Problems and prospects of personnel support of the Moscow healthcare system

Author: Yarasheva Aziza V., Aleksandrova Olga A., Medvedeva Elena I., Alikperova Natalya V., Kroshilin Sergei V.
Journal: Economic and Social Changes: Facts, Trends, Forecast @volnc-esc-en
Section: Social development
Article in issue: 1 т.13, 2020.
Free access
The article is devoted to the study of the problem of personnel support in the capital's healthcare. Its research is connected, on the one hand, with the analysis of statistical data on the medical personnel staff in organizations, which allows building (on the basis of theoretical model) the prognosis of availability/ absence of staff (according to different indicators). On the other hand, it is connected with the analysis of motivational factors affecting entrance into the profession, long successful professional career, processes of “burnout” and retirement from the profession. In the article, we present the results of the scientific project, conducted in 2019, on studying problems of the quality of the staff in the Moscow's system of healthcare within the implementation of the current capital standard of providing medical assistance. The usage of statistical, mathematical, and sociological research methods allowed us to identify not only the characteristic features of the available labor resources, but also the prospects of personnel support of Moscow healthcare institutions. The forecast for the development of the personnel potential of Moscow's medical organizations is based on statistical data for the last 5 years (2014-2018). The prospects of changing of the age and gender structure of employees (doctors and nursing staff), the number of doctors of the most popular specialties in the capital are shown. On the basis of sociological surveys, we reveal the level of satisfaction of medical employees (depending on working experience) with working conditions (salaries in hospitals and clinics and its correspondence with the work performed). We also define main types of doctors and nursing staff's workload, which act as motivational factors affecting the quality of medical assistance. On the basis of expert opinions, we show material and non-material factors that determine the increase of the personnel potential of the Moscow's healthcare system.
Healthcare, personnel support, working conditions, motivations, prospects of personnel needs, moscow
Short address: https://sciup.org/147225435
IDR: 147225435 | UDC: 331.104; | DOI: 10.15838/esc.2020.1.67.10
Text of the scientific article Problems and prospects of personnel support of the Moscow healthcare system
One of the most important components of the improvement of the quality of medical services, provided to the population, is the personnel support of medical organizations. It causes the need for a timely and accurate forecast of the personnel needs of the city’s healthcare system. However, the reliability of such forecast depends not only on the available corps of medical employees of different profiles and planned indicators of certain specialists’ training, but also on how busy doctors, middle and junior medical staff of health care institutions are today, and are they satisfied with their work and ready to remain loyal to the chosen profession.
Degree of the problem’s development
Due to the fact that the medical personnel is one of the most important structural elements of the healthcare system, it is studied not only within the academic and industry science, but also on the level of international organizations – WHO, the World Bank, OECD, etc. In particular, WHO report on labor resources of the healthcare system (2006) recorded the shortage of “the required number of health workers in the required places”, revealed the reasons of the deficit and misbalances (poor planning, including the inability to collect relevant and up-to-date data necessary for making management decisions; insufficient investment in medical education, professional development and retraining; poor working conditions and low salaries, lack of career prospects, etc.) [1], and started the development of several WHO documents. One of them is the Global Strategy on Human Resources for Health addressed to management and planning bodies, vocational education institutions, employers, trade unions, etc. [2]. After highlighting the human resources problems, faced by countries with different income levels, the Strategy pointed to a universal “comprehensive package of measures” for ensuring “decent employment” – a necessary condition for optimal distribution of healthcare workers across territories and sectors (public/ private) and improving their performance: job security; adequate premises and instruments for work; allowable load; allowances for working in difficult conditions; opportunities for professional development; clear career paths; social support in the form of housing grants, education grants, etc. Besides, low-and middle-income countries are encouraged to strengthen the potential of medical schools and colleges and improve the quality of education through accreditation of educational institutions, certification of diplomas, and investments in teaching staff (a “priority area for investments”) to ensure the necessary number and competence of teachers. High-income countries are encouraged to strengthen measures aimed at developing the competencies of healthcare workers, helping graduates find job, and involving workers from other industries in the healthcare sector to perform functions that do not require a long period of training.
It is also worth noting WHO Resolutions, adopted before the approval of the Global Strategy, on increasing the scale of healthcare employees training (2009); strengthening nursing and midwifery (2006), primary healthcare personnel (2009), and other Statistical indicators of healthcare personnel provision and the analysis of main trends in training and movement of personnel are reflected in the materials published by the OECD [3], reports of WHO regional offices [4].
Considering problems of planning personnel’s needs and optimal organization of available healthcare employees in less economically prosperous countries, under the WHO authority, the Handbook on monitoring and evaluation of human resources for health was released [5]. It proposes organizational mechanism and analytical instruments for collecting and analyzing data on medical staff, including successful experience of several countries. The author’s approach is based on the concept of “duration of labor activity”, which considers labor resources within training, attracting and retaining, which involves the monitoring of the dynamics of the labor market for each stage and the prospects of healthcare employees. The main goal of the management structures at the first stage is the preparation of the sufficient number of competent and motivated employees and their optimal organization, which requires efficient planning, budgeting, and management of the process of creating powerful educational institutions and improving recruitment mechanisms. At the stage of active labor activity, efforts should be aimed at ensuring the availability, competence (including communicational) and productivity of employees, which requires the assessment of medical personnel from different workplaces in the context of the national labor market.
It is worth noting a special section of Recommendations, dedicated to qualitative research methods. Due to the fact that the study of healthcare personnel is a fairly new field of research, which does not have a solid theoretical foundation, numerous quantitative studies are mostly descriptive. Hence, it is expedient to use qualitative methods that allow us to better understand the working conditions and motives of healthcare employees’ behavior and to improve methods for evaluating their activities.
The possibilities of qualitative methods are illustrated by numerous studies on the role of professional identity, motivation, etc. in the “survival” strategies used by medical professionals within healthcare reform [6, 7, 8]; the impact of professional insecurity on the attitude to patients and the quality of clinical care [9]; obstacles to attracting and retaining nurses [10] and the possibility of imposing broader functions on them [11]; the nature of part-time work among medical workers [12] and the impact of financial and nonfinancial incentives on the behavior patterns of doctors, simultaneously employed in the public and private sectors [13, 14]; features of secondary employment, which determines employment in a state institution as the main job [15], etc.
We should also mention the manual on assessing key factors in strategic planning of human resources (2009), released under WHO authority [16]. The authors emphasize that the goal of human resources policy in healthcare, given in the WHO Report of 2006, which is “to train the right people with the right skills, put them in the right place and give them the right task” and, at the same time, respond flexibly to emergencies, solve current problems, and predict future challenges, cannot be achieved in all countries using the same templates. In this regard, the approaches to the development and usage of tools, which allow adequate assessment of the situation and selection of the best solutions for improving the personnel support in healthcare sphere in specific conditions, are proposed. In addition, on the basis of several studies, for example [17], it is shown that the development of personnel policy, which can overcome the “human resources crisis”, requires consideration of “cross-cutting issues”, related to the demand for medical employees, associated risks, motivation, compatibility, etc.
Russian authors study healthcare personnel problems through analyzing the dynamics of changes in the number and composition of medical employees in the international context [18], studying the factors that determine the movement of medical personnel, the quality of their work [19], and the problems of forming corps of managers [20] and a personnel reserve [21], etc.
Informational and methodological basis of the research
The article presents results gained in 2019 during the implementation of the project “The development of the personnel potential of the capital’s healthcare system” using sociological
(quantitative and qualitative) statistical and mathematical methods. An array of questionnaires (551 units), collected as part of a survey of employees of healthcare institutions under the city’s jurisdiction (polyclinics and hospitals for children and adults), was formed. It is consistent with the official statistics of the Moscow Healthcare Department (MHD). A series of in-depth structured interviews (N=15) was conducted with the heads of clinics and outpatient institutions under the MHD jurisdiction, the management of medical universities and colleges, and FE institutions.
The forecast of the development of the capital’s healthcare personnel potential was based on statistical data for the last 5 years (2014–2018), during which the personnel policy has undergone the most significant changes; the forecast horizon is 2020, 2025, and 2030. The assessment of the balance of labor resources was carried out on the basis of comparing the number of medical workers with various indicators of the form no. 30 “Information about a medical organization” (in wording of the Rosstat order no. 483, dated 03.08.2018). Formalized forecasting methods (extrapolation, moving average, expo-nential smoothing, least squares), as well as the method of individual expert assessments, were used to build the forecast model and the forecast itself [22]. At the first stage, gender and age indicators were calculated for categories “doctors” and “secondary medical personnel” (hereinafter – SMP). Then the personnel resources shortage forecast for categories “doctors”, “SMP”, and “junior medical personnel” (hereinafter – JMP) was built. The forecast of medical personnel staffing (percentage) was calculated for the same categories of medical employees using the formula
ФЛ (занятых) (штатных) , where УФЛ – indicator of doctors staffing (individuals);
ЧД(занятых) – number of positions in the organization (employed);
ЧД(штатных ) – number of positions in the organization (staff).
In turn, the forecast of the deficit by positions (people) and the relative deficit by positions (percentage) for the same three categories of healthcare employees was calculated according to the formulas:
ДД =
ЧД
(штатных)
ЧД
(занятых)
where ДД – deficit indicator by positions;
ЧД (занятых) – number of positions in the organization (employed);
ЧД (штатных) – number of positions in the organization (staff).
ОД Д = Д Д / ЧД
(штатных)
where ОДД –relative deficit indicator by positions;
ДД – deficit indicator by positions;
ЧД (штатных) – number of positions in the organization (staff).
Results of the research
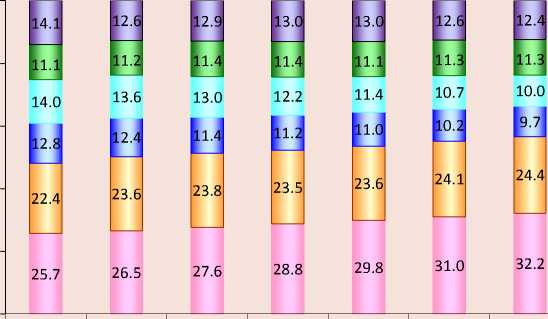
The forecast calculated on the basis of the developed forecast model indicates the following prospects. The share indicators for age groups show the trend of doctors’ “rejuvenation”: by 2030, doctors under the age of 45 will have made up 2/3 of the total number; doctors of preretirement and retirement age will constitute 8.3 and 6.7%, respectively ( Fig. 1 ).
In comparison with doctors of the “SMP” category, the age structure will change slightly. There is no trend towards “rejuvenation”, the share of the “46–50 years old” cohort will increase by 7%, the “51–55 years old” cohort will also increase slightly, the share of pensioners and pre-retirees will be 4.8 and 7.1%, respectively ( Fig. 2 ).
-
Figure 1. Forecast for the doctors’ age structure, %
100%
0%
80%
60%
40%
20%
2014 2015 2016 2017 2018 2019 2020
11.0
8.6
8.1
13.6
6.7
8.3 6.3
15.5 о
27.0
31.7
30.2

32.9
Doctors
-
□ 61 and more
-
□ 56-60
-
□ 51-55
-
□ 46-50
-
□ 36-45
-
□ until 36
Source: own compilation on the basis of the results of the scientific project “Development of the personnel potential of the capital’s healthcare system”, 2019.
2025 2030
-
-
Figure 2. Forecast for the SMP’s age structure, %
100%
8.8
7.8
8.6
8.0
8.2
7.9
7.7
6.8
80%
60%
40%
20%
0%
9.6
12.8
13.1
26.0
29.7
9.3
12.5
13.3
27.5
29.5
9.9
9.7
9.5
9.6
9.7
8.2
SMP
12.1
11.5
11.2
10.5
13.5
14.2
14.9
15.3
9.9
I
16.0 о
11.3
21.2
27.1
28.9
27.2
27.1
27.7
28.0
25.5
13,6

□ 61 and more
□ 56-60
□ 51-55
о 46-50
26.7
27.6
□ 36-45
29.4
29.2
28.9
28.7
27.0
п until 36
Source: own compilation on the basis of the results of the scientific project “Development of the personnel potential of the capital’s healthcare system”, 2019.
As for the gender composition of healthcare employees, it remains unchanged: among doctors, the ratio of 30% of men to 70% of women will remain; among MSP, there are even fewer men – about 10%.
Prognostic indicators of the number of people – main employees in occupied positions in short- (2020), medium- (2025) and long-term
-
(2030) perspective show the trend of the reduction of the number of healthcare employees in all categories, although in varying degrees. The number of doctors will change slightly in the longterm perspective; at the same time, the number of JMP, with the retention of current trends, will be reduced in 8 times in comparison with 2014, and in 1.2 times – in comparison with 2018 ( Tab. 1 ).
Table 1. Forecast for the number of natural persons’ key employees in occupied positions, people
Category
2014
2016
2018
2020
2025
2030
Doctors
48289
43777
45689
43144
42624
41203
Secondary medical personnel
88832
79173
71320
61148
59984
57828
Junior medical personnel
25760
18451
3570
2830
3520
3130
Source: own compilation on the basis of the results of the scientific project “Development of the personnel potential of the capital’s healthcare system”, 2019.
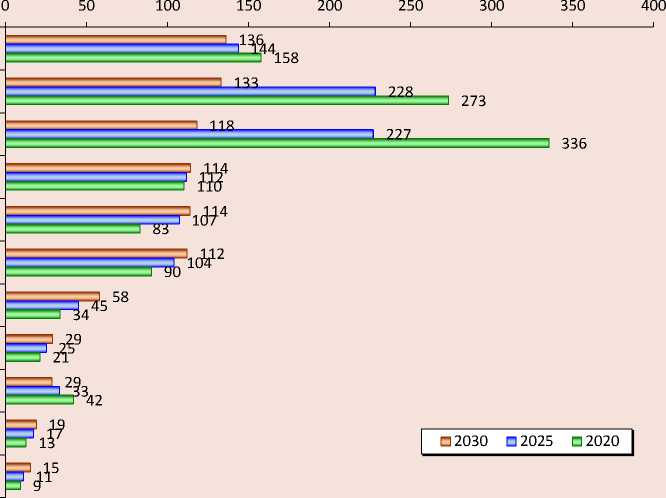
For a more detailed analysis, 44 positions (specialties) of doctors were allocated, 22 – SMP and 2 – JMP, the choice of which was determined by the possibilities of statistical analysis and forecast1. Then the doctors’ data set was divided into 4 groups (11 positions/specialties in each) on the basis of the degree of the demand for a particular specialty in the short-, medium- and long-term perspective. In figures 3 and 4 , the forecast for the first (most popular specialties) and the fourth (most non-popular) groups is presented.
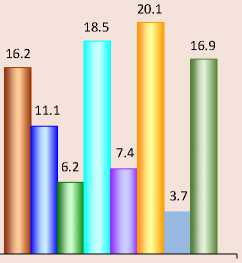
According to the forecast, general practitioners (family doctors) will be the most numbered medical personnel. If current trends retain, their number will have tripled by 2030. In terms of future demand, the next are pediatricians and anesthesiologists-resuscita-tors, whose number will increase by 1.4 times ( Fig. 3 ).
If current trends remain, surgeons (plastic and thoracic) and adolescent psychiatrists will be least demanded ( Fig. 4 ).
-
Figure 3. Forecast for the number of doctors of the most demanded specialties, people
General practice (family) doctors
Pediatricians
Anesthesiologists-resuscitators
Obstetrician-gynaecologists
District pediatricians
Ultrasound diagnostics
Radiologists
Neurologists
Surgeons
Psychiatrists
Ophthalmologists

Source: own compilation on the basis of the results of the scientific project “Development of the personnel potential of the capital’s healthcare system”, 2019.
-
Figure 4. Forecast for the number of doctors of the least demanded specialties, people
Psychotherapists
Dentists (for children)
Orthopedic dentists
Cardiologists (for children)
Oral and maxillofacial surgeons
Dentists
Oncologists (for children)
Genetics
Thoracic surgeons
Psychiatrists for adolescents
Plastic surgeons
Source: own compilation on the basis of the results of the scientific project “Development of the personnel potential of the capital’s healthcare system”, 2019.
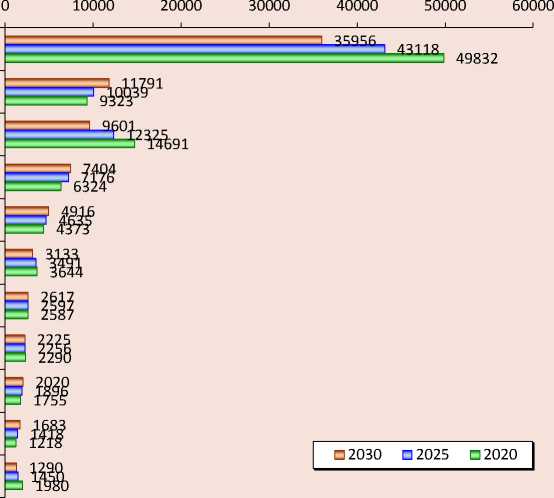
Figure 5. Forecast for the number of SMPs of the most demanded specialties, people
Medical nurses
Feldshers
Ward (post) nurses
Ambulance feldshers
Procedural
Senior
Obstetricians
Operating
Precinct pediatricians
General practice (family) doctors
Precinct pediatricians
Source: own compilation on the basis of the results of the scientific project “Development of the personnel potential of the capital’s healthcare system”, 2019.
Secondary medical personnel were divided in 2 groups (11 positions/specialties in each one). As a result, nurses will become the most popular staff, despite the overall decrease of their number. The next most demanded doctors will be feldshers and ward (post) nurses ( Fig. 5 ).
The forecast for the second group of SMP specialties showed a significant decrease of the need for dietary and medical nurses (ambulance feldshers), as well as the need for the secondary medical personnel working with dentists. As for JMP, there is still a trend of reduction of the number of orderlies and nursing assistances – in 2 and 1.3 times, respectively.
The short-term calculation of staffing indicators (individuals) is positive: the doctors’ indicator will increase to 79.6%, SMP’s indicator will remain within 78%, and JMP’s indicator will reach 67%. For a more detailed analysis, the entire array of data on doctors was divided into 4 groups, formed according to the degree of doctors’ staffing (individuals) of a particular specialty in the short-, medium-, and long-term perspectives. As the result, the less stuffed positions in the short-term perspective are positions of plastic surgeons (28.0%), psychotherapists (30.8%), and adolescent psychiatrists (60%). The situation with staffing is slightly better in the short-term perspective in the fourth group: cardiologists (92.3%), ophthalmologists (93.1%), endocrinologists (94.7%), and, especially, district pediatricians (almost 100%).
As for the projected shortage of personnel, in the long term perspective, if current trends retain, the deficit of doctors will remain almost unchanged (13.8%), the SMP deficit will grow slightly (up to 15.6%), and JMP deficit will increase quite noticeably (up to 32.1%). While dividing the array of doctors’ data into 4 groups, which were formed according to the decreasing degree of doctors’ shortage in a particular specialty in the short-, medium-, and long-term perspectives, it was revealed that in the first group, while maintaining current trends in the long-term perspective, the deficit of psychotherapists (72.7%), plastic surgeons (72.6%), and child psychiatrists (55.5%) will increase quite noticeably. The situation is better in the fourth group: if the current trends retain, the deficit of obstetricians-gynecologists in the long term perspective will be 3.4%, and the shortage of maxillofacial and thoracic surgeons will reach 2.7%.
In SMP group, the three most deficit specialties are secondary medical personnel working with dentists (38.0%), with district pediatricians (21.3%), and masseurs (20.0%). In the second SMP group (the SMP data set was divided according to the same principle as doctors’ data, into 2 groups), the deficit is not expected in the long-term perspective among operating nurses, feldshers, and ambulance feldshers (6.4, 4.1, and 2.5%). As for JMP, the deficit of junior nurses will remain almost the same (16%), but the shortage of orderlies will noticeably increase (49.3%).
Thus, the forecast suggests that, in the longterm perspective, public health institutions in the capital may face certain personnel imbalances. In such a situation, it is important to understand how the doctors, working in them, feel, because their well-being affects the nature of the personnel movement (movement between the public and private sectors, between outpatient institutions and hospitals; loyalty to the profession) and the quality of provided medical assistance.
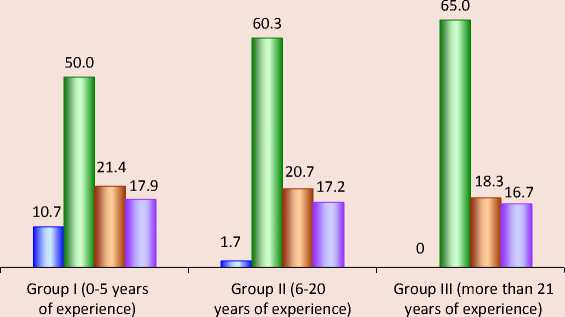
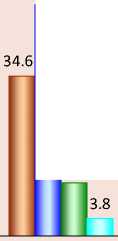
According to the results of the survey, the level of satisfaction with the amount of employees’ salaries in hospitals and clinics significantly differs: if only 12.0% of doctors and 18.4% of nurses were dissatisfied with salaries in polyclinics, almost a third of hospitals’ employees were not happy with their salaries (31.6% of doctors and 37.7% of nurses). Apparently, this is caused by their ideas on differences in responsibilities and labor efforts among specialists of the same profile working in the hospital and on the primary level. For example, more than a third of hospital employees (35.5% of doctors and 38.2% of nurses: a third of them have 0–5 years of the work experience) believe that their salaries are less than their labor contribution. In polyclinics, 19.6% of doctors and 25.0% of nurses chose this answer (which, however, is also not enough). The experience positively affects doctors’ attitudes – the higher it is, the more doctors think that their labor contribution is equal to the material reward: in hospitals, 46.9% of doctors with 6–20 years of experience and 59.3% of those with more than 20 years of experience think so; in polyclinics, this trend is even more noticeable (Fig. 6). In contrast, nurses have a negative attitude toward their experience. In hospitals, 22.2% of nurses with little experience are not satisfied with the ratio of their labor contribution and monetary remuneration (44% of respondents in this group consider it fair). With the growth of experience, the percentage of dissatisfied personnel doubles: 44.2% of nurses with 6–20 years of experience and 37.2% of those with more than 20 years of experience are not happy with their salaries. In polyclinics, the situation is quite similar.
The feeling of discrepancy between monetary remuneration and labor contribution appears, because, according to the results of the study, the majority of employees of the Moscow hospitals and polyclinics get very busy and tired at the main job. It is even more relevant for primary doctors than for their colleagues in hospitals (Tab. 2) .
Figure 6. Influence of the work experience on representations of doctors in polyclinics concerning the correspondence of labor contribution and material remuneration, %
Doctors in polyclinics
-
□ Payment is higher than Your labor contribution
-
□ Payment is approximately equal to Your labor contribution
-
□ Payment is less than Your labor contribution
-
□ Hesitate to answer
Source: own compilation on the basis of the results of the scientific project “Development of the personnel potential of the capital’s healthcare system”, 2019.
50.0
11.5
Table 2. Distribution of health employees’ answers to the question “How do You assess your workload, the intensity of work at the main job?”, %
|
Personnel |
Quite busy, very tired |
Normal workload, work within own capabilities |
Total |
|
|
Hospitals |
Doctors |
63.7 |
36.3 |
100 |
|
Nurses |
75.5 |
24.5 |
100 |
|
|
Polyclinics |
Doctors |
71.2 |
28.8 |
100 |
|
Nurses |
72.4 |
27.6 |
100 |
|
|
Source: own compilation on the basis of the results of the scientific project “Development of the personnel potential of the capital’s healthcare system”, 2019. |
||||
Figure 7. Main types of doctors’ workload in hospitals, %
Doctors in polyclinics
Group I (0-5 years of experience)
37.5
26.1
20.5
12.5
1.1 2.3
Group II (6-20 years of experience)
38.9
18.5
27.8
11.1
1.9 1.9
Group III (more than 21 years of experience)
-
□ Large amount of medical work
-
□ Large amount of work with medical and other documentation
-
□ You have to perform the functions of missing or absent personnel
-
□ Helping your work colleagues
-
□ Other
-
□ You have normal or small workload
Source: own compilation on the basis of the results of the scientific project “Development of the personnel potential of the capital’s healthcare system”, 2019.
According to data, given in figure 7, a significant part of the additional workload for young doctors (up to 5 years of experience), employed in hospitals, includes the work with medical and other documentation. The workload on more experienced doctors in hospitals (with 6–20 years of experience) grows due to the need to additionally perform the functions of missing or absent employees and help younger colleagues. Doctors with more than 20 years of experience also note the severity of the workload associated with medical and other documentation and with the necessity to work for others: they are less likely to feel the burden associated directly with the treatment of patients. It can be assumed that different estimates of the volume of a particular workload are caused by differences in professional skills and experience: it is unlikely that young specialists are significantly more loaded with medical work than their older colleagues. They, rather, compensate the lack of experience with more serious efforts. The same seems to go for work with documentation: with experience, the speed of filling in the report documentation increases (although it is impossible to exclude the transfer of some “paper” work to young specialists by more experienced doctors).
Unlike hospitals, in polyclinics, the functions of missing or absent staff are almost equally performed by doctors with a wide variety of work experience (in all groups, one out of four respondents notes that). Most of all, doctors complain about the large amount of work with documentation ( Fig. 8 ).
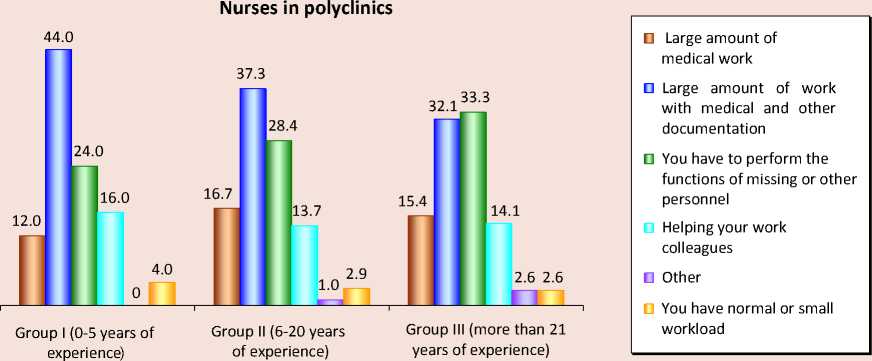
As for nurses who work in hospitals, regardless of the experience, their primary workload is associated with large amounts of medical work ( Fig. 9 ). One out of four or five nurses (depending on their experience) pointed out the workload associated with filling in large volumes of medical and other documentation and performing the functions of missing or absent staff. It is worth noting that among SMPs, young employees are more likely to help their colleagues than more experienced personnel.
Figure 8. Main types of doctors’ workload in polyclinics, %
Doctors in polyclinics
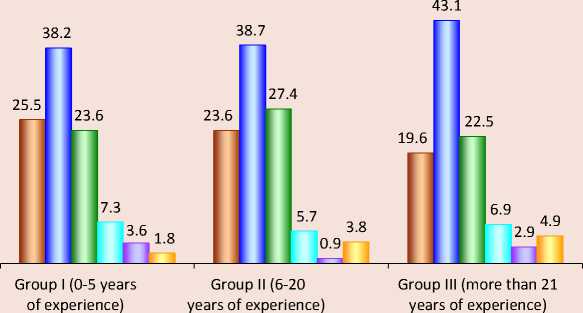
-
□ Large amount of medical work
-
□ Large amount of work with medical and other documentation
-
□ You have to perform the functions of missing or other personnel
-
□ Helping your work colleagues
п Other
-
□ You have normal or small workload
Source: own compilation on the basis of the results of the scientific project “Development of the personnel potential of the capital’s healthcare system”, 2019.
Figure 9. Main types of nurses’ workload in hospitals, %
Nurses in hospitals
-
□ Large amount of medical work
-
□ Large amount of work with medical and other documentation
-
□ You have to perform the functions of missing or other personnel
-
□ Helping your work colleagues
-
п Other
D You have normal or small workload
Source: own compilation on the basis of the results of the scientific project “Development of the personnel potential of the capital’s healthcare system”, 2019.
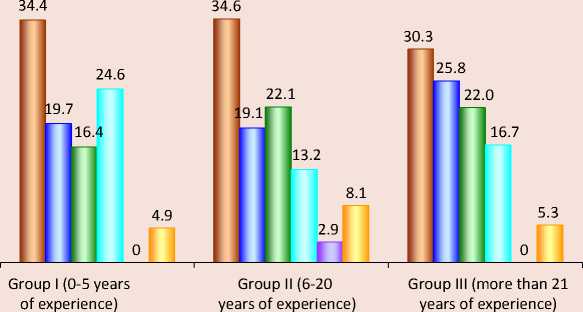
In policlinics, nurses’ primary workload is documentation ( Fig. 10 ). More experienced professionals less feel this type of workload, but with more experience, the workload, associated with performing the duties of missing or absent personnel, increases.
The increase of workload, related to the sharp extension of regulations and reports, was confirmed by surveyed experts: “ Doctors and nurses’ workload is not the same as it was 10 years ago. Not everyone is ready to stand it. Sometimes it forces them to leave for private clinics, where
Figure 10. Main types of nurses’ workload in polyclinics, %
Source: own compilation on the basis of the results of the scientific project “Development of the personnel potential of the capital’s healthcare system”, 2019.
the workload is not as high as in public medical institutions ”; “ Overregulation of work is high. It is impossible to comply with all the regulations at the same time, because it is impossible to remember everything at the moment when it is necessary. A person who constantly treats patients does not have time to go through legal bases: he does not even have an appropriate education for this…”
Overloads increase the risk of a rapid professional burnout. However, experts emphasize that it could be prevented by “ even workload distribution ”. Moreover, as it turns out, material reasons force many healthcare employees to look for opportunities for additional earnings. More than 30% of urban hospitals’ personnel named this reason for justifying their other parttime jobs. According to the results of the survey, doctors working in hospitals are much more likely to work part-time or have other part-time jobs than doctors working in policlinics. Similar trends apply for nurses.
According to diagrams, shown in figure 11, except high personnel’s workload, medical work is hindered by insufficient provision of modern equipment, medications, and materials. Excessive standards of patients’ services and psychological discomfort caused by communications with them are also severe factors. For doctors and nurses in polyclinics, factors that make it difficult to work are excessive standards of patients’ services, problems of communicating with patients, and uncomfortable working environment (tightness, etc.).
In turn, our experts also paid attention to negative influence of the shortage of equipment and materials on labor motivation (“If the equipment is old and you always have problems with consumables and forms, and a chair falls under you every time, then all of this is perceived as “they do not hear me and do not respect me”); communication problems with patients (“ People complain about being asked to wear shoe covers before entering the treatment room or to be quieter. It became a standard that a healthcare employee can be cursed or hit: nobody will be punished for it. It makes many people leave the profession. The risk of being misjudged or called a pest puts pressure on medical personnel: they
Figure 11. Factors which make it difficult for medical staff to perform high-quality work in polyclinics and hospitals, %

Polyclinics
-
□ Working conditions (poor temperature conditions, low light, tightness, etc.)
-
□ Insufficient availability of modern equipment, medications etc.
-
□ Psychological tension among personnel
-
□ Psychological discomfort due to working with patients
-
п Overregulation of work
-
□ Excessive standards of patients' services
-
■ Other
-
□ Nothing is difficult
Source: own compilation on the basis of the results of the scientific project “Development of the personnel potential of the capital’s healthcare system”, 2019.
know that they are right, but public opinion makes them feel unsafe”; “If a person tries to provide great medical assistance, he should be satisfied with the work. It goes beyond salaries: he should feel patients’ gratitude and respect, because he really works in a difficult environment. It is very emotionally challenging to work in a situation, when you are considered an enemy. It greatly affects emotional burnout”.
Psychological assistance should prevent conflicts with patients: “ There should be a balance of negative and positive emotions. Medical personnel should learn how to restore emotional strengths: a doctor is an enemy – he is just tired. This is why psychologists work with medical personnel in other countries. We do not have it ”; “ Even the most professional doctor will leave if he gets beaten by a patient. Medics should be taught to control a situation: it is quite a professional risk, and it is important that they keep such situations from happening themselves ”.
The analysis of the results of the study allows us to point out a number of other tools of a material and non-material nature that allow consolidating the necessary medical personnel and improving the quality of their work:
-
1. Increase of the fixed part of the salary. Statistics show that this component of the remuneration of healthcare workers has changed slightly, and, taking into account inflation, it has not changed much. It is obvious that it is easier for employees to rely on their constant salary than on such a non-permanent component as a bonus. 58.8% of medical personnel, who work in hospitals, noted that the increase of the basic salary is necessary for a comfortable work (more than a third of respondents paid attention to incentive payments), as well as 65.5% of polyclinic employees (incentive payments were noted by a quarter of respondents from this group).
-
2. Payment of incentive allowances, the importance of which was noted by more than a half of the respondents and the experts (“ Salary should be differentiated. If there is a small difference between basic and maximum salary, it will not be a motivating factor ”), should be regulated: everyone have to understand how to get a bonus and what could be done for its increase without damaging primary work.
-
3. The provision of adequate working conditions:
– doctors should treat, and not engage in other activities (to plan purchases of medical equipment, medicines, etc., and, moreover, to search for suppliers and purchases);
– it is necessary to increase the amount of time for patients’ reception – otherwise, the doctor can’t get satisfaction from his own work, let alone the result (this is also indicated by foreign studies [23]);
– adequate planning of medical employees’ working hours – exclusion/limitation of overtime work;
– creation of opportunities for proper rest (in some cases an effective method of preventing professional burnout could be a mandatory sending to an unscheduled vacation in a sanatorium or preventorium);
– planning of an “individual employee professional development map”: since the
moment of employment until retirement, a healthcare employee must have an idea about possible trajectories of professional and career growth, including the terms in which certain career stages could be achieved.
Conclusions
Thus, the study showed that even Moscow’s medical organizations with its diverse capabilities may face a number of personnel shortages and imbalances in the future. Although they are not critical, such forecast makes us look more closely at how the capital’s medical employees feel themselves today. It should be done in order to correct, if possible, the detected problems. The data, obtained in the course of the study, correspond to the conclusions of numerous experts – scientists and practitioners – that, as the result of optimization and achievement of salary indicators corresponding to so-called “May decrees” (2012), the level of medical employees’ workload has significantly increased. Meanwhile, excessive intensity of work, even with an increase of material remuneration, leads to a reduction of physical, intellectual, and psycho-emotional resources of medical personnel, provokes chronic diseases and emotional burnout. This, in turn, affects the quality of medical services and staff turnover, including withdrawal from the profession.
References Problems and prospects of personnel support of the Moscow healthcare system
- The world health report 2006: working together for health. Available at: https://www.who.int/whr/2006/whr06_en.pdf?ua=1
- Global strategy on human resources for health: Workforce 2030. Available at:https://www.who.int/hrh/resources/global_strategy_workforce2030_14_print.pdf?ua=1
- Health at a Glance 2017: OECD Indicators. Available at: https://www.health.gov.il/publicationsfiles/healthataglance2017.pdf
- Organization and financing of public health services in Europe. Ed. by Bernd Rechel, Elke Jakubowski, Martin Mckee, Ellen Nolte. Available at: http://www.euro.who.int/__data/assets/pdf_file/0011/370946/public-healthservices.pdf?ua=1
- Handbook on monitoring and evaluation of human resources for health, with special applications for low- and middleincome countries. Ed. By Mario R. Dal Poz Neeru Gupta Estelle Quain Agnes L.B. Soucat. Available at: https://www.who.int/workforcealliance/knowledge/toolkit/25.pdf?ua=1
- Helderman J.-K. The crisis as catalyst for reframing health care policies in the European Union. Health Economics, Policy and Law. 2015, 10 (1), pp. 45–59.
- Simou E., Koutsogeorgou E. Effects of the economic crisis on health and healthcare in Greece in the literature from 2009 to 2013: A systematic review. Health Policy, 2014, 115 (2–3), pp. 111–119.
- Kyaddondo D, Whyte SR. Working in a decentralized system: a threat to health workers’ respect and survival in Uganda. International Journal of Health Planning and Management, 2003, no. 18(4), pp. 329–342.
- Jewkes R, Abrahams N, Mvo Z. Why do nurses abuse patients? Reflections from South African obstetric services. Social Sciences and Medicine, 1998, no. 47(11), pp. 1781–1795.
- Brewer CS, Zayas LE, Kahn LS, Sienkiewicz MJ. Nursing recruitment and retention in New York State: a qualitative workforce needs assessment. Policy, Politics and Nursing Practice, 2006, no. 7(1), pp. 54–63.
- Richardson G. et al. et al. Economic Evaluation of a Nursing-Led Intermediate Care Unit. International Journal of Technology Assessment in Health Care International Journal of Technology Assessment in Health Care, 2001, no. 17 (3), pp. 442–450.
- Jumpa M, Jan S, Mills A. The role of regulation in influencing income-generating activities among public sector doctors in Peru. Human Resources for Health, 2007.
- Gruen R, Anwar R, Begum T et al. Dual job holding practitioners in Bangladesh: an exploration. Social Science and Medicine, 2002, no. 54(2), pp. 267–279.
- Filc D., Davidovitch N. Rethinking the private-public mix in health care: Analysis of health reforms in Israel during the last three decades. Journal of Health Services Research and Policy, 2016, 21 (4), pp. 249–256.
- Ferrinho P, Van Lerberghe W, Julien MR et al. How and why public sector doctors engage in private practice in Portuguese-speaking African countries. Health Policy and Planning, 1998, no. 13(3), pp. 332–338.
- Bossert Th. Et al. Assessing financing, education, management and policy context for strategic planning of human resources for health. Available at: https://www.who.int/hrh/tools/assessing_financing.pdf
- Human resources for health: Overcoming the Crisis. Available at: https://www.who.int/hrh/documents/JLi_hrh_report.pdf
- Ulumbekova G.E. Zdravookhranenie Rossii. Chto nado delat’. 2-e izd. Moscow: GEOTAR-Media, 2015. 704 p.
- Yarasheva A.V. Research of the personnel potential of the Moscow healthcare system. Moskovskaya meditsina=Moscow Medicine, 2019, no. 3. (In Russian).
- Aleksandrova O.A., Aksenova E.I., Yarasheva A.V., Alikperova N.V., Nenakhova Yu.S. Management personnel in Moscow healthcare: Search for answers to current questions. Problemy sotsialnoi gigieny, zdravookhraneniya, i istorii meditsiny=Problems of Social Hygiene, Public Health and History of Medicine, 2019, no. 5. (In Russian).
- Aleksandrova O.A., Komolova O.A. Formation of the personnel reserve of the heads of the capital’s medical institutions within health care reform. Part 1: Personnel structure of medical institutions’ management and problems of its formation before the health care reform. Trud i sotsial’nye otnosheniya=Labor and Social Relations Journal, 2019, vol. 30, no. 2 (152), pp. 5–18. (In Russian).
- Novikova N.V., Pozdeeva O.G. Prognozirovanie natsional’noi ekonomiki: uchebno-metodicheskoe posobie. Yekaterinburg: Izd-vo Ural. gos. ekon. un-ta, 2007.
- Brooks C. Working with healthcare professionals. In: Walshe K. and Smith, J. (Eds.) Healthcare Management Maidenhead: Open University Press, 2006.
