irreversibly damaged dental tissues and to avoid macroretention preparation in healthy tissues [1]. Additionally these techniques should protect the underlying pulp and to leave the treated surface suitable for adhesive bonding [1]. Antibacterial effects of the alternative preparation techniques must not be lower than those of standard necrotomy with rotary instruments and even to excel them [1].
Nowdays the laser devices available for clinical use are capable for effective and controlled ablation of hard dental tissues [2]. However, not all researchers agree with these conclusions. Therefore, such studies should be periodically updated due to constant introduction of new technologies.
The experimental results of the presented study revealed significant differences in the surface morphology of the studied samples, which would affect the ability to perform effective adhesive bonding. These morphological differences are highly dependent on the mechanism of action of the used preparation systems.
Laser devices use a variety of physical media as sources for generating different wavelength that is absorbed and interact with specific molecules in human tissues. The explanation for the hard tissue ablation is the water content that evaporates when exposed on laser radiation creating high internal pressure and subsequent microexplosions. In this interaction of laser radiation with tissue if inadequate water cooling occured, that will lead to undesirable thermal effects [3]. Depending on parameters such as pulse energy and frequency CO2 lasers, Nd: YAG and Er: YAG lasers cause changes in enamel and dentin as roughing, craters, cracking, slicing, carbonification, melting and recrystallisation described in many previous studies [4, 5, 6]. These changes depend on the laser type, mode of operation, system for water cooling and proper operation [3]. Additionally, the oppor- tunities to ablate carious dentin and enamel strongly vary according to different experimental studies [4 - 6]. For ar-gon-fluoride laser (ARF) and the excimer laser there are data on their ability to remove dental caries, which is not of sufficient efficiency [5]. Krypton fluoride excimer laser emitting in ultraviolet range has been shown to remove dentin, but enamel resists the attempt for ablation [5].
Used in this experimental study, the high-powered and high-frequency Er: YAG laser (LiteTouch, Israel) has advanced hydrokinetic system that claims for effective and safe ablation of hard dental tissues. LiteTouch laser incorporates unique software, which allows for the broadest range of energy and frequency settings. The unique LiteTouch handpiece prevents loss of energy and along with the precision control over pulse duration, pulse energy and repetition rate optimize, allows for a wide range of hard tissues procedures. LiteTouch is the first laser in the world to use a novel mechanism that controls energy output, offering optimal control of treatment parameters. Easy adjustable water spray flow, frequency and energy levels on a touch screen following special software. LiteTouch is also innovative in respect of its optical system incorporated in the ergonomic handpiece working with sapphire tips. The proposed mechanism of action of this system is the photons radiation that laser source delivers in targeted air – water jet, resulting in water droplets microexplosions. It is believed that this process is the mechanism of ablating particles from dental tissues without overheating, and without smear layer formation [7]. Another characteristic of this laser is the wavelength (2940nm) which is absorbed most of the water and also sapphire tips, showing stability in providing focused energy of laser radiation [8]. This combination allows precise microinvasive cavity preparation with minimal heating and optimal rate of radiation absorption by the hydroxylapatite incorporated water [7]. The program «hard tissue mode» removes enamel, dentin and dental caries effectively and without visible carbonization or disturbance of the specimen microstructure. Evaluated under SEM the dental tissues treated with Er: YAG laser showed rough and irregular surface without presence of smear layer, open dentinal tubules orifeces were found as well. Intertubular dentin is ablated more than peritubular giving a characteristic appearance of the dentinal surface with mild prominent dentinal tubules. Enamel shows preserved prismatic structure, but also strong retentions due to microexplosions on its surface. Overall the cavity form is irregular, devoid of strict geometry and dotted with microretentions, but without presence of contaminants or smear layer. The observed changes correspond to changes in hard dental tissues reported by other authors in previous studies on Er: YAG lasers [9, 10], but without thermic degenerated surfaces, areas of extensive recrystallisation, melted surfaces or cracks in the dentin, as described in some in vitro studies [3 - 5]. It is also reported for better opportunities for adhesive bonding [11], faster ablation of enamel and dentin compared with rotating burs [12] and an increase in dentinal microhardness after treatment with Er: YAG pulsed lasers [13]. The latter statement is not confirmed by other studies. The marked surface irregularities and lack of smear layer observed in the recent study, noted also in other researches [14, 15] provide a solid evidence for the physical mechanism of bonding with composite materials after laser treatment [11]. This fact is not yet fully explored as a possible opportunity to eliminate acid etching of hard dental tissues and its related adverse effects on the underlying dentin and pulp.
The results of some contemporary studies showed that despite of the differences between individual authors, generally the amount of smear layer after treatment with Er: YAG laser in all cases is less than that after conventional rotating instruments, and surface changes are characterized by markedly rugged topography [2, 3, 12, 16].
The morphological features of hard dental tissues observed in our study suggested us to generalize that cavity preparation with Er: YAG laser is consistent with the principles of minimally invasive preparation, leaving clean surfaces and strong microretentions suitable for adhesive restorations. These assumptions about the benefits of alternative techniques for minimally invasive preparation of dental tissues for adhesive restorations should be confirmed in future clinical studies.
Conclusion . SEM analysis of hard dental tissues treated with steel and diamond burs showed surfaces covered with a thick layer of debris, which could compromise the adhesion of filling materials. Dental tubules orifices are obturated with debris, with exception the areas under water turbulence where the debris is partially removed.All laser-treated samples showed no evidence of thermal damage or signs of carbonification and melting. The SEM examination revealed characteristic microirregularities of the lased dentin surface without smear layer, and opened dentinal tubules. Intertubul dentin is ablated more than peritubular dentin and that made the dentinal tubules appearance more prominent. Er: YAG laser ablated enamel effectively and remained exposed enamel prisms without debris. The surfaces are very retentive.
The author declare not having any financial interest in a company (or its competitor) that makes a product discussed in the article or any conflicts of interest.
Список литературы Оценка морфологических изменений твердых зубных тканей, обработанных лазером и ротационными инструментами с помощью ультразвукового электронного микроскопа
- Banerjee A., Watson T.F., Kidd E.A. Dentine caries excavation: a review of current clinical techniques//Br. Dent. J. 2000. Vol. 188(9). P. 476-482.
- Yazici A.R., Ozgunaltay G., Dayangac B.A. Scanning electron microscopic study of different caries removal techniques on human dentin//Operative Dentistry. 2002. Vol. 27. P. 360-366.
- Стефанович M. Скениращ електронно -микроскопски анализ на ефектите от въздействието на Er:YAG лазер и на конвенционалния метод върху дентина//СДК и НУС. 2005. Vol. 4(1). Р. 153-156.
- McCormack S.M. Scanning electron microscope observations of C02 laser effects on dental enamel//J. Dent. Res. 1995. Vol.74. P. 1702-1708.
- Palamara J. The effect on the ultrastructure of dental enamel of excimerdye, argonion and C02 lasers//Scanning Mi-crosc. 1992. Vol.6. P. 1061-1071.
- Li Z.Z., Code J.E., Van De Merwe W.P Er: YAG laser ablation of enamel and dentin of human teeth: determination of ablation rates at various fluences and pulse repetition rates//Lasers Surg. Med. 1992. Vol. 12. P. 625-30.
- Park N.S. Changes in Intrapulpal Temperature After Er: YAG Laser Irradiation//Photomedicine and Laser Surgery. 2007. Vol. 25. P. 229-232.
- Eguro T. Energy output reduction and surface alteration of quartz and sapphire tips following Er: YAG laser contact irradiation for tooth enamel ablation//Lasers in Surgery and Medicine. 2009. Vol.41. P. 595-604.
- Eberhard J. Cavity size difference after caries removal by a fluorescence-controlled Er: YAG laser and by conventional bur treatment//Clin. Oral Investig. 2008. Vol. 12(4). P. 311-318.
- Matsumoto M. Morphological and Compositional Changes of Human Dentin after Er: YAG Laser Irradiation//J. Oral Laser Applications. 2003. Vol. 3. P. 12-20.
- Ceballos L. Bonding to Er-YAG-laser-treated dentin//J. Dent. Res. 2002. Vol. 81 (2). P. 119-122.
- Baraba A. Ablative Potential of the Erbium-Doped Yttrium Aluminium Garnet Laser and Conventional Handpieces: A Comparative Study//Photomedicine and Laser Surgery. 2009. Vol. 11. P. 465-504.
- Chinelatti MA. Effect of erbium: yttrium-aluminum-garnet laser energies on superficial and deep dentin microhardness//Lasers Med Sci. 2008. Vol. 34. P. 135-140.
- Raucci-Neto W., Chinelatti M.A., Palma-Dibb R.G. Ablation Rate and Morphology of Superficial and Deep Dentin Irradiated with Different Er: YAG Laser Energy Levels//Photomedicine and Laser Surgery. 2008. Vol. 26. P. 523-529.
- Kinoshita J., Kimura Y, Matsumoto K. Comparative study of carious dentin removal by Er, Cr: YSGG laser and Carisolv//J. Clin. Laser Med. Surg. 2003. Vol. 21. P. 307-315.
- Banerjee A., Kidd E.A.M., Watson T.F. Scanning electron microscopic observations of human dentine after mechanical caries excavation//Journal of Dentistry. 2000. Vol. 28. P. 179-186.
