Patterns of population's self-preservation behavior: research approaches and building experience

Author: Korolenko Aleksandra V.
Journal: Economic and Social Changes: Facts, Trends, Forecast @volnc-esc-en
Section: Social development
Article in issue: 3 (57) т.11, 2018.
Free access
As countries make their epidemiological transition, the contribution of behavioral risk factors to population’s health is increased; they include challenges of low physical and medical activity, diet and sleep violations, imbalance of work and rest, tobacco and alcohol consumption, and high stress loads. In Russia, the situation is complicated by incomplete epidemiological transition, as well as increased morbidity and mortality from endogenous and quasi-endogenous causes. The purpose for the article is to analyze methodological approaches to studying the self-preservation behavior and build models describing it for the population of the Vologda Oblast. Russian scholars A.I. Antonov, V.A. Borisov, I.V. Zhuravleva, L.S. Shilova, G.I., Ivakhnenko, T.V. Shushunova, and A.E. Lugovoy attempt to highlight the patterns of self-preservation behavior taking into account all or some of its elements (needs, attitudes, motives and actions), but not considering them in a single system...
Self-preservation behavior, socio-demographic approach, behavior patterns, behavioral risk factors
Short address: https://sciup.org/147224058
IDR: 147224058 | UDC: 314.4 | DOI: 10.15838/esc.2018.3.57.16
Text of the scientific article Patterns of population's self-preservation behavior: research approaches and building experience
Over the past 50 years the majority of developed countries have demonstrated great success in fighting against non-infectious causes of death (mainly circulatory, respiratory, and digestive diseases, tumors, external causes), which has helped increase the average age of death from these groups of causes, as well as significantly increase the population’s life expectancy thereby triggering the “second epidemiological revolution” [1].
The observed upward trends in mortality rate and population’s life expectancy are explained from the standpoint of the concept of epidemiological transition which is a historically conditioned shift of one type of pathology defining the nature of population’s morbidity and mortality, towards another; of one structure of diseases and causes of death towards another. As communicable and parasitic diseases as key causes of morbidity and mortality are replaced by chronic noninfections diseases, the contribution of behavioral risk factors to health formation inevitably increases; these factors pose the challenges of low physical health and activity, diet and sleep violation, work and rest imbalance, tobacco and alcohol consumption, high stress loads.
In Russia, the situation is complicated by the fact that, on the one hand, the epidemiological transition is incomplete, i.e., the features of the “traditional” structure of pathology remain: morbidity and mortality rates from communicable and parasitic diseases, digestive and respiratory diseases remain at a high level; on the other hand, there is an increase in morbidity and mortality from endogenous and quasi-endogenous causes (cardiovascular diseases, neoplasms) [2, p. 475]. However, the state pays close attention to reducing mortality from cardiovascular diseases and cancer in recent years: modern cardiology and cancer centers are built, years of fighting against these diseases are announced (for example, 2015 is the Year of fighting against cardiovascular diseases), large conferences and symposia devoted to these issues are held annually. However, the problem of mortality from external causes due to its smaller extent becomes a secondary concern. The objectives of reducing mortality from road traffic injuries are top priority here [3, p. 896], but despite all the importance of this cause, it only causes 10% of all deaths from external causes [2, p. 493]. Other external causes – injuries with uncertain intentions, suicide, murder and alcohol poisoning – directly characterize the psychosocial state of the society and its individuals [4, p. 51].
Both at the federal and regional level, health development programs for 2014–2020 are being implemented, where mortality rates from
Table 1. Target indicators of mortality reduction in the framework of federal and regional health development programs in 2014–2020 according to data for 2017
In this regard, the issues of studying the characteristics of behavior determining the individual’s health and lifespan in order to identify the strategies and opportunities to manage them are of particular importance. In the scientific community, this type of demographic behavior is called self-preservation behavior. This term was first used in Russian sociology and sociological demography at the beginning of the 1970–s (studies by A.I. Antonov, V.M. Medkov, V.A. Borisov, V.A. Zotin, T.V. Lifar, I.V. Zhuravleva, L.S. Shilova, E.B. Babin, M.S. Bednyi, L.V. Shibut) to describe the individual’s willingness to preserve their own life and health, live until old age2. During the same period, Yu.P. Lisitsin, O.V. Grinitsyn, A.M. Izutkin, I.F. Matyushin in the framework of the medical approach used the term “healthy lifestyle” (or “the way of life which promotes health”), reflecting the characteristics of people’s behavioral activity related to their own health. Foreign experts began to study people’s self-preservation behavior in the 1970–s, first in the framework of the concept “health” (“health promotion”) [5, p. 8] and later – in the context of similar terms: “health behavior”, “health-related behavior”, and “healthy lifestyle” [6, pp. 42– 43; 7, pp. 262–263].
In modern research, the following terms are used as synonyms to “self-preservation behavior”:
– “health behavior” (M.V. Volkova [8]);
– “health-preserving behavior” (A.V. Ze-lionko [9], A.A. Shabunova, V.R. Shukhatowich [10], N.V. Yakovleva [11]);
– “vital behavior” (V.V. Yumaguzin, N.B. Vinnik [3]);
– “health-related behavior” (E.I. Rasskazova, T.Yu. Ivanova [12]).
– Moreover, terms characterizing destructive practices opposite to self-preservation, became widespread:
– “self-destructive behavior” (T.V. Shipu-nova [13], V.G. Rezapkina [14]);
– “deviant health behavior” (M.V. Volkova [8]).
Despite different conceptual frameworks, their nature is reduced to a priority of the value of health, motivation, and its preservation for individuals [15, p. 23].
Since in modern conditions the behavioral factor associated with the individual’s attitude to their own health and life expectancy is becoming increasingly important in determining population’s morbidity and mortality, it is important to study the individual characteristics and strategies of self-preservation behavior. The purpose of this paper is to analyze methodological approaches to studying selfpreservation behavior and construct models describing it for the population of the Vologda Oblast taking into account the inextricable relation of all its components.
Theoretical aspects of the research
In the scientific community, selfpreservation behavior (SPB) is studied in the framework of medical, psychological, and sociodemographic approaches. The medical approach equates this type of behavior with a healthy lifestyle (hygienic or sanitary behavior), i.e. activities of an individual or groups of individuals most characteristic of specific socio-economic, political, environmental and other conditions aimed to preserve, improve and promote health [16]. The proponents of this approach see medical activity as a key component of SPB, while other parameters are considered secondary, subordinated to it (Tab. 2). The medical approach only takes into account the individual’s health-reserving activities, rather than their motives and values of self-preservation.
In social psychology, self-preservation (health-preserving) behavior is interpreted from three directions: 1) as an act of decisionmaking; 2) as a staged process; 3) as an activity. Most often it is considered as a specific regulatory activity to ensure an optimal level of individual’s health [11]. In the framework of the first direction, foreign researchers M. Becker and L. Maiman developed a health belief model back in the 1970–1980-s. It describes the behavior of a subject as a result adding together individual health-related knowledge: perceived risk, awareness of the severity of the problem, the possible benefits and obstacles to adopting this pattern of behavior [17]. The key components of the model of planned behavior of M. Fishbein and A. Ajzen are assessment of expectations, validity of action, rules guiding the subject, and control of perceived behavior [18].
The most popular models considering selfpreservation behavior as a staged process are precaution adoption process model by H. Weinstein and P. Sandman [19] and the transtheoretical model of behavior change by J. Prochaska and C. DiClemente [20]. According to them, the stages of SPB represent qualitatively different types of behavior, ideas, and experiences. The factors mediating transitions between stages vary depending on the stage an individual is currently at [11].
In Ru-ssian social psychology, the study of self-preservation behavior is based on the activity-based approach is used. N.V. Yakovlev
Table 2. Theoretical approaches to interpretation of self-preservation behavior and its structure
Approach Scholars Interpretation of SPB SPB components Medical Yu.P. Lisitsyn, O.V. Grinitsyn, A.M. Izutkin, I.F. Matyushin Self-preservation behavior is equivalent to a healthy lifestyle (or hygienic behavior), i.e. the activity of an individual, groups of individuals, most characteristic of specific socio-economic, political, environmental and other conditions aimed at preserving, improving, and promoting health 1. Key element – medical activity 2. Subordinate elements (healthy lifestyle standards): - occupational health and safety; - quitting smoking and alcohol abuse; - psychohygienic and therapeutic self-help; - physical activity; - balanced diet; - timely use of medical resources; - first aid skills. Psychological M. Becker, L. Maiman, М. Fishbein, А. Ajzen, J. Prochaska, C. DiClemente, N.V. Yakovleva, N.N. Ulanova, L.G. Ulyaeva Self-preservation behavior (often called healthsaving behavior) is considered in different ways: - as an act of decision-making (M. Becker, Л. Maiman, М. Fishbein, А. Ajzen) - as a staged process (Weinstein N., Sandman P., J. Prochaska, C. DiClemente) - as an activity (N.V. Yakovleva, N.N. Ulanova, L.G. Ulyaeva) Main SPB components: 1. motivation; 2. assessment of current state of health (self-assessment); 3. fixation; 4. system of actions; 5. control of results. Sociodemographic A.I. Antonov, V.M. Medkov, V.A. Borisov, V.A. Zotin, T.V. Lifar’, I.V. Zhuravleva, L.S. Shilova, E.B. Babin, L.V. Shibut, I.S. Vyalov, G.A. Ivakhnenko, V.Ya. Shklyaruk, L.Yu. Ivanova, A.A. Shabunova Self-preservation behavior is a system of actions and relations of an individual aimed at preserve health during the whole life and extending lifespan. 1. Needs (in health and longevity). 2. Attitudes (self-reported health, value of health, socially approved standards). 3. Motives. 4. Actions (measures): - medical activity; - physical activity; - balance of work and rest; - sexual behavior; - diet control; - work and rest balance control; - bad habits; - counteracting stress. Sources: compiled by the authors using: Lisitsyn Yu.P., Izutkin A.M., Matyushkin I.F. Medicine and humanism. Moscow: Meditsina, 1984; Yakovleva N.V. Health-preserving human behavior: socio-psychological discourse. Personality in a changing world: health, adaptation, development: electronic scientific journal, 2013, no. 3. Available at: ; Yakovleva N.V. Study of individual differences in health-preserving activity of an individual. Experimental psychology, 2015, vol. 8, no. 3; Glanz K., Rimer B., Viswanath K. Health behavior and health education: theory, research and practice. San Francisco: Jossey-Bass, 2008. P. 42; Antonov A.I. Microsociology of a family (research methodology of structures and processes): high school manual. Moscow: Publishing House “Nota Bene”, 1998. 360 p.; Shilova L.S. Transformation of the female model of self-preservation behavior. Sociological research, 2000, no. 11, pp. 134–140.
distinguishes five components of health preserving behavior: motivation, self-reported health, fixation on healthcare; system of health preserving actions, control of results [21, p. 203]. The advantage of this approach is that it recognizes the priority of the value-motivational component in self-preservation. However, the psychological approach does not consider SPB as demographic behavior and therefore does not imply its relation with demographic processes.
Within the framework of the sociodemographic approach which has been successfully developed in Russian science and was formed into a concept of self-preservation behavior, such behavior is understood as a system of actions and relations of an individual aimed at preserving health during the whole life and extending the lifespan. Moreover, the proponents of this approach, defining the components of the SPB structure, use the value-motivational approach based on the category of social psychology (motivation, attitudes, motives, and actions), on the one hand. On the other hand, they interpret self-preservation behavior as a kind of demographic behavior and recognize its contribution to determining key demographic parameters: population’s mortality, life expectancy and birth rate.
At the first stage of developing the concept of self-preservation behavior (1970–1980s), the researchers’ attention when studying reproductive behavior was focused on the needs, namely on identifying the preferred (ideal, desired, and expected) lifespan. Further, the concept of SPB was developed in works by I.S. Vyalov, I.V. Zhuravleva, L.S. Shilova, G.A. Ivakhnenko, V.J. Shklyaruk, L.Y. Ivanova who developed a structure and a system of indicators of self-preservation behavior, and identified mediating factors. The issues of its determination and the relation of its components were covered by E.M. Andreev, V.M. Shkolnikov, V.A. Biryukov [7, p. 264]. The problem of preserving health in population’s individual activities was being developed by Belarusian sociologists and demographers V.R. Shukhatowitz, T.N. Shushunova, N.A. Baranovskii, and A.A. Zlotnikov.
The most reasonable and developed approach to studying self-preservation behavior, its factors and structural components is, in our opinion, the socio-demographic approach based on principles of social psychology related to SPB content and on theoretical development of sociology and demography, which recognize self-preservation behavior as part of demographic behavior, which determines the performance of the processes of fertility and mortality. In our work, we follow this approach and consider the model of self-preservation behavior as a set of needs, attitudes, motives, and specific actions of an individual to maintain and strengthen their own health.
Methodology
A.I. Antonov made a great contribution to the development of the methodology of studying self-preservation behavior. In 1980– 1986, he and a team of scientists from Lomonosov Moscow State University, and later the Institute of Sociology in the regions of the former USSR conducted large-scale sociological surveys to identify the population’s motives and attitudes to preserve individual health and longevity. The research of A.I. Antonov, V.M. Medkov, V.K. Zotin, T.V. Lifar, I.V. Zhuravleva, L.S. Shilova, E.B. Babin, L.V. Shibut was based on the scheme of dispositional regulation of behavior [22], according to which the results of self-preservation behavior depend not only on the living conditions, but also on how they are subjectively determined by AN individual in everyday situations.
Most often, when studying self-preservation behavior scientists are limited to considering its individual aspects such as the place of health in the system of life values, self-reported health, medical and physical activity, bad habits, stress resistance of the body, diet, etc., which does not form the idea of the existing total behavior strategies. Attempts to build models describing the individual’s health preserving actions less often made, were based on various features.
Table 3. Methodological approaches to identifying models of self-preservation behavior
|
Scholars |
Features of model elements |
Models |
|
A. I. Antonov, V. A. Borisov, I. V. Zhuravleva, L. S. Shilova, L. Y. Ivanova |
|
“Pessimistic” and “optimistic” Male and female SPB pattern |
|
T.V. Shushunova |
|
B+P+S+ “Positivist” B+P+S- “Realist” B+P-S+ “Career person” B-P+S+ “Activist” B-P+S- “Conformist” B-P-S+ “Moralist” B+P-S- “Consumer” B-P-S- “Negativist” |
|
E.A. Yugova |
|
Unstable model Semi-strict model Stable model Sustainable/health preserving model |
|
Sources: compiled by the author using: Antonov A.I. Microsociology of a family (research methodology of structures and processes). Moscow: Nota Bene, 1998. P. 315; Shilova L.S. Transformation of a female model of self-preservation behavior. Sociological research , 2000, no. 11, pp. 134–140; Shushunova T.N. Self-preservation behavior of students: sociological analysis (on the example of Minsk universities) . Minsk: Pravo I ekonomika, 2010. 114 p.; Yugova E.A. Formation of health preserving behavior among students of higher educational institutions. Herald of SPbSU , 2012, no. 2, p. 32. |
||
For example, in studies by A.I. Antonov3, V.A. Borisov, I.V. Zhuravleva, L.S. Shilova, G.I. Ivakhnenko such indicators are the nature of respondents’ fixation on ideal, desired, and expected lifespan (pessimists and optimists) and gender (male and female models) [23; 24; 25]; in works by T.V. Shushunova – the nature of motivation (negative or positive) and level of orientation when forming self-preservation (biological, social, and psychological) [5]; in works by E.A. Yugovaya – absence/presence of bad habits, rational diet, physical activity, work and rest balance, hygiene and prevention of diseases (unstable, semi-strict, stable, and sustainable models [26]; Tab. 3 ).
The advantage of these classifications is that all of them use sociological methods to obtain information about SPB characteristics and take into account the value-motivational aspect of health preservation. However, they do not reflect the components of self-preservation behavior (needs, attitudes, motives, and actions) in a single system. That is why the purpose of the study is to develop models that would take into account the key elements of SPB based on data of sociological surveys.
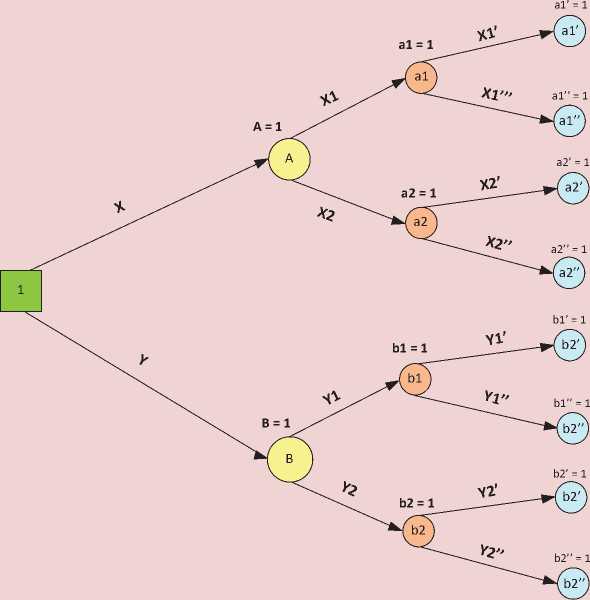
To build these models we use the decision tree method based on a schematic representation of a decision-making process branching under certain conditions. This method is used when the result of one decision forces an individual to make the next decision which, in turn, affects the third, the fourth one, etc., until the final result is achieved4.
The elements of decision tree are nodes and branches of decision-making options ( Fig. 1 ). The branches denote possible alternative decisions that can be made and possible outcomes that result from these decisions. The nodes denote the points where decisions are made.
Figure 1. The decision tree
Decision 1 (branch 1)
Decision 2 Decision 3
(branch2) (branch3)
"Nodes"
(points of decision-making)
Source: compiled by the author
In the present study, the following sequence of decisions is made: value of health – need for health and motivation to care for it – measures to preserve and promote health. We assume that the value of health characterizes the basic attitude of an individual towards this category. The value of health in an ideal situation depends on the need for it and the motivation to care for it, which, in turn, affects specific self-preservation actions implemented by an individual.
Thus, the starting point of decision-making is defining the place of health in the system of life values reflecting the individual’s attitude to health as the main condition for sustaining life (Tab. 4). Depending on the distribution of respondents’ answers to the question “What is the main value for you? “ two “branches” are singled out: people who consider health the main value and those who do not consider it a life priority. The next “node” implies the presence (or absence) of motivation to healthcare, which acts as an incentive for an individual to take action to promote health and prolong life [5, p. 17]. According to whether a person has any social (desire to have children, be an example for the loved ones, look good, unwillingness to be a burden), psychological (unwillingness to deal with medical institutions, need for good health, fear of illness, deterioration of health) or economic (desire to preserve and improve the ability to
Table 4. Indicators for building the model of self-preservation behavior
|
Elements of SPB |
Questions |
Indicators for building decision-making nodes |
|
Attitudes to health |
What is your main value in life?* |
1. Share of respondents who chose health as the main value |
|
2. Share of respondents who did not choose health as the main value |
||
|
Need for selfpreservation and motivation to care for health |
What motivates you to take care of your health?** |
|
|
4. Share of respondents who are not motivated to care for their health (who chose the answer “I do not care for my health”) |
||
|
Actions (measures) taken to preserve and promote health |
What do you personally do to preserve and strengthen your health?** |
self-fulfillment;
|
|
6. Share of respondents who do not take any measures to preserve and strengthen their health (who chose the answer “I do not take any measures on purpose”) |
||
|
* The answer implies the choice of up to 3 options. ** The answer implies the choice of all options applied. Source: compiled by the author. |
||
work, achieve significant goals) motives that encourage to care for health, we distinguish the following “branches”: people motivated to care for health and those who are not motivated to care for it. At the same time, in our opinion, the presence of motives simultaneously reflects the need to promote health or, in the case of the answer “I do not care for health”, the absence of such. Further, the division of “branches” is based on the distribution of answers to the question about actions taken to preserve and strengthen one’ health: people who implement such measures and those who so not comply with any measures.
When the “tree” is built all decisions are indicated on it, the share of each option is calculated, their values are put down over the “branches”. In our study, the weights are determined based on the distribution of respondents’ answers to special questionnaire questions reflecting individual elements of selfpreservation behavior (Tab. 4). According to the provisions of the probability theory, each “node” of decision-making equals 1, therefore, each “branch” acquires a certain weight expressed in unit fractions.
The prevalence of models of selfpreservation behavior, i.e. the share of each model in their total number, is calculated through multiplying the weights of all “branches” of decision-making to final “nodes” (see Fig. 1):
ш = X^X1■XI' ■ ... ■ 100%
, where ω is prevalence of a model, X, X1, X1' are weights of the decision-making tree branches (%).
The limitations of the method of subjective assessments include the possible of distortion of information provided by the respondents under the influence of factors such as the quality of a questionnaire, professionalism of an interviewer, time and place of a survey, quality of the procedure itself, etc. This should be taken into account when interpreting the results of a sociological study [27]. Despite these disadvantages the method is considered reliable and is recommended by the WHO for monitoring the population’s health status as an additional tool for assessing public health [28, p. 51]. Data of sociological surveys make it possible to analyze the characteristics of people’s self-preservation behavior, their individual strategies, driving motives and factors.
Designing individual strategies of selfpreservation behavior will help identify risk factors of population’s unhealthy condition and further assess the possibility of their management influence, which, through a number of special measures, will contribute to the provision of desirable parameters of population quality, and consequently, reproduction process.
Research results
The study is based on data of a stage of monitoring the physical health of the population in the Vologda Oblast conducted by the Vologda Research Center of the Russian Academy of Sciences in 20165. The monitoring study has been carried out in the region since 2002 in order to identify the key factors in public health including the parameters of people’s self-preservation behavior, in particular, the level of physical and medical activity, diet, balance of work and rest, presence of bad habits in everyday life, as well as assessment of availability and quality of healthcare services, and living conditions (environmental, housing, labor).
Constructing the “decision tree” has helped identify eight possible variants of models of selfpreservation behavior (Fig. 2). As it turned out, the most common strategy among the population of the Vologda Oblast is characterized by recognizing health as the main value, motivation to care for health and implementation of measures to promote health (57%). However, 14% of respondents care for their health and take certain actions although health is not part of their life values (model 5). Nevertheless, 11% of respondents, despite the fact that they understand the value of their own health and
5 Monitoring physical health of the population in the Vologda Oblast is carried out in the cities of Vologda, Cherepovets, and eight municipal districts of the Vologda Oblast. The target quota sample size – 1500 respondents. The sample representativeness is ensured by the following conditions: the proportion between urban and rural population, the proportion between residents of different types of settlements (rural settlements, small and medium cities), proportions of the age and sex structure of adult population in the region. The sample error is less than 5%. Technical processing of information is conducted through SPSS and Excel.
Figure 2. Models of self-preservation behavior of the population in the Vologda Oblast
Take measuresto preserve and improve health
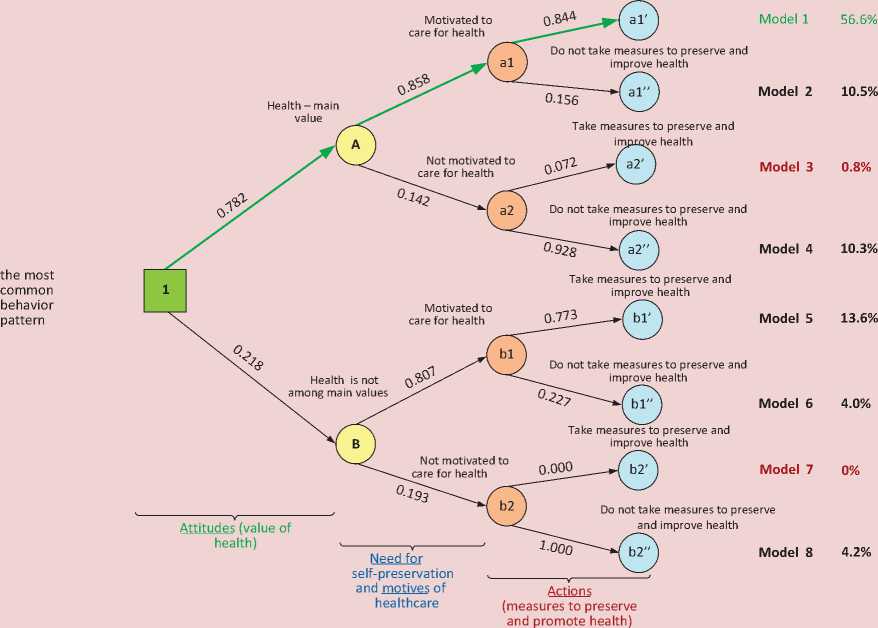
Source: compiled by the author according to the monitoring data on physical health of the population of the Vologda Oblast in 2016.
are motivated to care for it, do not implement any health preserving measures (model 2). 10% of respondents combine the importance of health with lack of motivation for a healthy lifestyle and special self-preservation actions (model 4).
Other behavior patterns were less common. 4% of respondents are characterized by the most unfavorable model 8: health is not considered the main value, there are no incentives and practices of to preserve health. It is noteworthy that the surveyed population do not demonstrate a fixed strategy of individual’s behavior where they use measures to promote and preserve health but do not value it and are not motivated to promote it.
Next consider the correlation between behavioral determinants and the components of self-preservation. Currently the main causes of the most common non-communicable diseases (cardiovascular, cancer, chronic respiratory and diabetes) are preventable behavioral risk factors such like tobacco use, lack of physical activity, poor diet and alcohol abuse . They cause four main metabolic (physiological) changes: high blood pressure, overweight (obesity), hyperglycemia, and hyperlipidemia [29, C.]. 13].
According to data of the sociological survey, among the residents in the Vologda Oblast who do not consider health one of key life values compared with people who consider it a value,
Table 5. Correlation of key risk factors with components of self-preservation behavior
|
Risk factors |
Value of health |
Motivation to care for health |
Measures to preserve and promote health |
|||
|
Health is the main value |
Health is not among main values |
Motivated |
Not motivated |
Taken |
Not taken |
|
|
Alcohol |
||||||
|
Drink |
62.2 |
69.7 |
60.7 |
81.2 |
59.2 |
75.3 |
|
Do not drink |
37.8 |
30.3 |
39.3 |
18.8 |
40.8 |
24.7 |
|
Smoking |
||||||
|
Smokers |
28.8 |
41.3 |
26.0 |
62.4 |
21.7 |
55.8 |
|
Non-smokers |
71.2 |
58.7 |
74.0 |
37.6 |
78.3 |
44.2 |
|
Physical activity |
||||||
|
1. Walking for more than 30 minutes |
||||||
|
Every day or several days a week |
79.5 |
62.5 |
78.4 |
61.8 |
80.9 |
63.3 |
|
Rarely (several times a month) |
6.3 |
9.9 |
7.1 |
7.0 |
6.9 |
7.4 |
|
No |
14.2 |
27.6 |
14.6 |
31.1 |
12.2 |
29.3 |
|
2. Physical education and sports |
||||||
|
Every day or several days a week |
17.5 |
22.9 |
21.6 |
2.6 |
24.1 |
5.2 |
|
Rarely (several times a month) |
10.4 |
11.1 |
11.3 |
6.2 |
11.8 |
7.5 |
|
No |
72.2 |
66.0 |
67.1 |
91.2 |
64.1 |
87.3 |
|
3. Running |
||||||
|
Every day or several days a week |
7.1 |
8.5 |
8.5 |
1.3 |
9.4 |
2.6 |
|
Rarely (several times a month) |
7.0 |
9.5 |
8.5 |
2.2 |
8.4 |
5.4 |
|
No |
85.9 |
82.0 |
82.9 |
96.5 |
82.2 |
92.0 |
|
4. Morning exercises |
||||||
|
Every day or several days a week |
20.5 |
16.1 |
22.5 |
3.5 |
25.8 |
4.2 |
|
Rarely (several times a month) |
10.9 |
13.9 |
13.4 |
1.3 |
13.8 |
5.9 |
|
No |
68.7 |
70.0 |
64.2 |
95.2 |
60.4 |
89.9 |
|
Diet |
||||||
|
Keep to a healthy diet |
72.2 |
61.8 |
77.5 |
27.9 |
84.3 |
34.6 |
|
Do not keep to a healthy diet |
27.8 |
38.2 |
22.5 |
72.1 |
15.7 |
65.4 |
|
Source: data of monitoring study of physical health of the population in the Vologda Oblast in 2016. |
||||||
the share of those who drink alcohol (70% against 62%), smoke (41% against 29%), do not keep to a proper diet (38% against 28%), and do not walk for more than 30 minutes (28% against 14%; Tab. 5 ) is higher.
Among the respondents who are not motivated to care for health, compared with motivated people, the share of those who drink alcohol (81% against 61%), smoke (62% against 26%), do not keep to a proper diet (72% against 23%) and do not engage in basic physical activity: walking for more than 30 minutes
(31% against 15%), physical education and sports (91% against 67%), running (97% against 83%), morning exercises (95% against 64%) is also significantly higher.
Naturally, respondents who do not take any measures to preserve and strengthen their health are more likely to drink alcohol (75% against 59%) and smoke (56% against 22%) compared to those who take measures; they are much more likely to ignore any healthy eating diet (65% against 16%) and all types of physical activity (walking – 29% against 12%, physical education and sports – 87% against 64%, running – 92% against 82%, morning exercises – 90% against 60%).
Thus, the absence of health in the system of life values, low motivation, passive use of selfpreservation measures contribute to the fact that destructive health-related behavioral patterns become widespread: alcohol abuse, smoking, malnutrition and low physical activity. 21% of respondents do not see health as one of their life priorities, 15% – are not motivated to live healthy lives, and 29% – do not take any action to preserve and promote their health.
Based on the revealed specific features of self-preservation behavior of the Vologda Oblast residents we believe it is appropriate to introduce the measures to reduce behavioral risk factors, preserve and promote health, which are aimed at increasing the value of health, the population’s motivation to lead a healthy lifestyle, and applying health preserving measures. These include the following:
-
1. Development and implementation of a target regional program for behavioral risk factors prevention: such activities should be focused on different models of self-preservation behavior.
-
2. Introduction of a monitoring system of self-preservation behavior of the population in a region in the framework of implementing the target program of behavioral risk factors prevention for a number of SPB indicators: selfreported health, assessment of importance of health factors, the place of health in the system of values, motivation to lead a healthy lifestyle, measures to preserve and promote health, physical activity, nutrition, bad habits.
-
3. Raising population’s awareness through the media of the importance of preserving and promoting health, the impact of negative risk factors on health and the ways to avoid
-
4. Development and implementation of educational programs aimed to form a responsible attitude to health, a healthy lifestyle and prevent behavioral risk factors in the programs of educational institutions (preschool, schools, secondary vocational and higher educational institutions).
-
5. Engaging public organizations in activities in the sphere of public health and accounting of public initiatives.
-
6. Engaging population in physical activities, tourism and sports, recreation and leisure activities, prevention of health risk factors through specialized mass events at the regional and municipal level. At the same time, the systematic approach nature to these activities is of fundamental importance.
them. Due to the increasing role of social networks and blogosphere in promoting public information, including health-related topics [30], their use as tools for forming selfpreservation attitudes and practices among the residents of the region seems promising.
Conclusion. The study has led to a number of important conclusions.
First, the most reasoned theoretical and methodological approach to studying selfpreservation behavior of the population is the socio-demographic approach which, on the one hand, uses the principles of social psychology in the content of SPB components (needs, attitudes, motives, actions), on the other hand, recognizes self-preservation behavior as part of demographic behavior that determines the performance of the processes of fertility and mortality.
Second, the existing scientific approaches to constructing the models of self-preservation behavior take into account all or some of its elements, but not always consider them in a single system.
Third, the proposed method of decision tree for constructing models of self-preservation behavior, which covers all its structural components, namely attitudes, motives, needs, and practices of healthy lifestyle, helps track the self-preservation strategies formed among the population.
Fourth, 57% of people in the Vologda Oblast demonstrate an SPB model characterized by recognizing health as the main value, motivation to care for it and use of healthsaving measures. However, other models contain certain behavioral risks. Thus, 21% of respondents do not see health as one of their life priorities, 15% – are not motivated to live healthy lives, and 29% – do not take any action to preserve and promote their health.
Fifth, absence of health in the system of life values, low motivation to care for it, passive use of self-preservation measures are directly related to the spread of self-destructive practices such as alcohol abuse, smoking, malnutrition and low physical activity.
Despite the fact that the objectives set at this stage of the study have been implemented, there are still issues to be addressed: what are the strategies of population’s behavior taking into account the implementation of specific selfpreservation practices; what is the difference between SPB models of various sociodemographic population groups; what are the possibilities of management influence on each of them. The next stage of monitoring study of physical health of the population in the Vologda Oblast is planned for 2018. The results will help deepen the study through a more detailed study of models of self-preservation behavior at the level of individual population groups, expanding the range of behavioral risk factors under study.
References Patterns of population's self-preservation behavior: research approaches and building experience
- Vishnevskii A.G. Mortality in Russia: the second epidemiologic revolution that never was. Demograficheskoe obozrenie=Demographic review, 2014, no. 4. Available at: http://demreview.hse.ru/2014-4/150227447.html (accessed: 06.02.2018)..
- Vishnevskii A.G., Vasin S.A. Causes of deaths and priorities of the mortality reduction policy in Russia. Ekonomicheskii zhurnal VShE= Higher School of Economics economic journal, 2011, no. 4, pp. 472 496..
- Yumaguzin V.V., Vinnik M.V. Mortality from external causes in Russia and in the EOCD countries: assessment of premature loss and conditions of their reduction. Vestnik Bashkirskogo universiteta=Bulletin of Bashkir University, 2015, no. 3 (20), pp. 896-902..
- Korolenko A.V., Morev M.V. About the consequences of demographic suicide deaths. Suitsidologiya=Suicidology, 2015, no. 4, pp. 48-60..
- Shushunova T.N. Samosokhranitel’noe povedenie studencheskoi molodezhi: sotsiologicheskii analiz (na primere minskikh vuzov) . Minsk: Pravo i ekonomika, 2010. 114 p.
- Glanz K., Rimer B., Viswanath K. Health behavior and health education: theory, research and practice. San Francisco: Jossey-Bass, 2008. 552 p.
- Obrazhei O.N., Podval’skaya V.S. Actual character of the study of people’s self-protective behavior. Sotsiologicheskii al’manakh=Sociology almanac. 2010, no. 1, pp. 262-269..
- Volkova M.V. Zdravookhranitel’noe povedenie naseleniya v usloviyakh rossiiskikh sotsial’no-ekonomicheskikh transformatsii: dis. na soisk. uch. st. kand. sotsiolog. nauk: 22.00.03 . Saratov, 2005. 269 p.
- Zelionko A.V. Obosnovanie organizatsionno-profilakticheskikh meropriyatii po sovershenstvovaniyu sistemy formirovaniya zdorov’esberegayushchego povedeniya i uluchsheniyu kachestva zhizni naseleniya: dis. na soisk. uch. st. kand. med. nauk: 14.02.03 . Saint Petersburg, 2016. 193 p.
- Shabunova A.A., Shukhatovich V.R., Korchagina P.S. Health saving activity as a health-promoting factor: the gender aspect. Ekonomicheskie i sotsial’nye peremeny: fakty, tendentsii, prognoz=Economic and social changes: facts, trends, forecast, 2013, no. 3 (27), pp. 123-132..
- Yakovleva N.V. Health-human behavior: socio-psychological discourse. Lichnost’ v menyayushchemsya mire: zdorov’e, adaptatsiya, razvitie=An individual in the changing world: health, adaptation, development, 2013, no. 3, pp. 70-79..
- Rasskazova E.I., Ivanova T.Yu. Motivational models of health behavior: the problem of the "gap" between intention and action. Psikhologiya: zhurnal Vysshei shkoly ekonomiki=Psychology. Journal of the Higher School of Economics, 2015, vol. 12, no. 1, pp. 105-130..
- Shipunova T.V., Kovaleva A.A. Behavior concerning health in the context of anomical adaptation. Vestnik Sankt-Peterburgskogo universiteta. Seriya 12: Psikhologiya. Sotsiologiya. Pedagogika=Vestnik of Saint Petersburg University. Series 12: Sociology, 2011, no. 2, pp. 343-350..
- Rezapkina V.G. Self-preservation behavior: causes and prevention. Akademicheskii vestnik Akademii sotsial’nogo upravleniya=Academic bulletin of Academy of Public Administration, 2017, no. 2 (24), pp. 18-24..
- Vangorodskaya S.A. Self-preservation behavior: the term content in domestic sociology. Srednerusskii vestnik obshchestvennykh nauk=Central Russian journal of social sciences, 2017, vol. 12, no. 4, pp. 20-29. DOI: 10.22394/2071-2367-2017-12-4-20-29
- Lisitsyn Yu.P., Izutkin A.M., Matyushkin I.F. Meditsina i gumanizm . Moscow: Meditsina, 1984. 278 p.
- Becker M.H., Maiman L.A. Sociobehavioral determinants of compliance with health and medical care recommendations. Medical care, 1975, vol. 13, pp. 10-24.
- Ajzen I., Fishbein M. Understanding attitudes and predicting social behavior. Englewood Cliffs, New Jersey: Prentice Hall, 1980. 278 p.
- Weinstein N., Sandman P. The precaution adoption process model. Health behavior and health education. San Francisco: Jossey-Bass, 2002, pp. 121-143.
- Prochaska J., DiClemente C., Velicer W., Rossi J. Standardized, individualized, interactive, and personalized self-help programs for smoking cessation. Health psychology, 1993, vol. 12, pp. 399-405.
- Yakovleva N.V. The study of individual differences in health-activity of the person. Eksperimental’naya psikhologiya=Experimental psychology, 2015, vol. 8, no. 3, pp. 202-214..
- Samoregulyatsiya i prognozirovanie sotsial’nogo povedeniya lichnosti: dispozitsionnaya kontseptsiya . 2nd edition, extended. Moscow: TsSPiM, 2013. 376 p.
- Shilova L.S. Transformation of the female self-preservation behavior model. Sotsiologicheskie issledovaniya=Sociological studies, 2000, no. 11, pp. 134-140..
- Zhuravleva I.V. Self-preservation behavior of teenagers and sexually transmitted diseases. Sotsiologicheskie issledovaniya=Sociological studies, 2000, no. 5, pp. 66-74..
- Ivakhnenko G.I. The health of Moscow students: analysis of self-preservation behavior. Sotsiologicheskie issledovaniya=Sociological studies, 2006, no. 7, pp. 78-81..
- Yugova E.A. Forming the model of self-preservation behavior among students of higher educational institutions. Vestnik Sankt-Peterburgskogo universiteta. Seriya 12: Psikhologiya. Sotsiologiya. Pedagogika=Vestnik of Saint Petersburg University. Series 12: Sociology, 2012, no. 2, pp. 29-34..
- Korolenko A.V., Kalachikova O.N. Physical health in subjective assessments of the population of the vologda oblast: territorial aspect. Sotsial’noe prostranstvo=Social area, 2017, no. 1. Available at: http://sa.vscc.ac.ru/article/2186 (accessed: 09.02.2018)..
- Shabunova A.A. Zdorov’e naseleniya v Rossii: sostoyanie i dinamika: monografiya . Vologda: ISERT RAN, 2010. 408 p.
- Nakitanda A.O., Shvireb G., Armstrong T. The increasing burden of non-communicable diseases and the role of physical activity. Profilakticheskaya meditsina=The Russian journal of preventive medicine and public health, 2014, no. 1, pp. 12-17..
- Gruzdeva M.A. Tools for shaping people’s self-preservation practices: social networks and the blogosphere. Sotsial’noe prostranstvo=Social area, 2017, no. 4. Available at: http://sa.vscc.ac.ru/article/2378 (accessed: 15.02.2018)..
