Physiological regulatory Mechanisms of Arterial Blood Pressure during Stress

Автор: Guliyeva Sh.
Журнал: Бюллетень науки и практики @bulletennauki
Рубрика: Медицинские науки
Статья в выпуске: 7 т.12, 2026 года.
Бесплатный доступ
Stress represents the physiological and psychological response of the organism to internal and external stimuli. Among the many physiological alterations that occur during stress, the regulation of arterial blood pressure is of particular clinical significance. Under the influence of stressors, the sympathetic nervous system becomes activated, leading to increased secretion of catecholamine hormones such as adrenaline and noradrenaline. These hormones accelerate heart rate, increase myocardial contractility, and cause vasoconstriction, resulting in elevated arterial blood pressure. The renin–angiotensin–aldosterone system (RAAS) and antidiuretic hormone (ADH) are simultaneously activated, regulating water–salt balance and contributing to blood pressure homeostasis. Baroreceptors located in the carotid sinus and aortic arch detect changes in vascular wall tension and relay signals to the central nervous system. The central nervous system then coordinates vasomotor responses. Cardiopulmonary baroreceptors are additionally sensitive to changes in blood volume and participate in the activation of hormonal regulatory pathways. Increased respiratory rate, skeletal muscle tension, and accelerated metabolism during stress are recognized indicators of the acute defense response. Prolonged emotional stress, however, imposes an additional burden on the cardiovascular system and raises the risk of hypertension. During short-term stress, these physiological alterations are largely adaptive and serve protective functions. Chronic stress, by contrast, may contribute to the development of arterial hypertension, cardiovascular disease, sleep disturbances, fatigue, impaired concentration, and psychoemotional disorders. Effective stress management and blood pressure monitoring are therefore essential for preserving long-term health.
Stress, arterial blood pressure, sympathetic nervous system, baroreceptors, hypertension, antidiuretic hormone
Короткий адрес: https://sciup.org/14138603
IDR: 14138603 | УДК: 612.133+616.12-008.331.1 | DOI: 10.33619/2414-2948/128/27
Физиологические механизмы регуляции артериального давления при стрессе
Стресс представляет собой физиологический и психологический ответ организма на внутренние и внешние стимулы. Среди многочисленных физиологических изменений, возникающих при стрессе, особое клиническое значение имеет регуляция артериального давления. Под воздействием стрессоров активируется симпатическая нервная система, что приводит к усиленной секреции катехоламинов — адреналина и норадреналина. Эти гормоны учащают сердечный ритм, повышают сократимость миокарда и вызывают вазоконстрикцию, что ведёт к повышению артериального давления. Одновременно активируются система ренин-ангиотензин-альдостерона (РААС) и антидиуретический гормон (АДГ), регулирующие водно-солевой баланс и способствующие поддержанию гомеостаза артериального давления. Барорецепторы, расположенные в каротидном синусе и дуге аорты, регистрируют изменения напряжения сосудистой стенки и передают сигналы в центральную нервную систему, которая, в свою очередь, координирует вазомоторные реакции. Кардиопульмональные барорецепторы дополнительно чувствительны к изменениям объёма крови и участвуют в активации гормональных регуляторных путей. При краткосрочном стрессе данные изменения являются адаптивными и выполняют защитную функцию. Хронический стресс, напротив, может способствовать развитию артериальной гипертензии, сердечно-сосудистых заболеваний, нарушений сна, усталости, снижения концентрации внимания и психоэмоциональных расстройств.
Текст научной статьи Physiological regulatory Mechanisms of Arterial Blood Pressure during Stress
Бюллетень науки и практики / Bulletin of Science and Practice
UDC 612.133 + 616.12-008.331.1
The term stress originates from the Latin word strictia. During the seventeenth century, it was used to denote disaster, distress, and grief [2].
In the eighteenth and nineteenth centuries, it came to be associated with resistance against adverse conditions. Hans Selye was the first researcher to introduce the concept into medicine, defining stress as the body’s nonspecific response to any demand or stimulus. Although organisms display broadly similar stress-related responses, the factors that trigger stress vary among individuals. When a person encounters a threat, excitement, or fear, the hypothalamus sends signals that initiate a cascade of physiological reactions: hormone production increases, glucose and lipids enter the bloodstream, respiration and heart rate accelerate, blood pressure rises, muscles tense, and blood vessels dilate. These changes constitute the body’s self-protective response. Individual perception of stress is variable; differences in personal perception influence both the nature of symptoms and the magnitude of the response. According to the General Adaptation Syndrome theory, the stress response proceeds through three stages: the alarm stage, the resistance stage, and the exhaustion stage [1].
When an individual encounters a stressor, the sympathetic nervous system is activated and the body mounts a defense response. The physiological alterations observed during the alarm stage include: increased respiratory rate, providing greater oxygen delivery to tissues; elevated blood pressure, accelerated heart rhythm, and enhanced blood circulation; increased skeletal muscle tension; suppression of digestive activity; release of stored glucose and lipids from the liver and muscles into the bloodstream, facilitating energy production; increased erythrocyte count, enhancing oxygen delivery to tissues and the brain; activation of the coagulation cascade, increasing blood clotting readiness as part of the acute-phase response; heightened sensory perception, increasing awareness of potential external threats [4].
If the body’s defense mechanisms are sufficient, physiological functions return toward baseline and the stress response progresses to the resistance stage. Stress symptoms may be categorised as follows: physical symptoms; psychological and emotional symptoms; social symptoms; cognitive symptomsn [3].
Physical symptoms include palpitations, elevated blood pressure, insomnia, back and chest pain, weight changes, persistent fatigue, tremors, headaches, and dryness of the throat and mouth. Psychological and emotional symptoms include feelings of emptiness, resentment, the perception that life is meaningless, anger, depression, anxiety, and persistent pessimism. Social symptoms include withdrawal, hypersensitivity, communication difficulties, and loneliness. Cognitive symptoms include difficulty concentrating, forgetfulness, and fear. Stress responses create a predisposition for various diseases and may contribute to conditions such as migraine, hypertension, and cardiovascular disorders.
Blood pressure is the force exerted on vessel walls when the heart pumps blood through the circulation. It comprises two components: systolic and diastolic blood pressure. The maximum arterial pressure generated during ventricular contraction is referred to as systolic blood pressure (SBP), whereas the minimum pressure recorded before ventricular contraction is termed diastolic blood pressure (DBP). In healthy individuals, normal blood pressure is approximately 120/80 mmHg, giving a pulse pressure of 40 mmHg.
Elevated central venous pressure is considered a sign of cardiovascular insufficiency and may occur in right ventricular dysfunction, tricuspid valve insufficiency, and related pathological states. Low venous pressure may be observed in individuals with severe weight loss, infectious diseases, acute or chronic intoxication, and neurogenic vascular hypotonia. Several mechanisms participate in the regulation of arterial blood pressure: afferent pathway (receptors); central nervous system; efferent pathway. Receptors constitute the sensory component that detects physiological changes. Vascular baroreceptors detect sudden alterations in blood pressure and transmit signals to the central nervous system, which processes this information and coordinates an appropriate vasomotor response via the efferent pathway. Baroreceptors are classified into two main types: arterial baroreceptors and cardiopulmonary baroreceptors. Two major arterial baroreceptors are present in the systemic circulation. The carotid sinus baroreceptor responds to both increases and decreases in blood pressure, transmitting afferent signals via the glossopharyngeal nerve (CN IX). The aortic arch baroreceptor responds primarily to elevations in blood pressure and transmits signals through the vagus nerve (CN X). Both receptor types respond to mechanical deformation of the vascular wall. Stretching of the vessel wall stimulates sensory nerve endings in the tunica adventitia, generating action potentials that are transmitted to the nucleus tractus solitarius, where autonomic cardiovascular responses are coordinated. Activation of the aortic baroreceptor during elevated blood pressure inhibits efferent sympathetic activity [5].
When blood pressure falls, reduced baroreceptor depolarisation decreases action potential frequency, leading to increased sympathetic activation and reflex restoration of blood pressure. Cardiopulmonary baroreceptors are located in the large veins, pulmonary arteries, and the walls of the right atrium and ventricle within the low-pressure venous system. The compliance of the venous system is approximately thirty times greater than that of the arterial system, meaning that changes in blood volume substantially affect venous baroreceptor activity. Reduced firing frequency from these low-pressure receptors stimulates secretion of antidiuretic hormone (ADH), renin, and aldosterone, exerting compensatory effects on arterial blood pressure. The regulation of baroreceptor-mediated blood pressure control can be illustrated through the following diagram (Figure 1) [6].
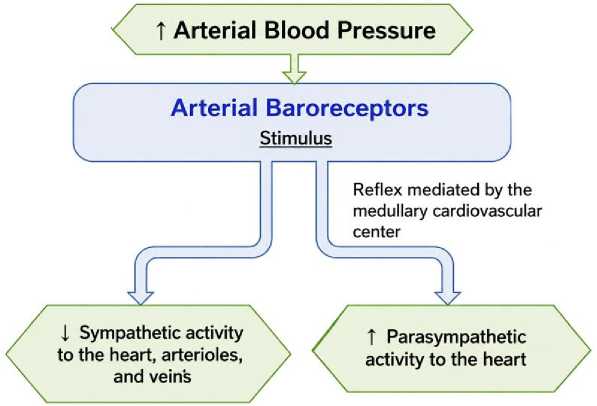
Figure 1. Baroreceptor reflex regulation of arterial blood pressure
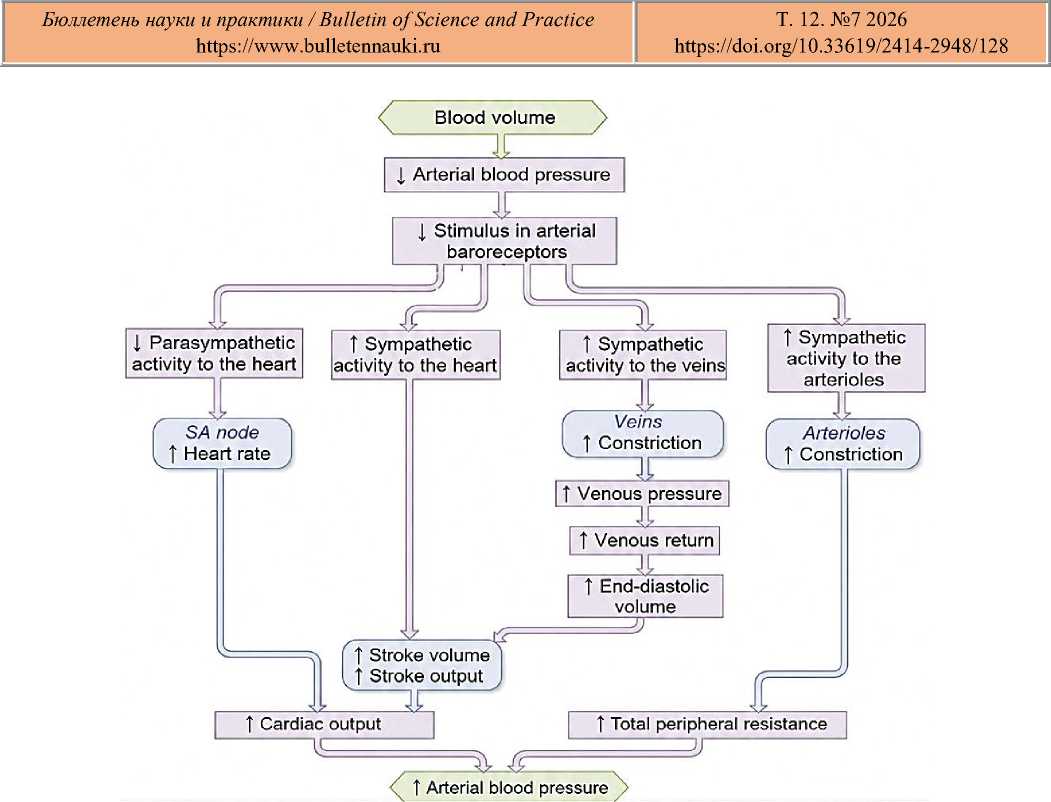
Figure 2. Baroreceptor reflex pathways in response to reduced blood volume
Antidiuretic hormone (ADH), also known as vasopressin, is synthesised in the supraoptic and paraventricular nuclei of the hypothalamus. ADH synthesis and secretion are regulated by several factors: increased serum osmolarity acting on hypothalamic osmoreceptors; reduced blood volume causing decreased stretch of low-pressure baroreceptors; decreased arterial pressure leading to reduced stretch of high-pressure baroreceptors. ADH synthesised in the hypothalamus travels along neuronal axons and is stored in the posterior pituitary gland. Its primary action is to increase water reabsorption in the collecting ducts of the nephron, thereby increasing plasma volume and arterial blood pressure. At higher concentrations, ADH also produces moderate vasoconstriction, further increasing peripheral resistance and arterial pressure [7, 8].
The renin-angiotensin-aldosterone system is among the principal regulators of arterial blood pressure, acting through coordinated hormonal mechanisms that govern both arterial pressure and peripheral resistance. The cascade begins with the synthesis and secretion of renin from the juxtaglomerular cells of the kidney, stimulated by decreased blood pressure, sympathetic nervous system activation, and reduced sodium ion concentration in the distal convoluted tubules. Circulating renin cleaves angiotensinogen—a protein continuously produced by the liver — to yield angiotensin I. Angiotensin-converting enzyme (ACE), secreted by pulmonary capillary endothelial cells, then converts angiotensin I into the biologically active angiotensin II.
Angiotensin II raises arterial pressure through several mechanisms: potent vasoconstriction of systemic arterioles, increasing peripheral resistance; constriction of efferent glomerular arterioles, helping to maintain glomerular filtration rate; stimulation of sodium reabsorption in renal tubules, with passive water reabsorption following the osmotic gradient; stimulation of aldosterone secretion from the adrenal cortex.
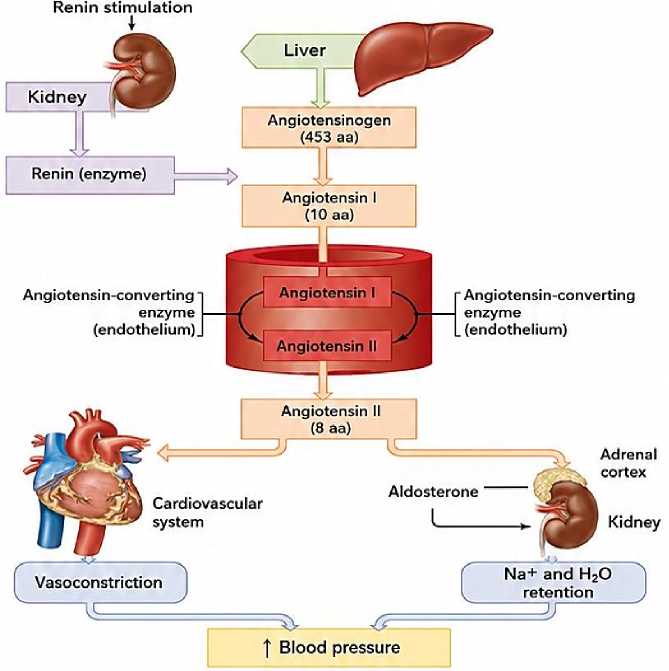
Figure 3. Mechanism of the renin–angiotensin–aldosterone system in the physiological regulation of arterial blood pressure
ACE also degrades bradykinin; accordingly, ACE inhibitors such as Captopril reduce blood pressure by preventing the formation of angiotensin II. Aldosterone, synthesised in the adrenal cortex, regulates sodium reabsorption and potassium excretion in the distal renal tubules by increasing the activity and expression of the Na⁺/K⁺-ATPase pump. The resulting sodium reabsorption creates an osmotic gradient that drives passive water reabsorption, ultimately increasing blood volume and arterial pressure. The primary physiological function of these regulatory mechanisms is to maintain adequate perfusion pressure for body tissues. During acute hypotension, baroreflex mechanisms act to restore arterial pressure and preserve blood supply to vital organs [9].
Chronic hypertension may develop as a consequence of sustained physiological dysregulation. In most cases it does not arise from a single cause but from the interaction of multiple risk factors; this form is classified as essential hypertension. Clinical data indicate that approximately 95% of hypertension cases fall into this category [10, 11].
Timely treatment is critically important because uncontrolled hypertension may lead to severe complications affecting target organs such as the brain, heart, and kidneys. Pharmacological management of essential hypertension commonly includes ACE inhibitors, calcium channel blockers, angiotensin receptor blockers, and thiazide diuretics.
Conclusion
The regulation of arterial blood pressure during stress involves the integrated activity of the sympathetic nervous system, baroreceptor reflexes, the RAAS, and ADH. During acute stress, these mechanisms are adaptive and collectively maintain tissue perfusion. Under conditions of chronic stress, however, the same pathways may contribute to the development of sustained hypertension and associated cardiovascular complications. Understanding the interplay between these systems is relevant to the clinical management of stress-related hypertension and highlights the importance of both pharmacological and non-pharmacological approaches to blood pressure control.
