Schistosomiasis of the female genital organs

Author: Turgunova Dildora Ziyapovna, Khozhimatova Guzal Marifjonovna
Journal: Re-health journal @re-health
Section: Акушерство и гинекология
Article in issue: 3,2 (7), 2020.
Free access
Human schistosomiasis remains an important public health problem in many tropical settings. At least 261 million people require treatment for schistosomiasis and up to 659 million people are at risk. Female genital schistosomiasis (FGS) is a manifestation mainly of Schistosomahaematobium infection. Given the nature of the signs and symptoms of FGS, women tend to approach health services with complaints of infertility or symptoms of sexually transmitted infections. Clinicians are generally unaware of FGS because it is not described in the medical textbooks or nursing curricula in any of the countries where schistosomiasis is endemic. Laboratory diagnostics are inadequate.
Schistosomiasis, fgs, s. haematobium, radical surgery, pathology
Short address: https://sciup.org/14125603
IDR: 14125603 | DOI: 10.24411/2181-0443/2020-10125
Шистосомоз женских половых органов
Шистосомоз человека остается важной проблемой для здоровья во многих тропических регионах. По меньшей мере 261 миллион человек нуждаются в лечении от шистосомоза, и до 659 миллионов человек находятся в группе риска. Шистосомоз женских половых органов (ФГС) в первую очередь является проявлением инфекции Schistosomahaematobium. Учитывая характер признаков и симптомов ФГС, женщины обращаются за медицинской помощью с симптомами бесплодия или заболеваний, передающихся половым путем. Врачи, как правило, не знают о ФГС, потому что в этих медицинских учебниках или программах для медсестер не описывается ни одна страна, где распространеншистосомоз. Лабораторной диагностики недостаточно.
Text of the scientific article Schistosomiasis of the female genital organs
Introduction: Human schistosomiasis (bilharzia) is a parasitic disease prevalent in tropical areas. Although the clinical manifestations on the urinary1 or gastrointestinal2 tracts are widely known, many clinical health-care professionals are unaware of the genital manifestations which are often ignored or underestimated.
Schistosomahaematobium is the main species causing genital manifestations but other species of schistosomiasis have been implicated. The number of people suffering from genital manifestations is not precisely known. The biological plausibility of a causal association between genital schistosomiasis and HIV has been described, and may be an important factor in increasing the risk of contracting HIV in areas or communities where both infections are coendemic.
The clinical manifestations of genital schistosomiasis occur both in women and in men.In men, the symptoms include epididymitis (an inflammation of the eipdidymis at the back of the testicle) which can simulate tuberculosis and associated funiculitis, indolence and possible fistulization, hemospermia, pain during urination prostatitis and others.In women, the symptomatology is unspecific because urogenital schistosomiasis can provoke gynaecological ailments. The most frequently observed signs and symptoms are abdominal and pelvic pain presenting in forms such as dyspareunia, dysmenorrhea, leucorrhoea, menstrual disorders, post-coital bleeding or simple contact bleeding (during an examination), cervicitis, endometritis and salpingitis. The disease evolves most often in a chronic manner. These genital lesions can cause complications such as early abortion, ectopic pregnancy and infertility.The clinical appearance of genital lesions is variable. Traditionally, the only specific lesions in women were considered to be granulomatous lesions the size of a pinhead and visible to the naked eye that look like sand grains. They are rough to the touch and have a sandy consistency (“sandy patches”). Several field studies and researchers have described other lesions such as papilloma , polyps and neovascularizations.Genital schistosomiasis may be associated with the presence of schistosome eggs (ova) in the genitals in both men and women. However, ova are not always concurrently present, and current laboratory methods have a low sensitivity to confirm their presence. Lesions associated with genital schistosomiasis may mimic a host of infections and premalignant or malignant conditions. It is therefore crucial to identify alterations that are pathognomic. Differential diagnosis must be done systematically to screen for cancers (of the vulva, vagina, cervix, endometrium), sexually transmitted infections and urogenital tuberculosis. Clinical diagnosis of female genital schistosomiasis is mainly done by visual inspection and histological methods. The WHO Female Genital Schistosomiasis Pocket Atlas and related Clinical Poster are visual aides that have been developed for clinical health-care professionals to raise the clinical index of suspicion and facilitate identification of these lesions, especially in low-resource settings.
Regular treatment with praziquantel from an early age prevents schistosomiasis from progressing to genital damage and other related complications. In endemic areas, WHO recommends regular large-scale administration of preventive chemotherapy to entire communities or routinely in health facilities.Treatment with praziquantel kills the adult worms and provides relief and regression of inflammatory lesions. Few studies reported that praziquantel has no effect on established grainy lesions. However, elimination of adult worms prevents further egg deposition in the tissues and thus development of new lesions. Early treatment, especially in childhood, is the most effective intervention to prevent the occurrence and development of complications associated with urogenital schistosomiasis. In a rural setting where syndromatic diagnosis is usually done, praziquantel may be added to the syndromic treatment protocol for abnormal discharge. The widespread lack of awareness of genital schistosomiasis leads to misdiagnosis and, therefore, false and ineffective therapy . As female genital schistosomiasis is rarely diagnosed correctly, knowledge about the effect of treatment is also scanty. Incorrect diagnostic of genital schistosomiasis lesions frequently leads to debilitating and irreversible operations such as ovarectomy, salpingotomiy and hysterectomy. It is therefore of utmost importance to sensitize health workers and raise awareness of urogenital schistosomiasis, particularly in endemic countries.The public health advantages of anthelminthic treatment with praziquantel go beyond the simple benefits of curing schistosomiasis and preventing its related genital morbidity. Regardless of the presumptive causal association with HIV infection, urogenital schistosomiasis is a disabling disease by itself, and it should be prevented with the currently available means. The WHO recommended policy of regularly treating school-age children with praziquantel should be reinforced and extended, to involve collaborations with programmes for preventing HIV and other sexually transmitted infections.
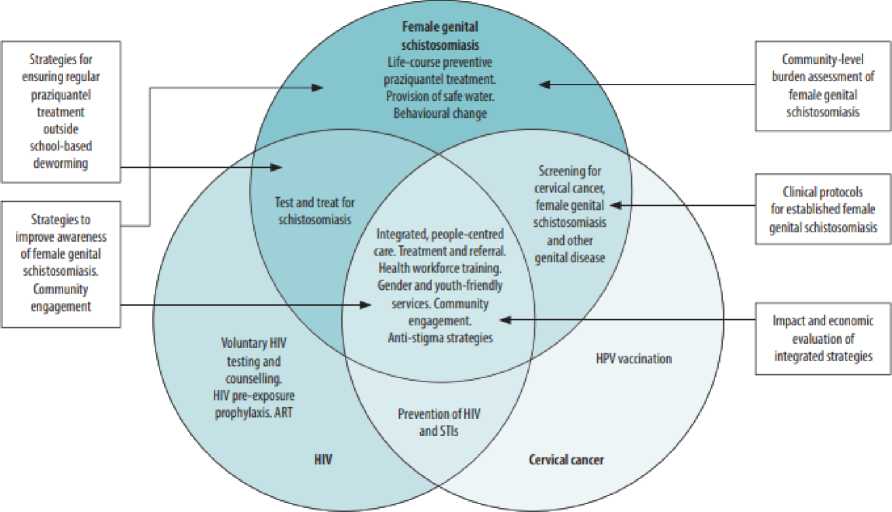
Based on their research on the peoples of Africa, the scientists commented in their scientific article as follows [10]: Operational research to facilitate implementation The operational research needs that were highlighted during the meeting included: (i) community-level burden assessment of female genital schistosomiasis; (ii) strategies for ensuring regular praziquantel treatment of women and girls outside of school-based deworming programmes; (iii) clinical treatment protocols for existing female genital schistosomiasis; (iv) strategies to improve awareness of female genital schistosomiasis and community engagement with the issue; and (v)
impact evaluation and economic analysis of integrated strategies versus separate, parallel approaches. Community-level burden assessment The Bilharzia and HIV study is currently evaluating genital selfswabbing as a potential low-cost approach to community-based diagnosis for female genital schistosomiasis in Zambia. [13] While this approach offers enhanced opportunities for research and impact evaluation studies, it is unlikely to trigger a large-scale investigation of the female genital schistosomiasis burden. We can ask: is such a global or regional burden assessment necessary? At the high-level meeting, [14] voices from experts working in the field confirmed that the public health relevance of the disease is easily revealed by its occurrence in gynaecological practice (Gamba V, University of Nairobi, 2019, personal communication) or qualitative methods in communities (Masong M, Catholic University of Central Africa, 2019, personal communication). Such information can be combined with capacity-building of the health workforce in diagnosing female genital schistosomiasis and the wider use of data platforms in local health services, including health centres equipped to test and treat cervical cancer. If so, the information should provide enough evidence to trigger programmatic integration. Key to the success of such a primary health-care approach is the establishment of a clear case definition of female genital schistosomiasis and the validation of diagnostic algorithms that need to be distributed for use in frontline health services. Strategies for ensuring regular treatment Chronic female genital schistosomiasis lesions can be prevented by regular treatment with praziquantel started at an early age, such as through primary school-based deworming programmes, [15] and continued in later life at all available opportunities. Encouragingly, in addition to praziquantel for school-age children (donated free of charge in sub-Saharan Africa by Merck
KGaA, Darmstadt, Germany), access to the treatment has recently been extended to selected groups of adults. There are also ongoing efforts to make a paediatric formulation widely available to preschool children. Yet, further operational research is needed to optimize opportunities for large-scale treatment of women and girls beyond deworming in school health programmes; for ensuring regular treatment of girls and women with praziquantel through the primary healthcare system; or for test-and-treat approaches during early childhood or from adolescence onwards. An important component of this work includes better ways to diagnose schistosomiasis and female genital schistosomiasis in sexual and reproductive health and rights programmes. The urine dipstick for microscopic haematuria is currently the best proxy for diagnosis of urinary schistosomiasis. However, more sensitive rapid diagnostic tests based on antigen detection in urine are under development and will facilitate test-andtreat approaches in children younger than 5 years, adolescent girls and young women. Combined packages of rapid diagnostic tests and treatment could be tailored for use in health services and programmes. Clinical diagnosis of female genital schistosomiasis would be improved if links could be established with healthcare facilities that provide cervical cancer screening programmes. While the aim of the current paper is to focus on female genital schistosomiasis, these principles are valid too for male genital schistosomiasis. [16] Clinical treatment protocols While its preventive effect is well documented, it is less clear whether praziquantel treatment at the standard dose improves established genital disease. In the Bilharzia and HIV Study in Zambia of women aged 18–31 years, the frequency of six female genital schistosomiasis-related symptoms all declined by 5 to 10 percentage points after a single dose (Bustinduy A, London School of Hygiene and Tropical Medicine,
2019, personal communication). This finding is consistent with the partial resolution of lesions observed in Malawi, [17] South Africa and Zimbabwe after standard praziquantel treatment. However, we need additional research to determine the optimal clinical treatment of female genital schistosomiasis, potentially with higher and more prolonged doses of praziquantel, with or without additional anti-inflammatory drugs. The results will inform the revision of treatment guidelines and curricula in training institutions [18,19].The physical and psychosocial impact of female genital schistosomiasis, along with the potential links across the three priority genital diseases, position female genital schistosomiasis as a pillar in a comprehensive sexual and reproductive health and rights agenda for women and girls in Africa. [20] Despite the many unanswered questions, integrated action with the currently available tools and practices is highly needed and possible. We have summarized a conceptual framework for the integrated programmatic implementation of the three diseases (Fig. 1) . The framework can be further tailored to include screening, treatment or referral for other common female genital diseases or complications of other infections, such as genital tuberculosis. Although female genital schistosomiasis is preventable by regular treatment, too often praziquantel is not available within the primary healthcare system outside of school-based, largescale treatment. [21] Many girls and women who do not attend schools are therefore missed. An integrated response to female genital schistosomiasis, HIV and cervical cancer is likely to boost access to praziquantel treatment for girls and women beyond primary schooling. Established female genital schistosomiasis can be diagnosed during screening for cervical cancer, such as colposcopy and visual inspection of the cervix with acetic acid. The World Health Organization (WHO) has produced a

visual aid to facilitate recognition of health-care professionals [22].
female genital schistosomiasis by clinical
Fig 1.
Conceptual framework for the integrated programmatic implementation of female genital schistosomiasis, HIV and HPV/cervical cancer
Based on the results of their research, this group of scientists came to the following conclusions: Several relevant global initiatives are already in place: the sustainable development goals, including universal health coverage; the 2016 United Nations political declaration on HIV; the HIV prevention 2020 road map46 and the H6 partnership to advance the Every Woman Every Child global strategy. The current global health environment offers opportunities to combine disease-specific initiatives; strengthen health systems at all levels to provide integrated, comprehensive and quality services; and to address the multifaceted and intersecting health, sociocultural, gender and economic issues facing women and girls. Integrated approaches, which have a strong rights-based approach, and which join up multiple public health programmes, create new opportunities and expand existing ways to reach more girls and women throughout their life span. In addition, an integrated approach provides opportunities to mobilize new resources and use existing resources more effectively. Building on lessons learnt from the response to the HIV epidemic, we need to expand and diversify partnerships beyond the traditional biomedical public health communities to engage advocates for sexual and reproductive health rights and women’s rights. Such expanded partnerships will help to position comprehensive prevention and control of female genital schistosomiasis, HIV and cervical cancer within the broader sexual and reproductive health and rights, women’s empowerment and social justice framework.
Diagnosis of acute schistosomiasis, most typically presenting as Katayama syndrome, is most often revealed by clinical observation e.g. urticaria and angio-oedema, as well as, patients’ amnestic recall of signs and symptoms e.g. swimmer itch, dry cough, intermittent fever etc.. Many of these features were thought to result from an over stimulated immune system, from an initial response to immunogenic eggs as first shed into the vasculature by mature female worms. New doubt has been cast on this classic interpretation by the controlled human schistosome infection model. In this carefully manipulated experimentation only male cercariae of S. mansoni were used, thereby precluding any production of egg-antigens specifically, however, Katayama-like syndrome was still described and found correlated with escalating cercarial-dose [23]. Perhaps such hypersensitive, largely Ig-E mediated reactions, are directed towards worm antigens found in worm vomitus as they feed more copiously. Nonetheless, when both the numbers and timings of cercarial dosing are unknown, a precise diagnosis of acute schistosomiasis can be perplexing. Clinical diagnosis is upon a combination of exclusion criteria and detective acumen of rather non-specific, intermittent signs and symptoms, and even if florid, have to tie-in with the individual history and location of cercarial exposure(s). Accurate diagnostic biomarkers of schistosome are needed, ideally that also denote species, worm burden and occurrence of ‘single sexed’ infection. Based on a study of the population of Europe and the United Kingdom, another group of scientists came to the following conclusion [27]: Thus, our diagnostic armamentarium for acute schistosomiasis, notwithstanding those infections caused by S. japonicum or other species within the S. haematobium group, remains incomplete. It is a sobering thought that across Europe and the UK only a few clinical diagnostic laboratories could undertake the methods reported by Cnops et al. [24]. It is also disappointing that the general priority given to schistosome diagnostics is surprisingly low despite its ubiquity and more importantly its potential severity, in terms of male and female genital schistosomiasis [25, 26]. At the very least, the Cnop et al. is a clear signpost for us to do better in our initial clinical triage and subsequent individual disease management plan.
Conclusion : Schistosomiasis is a parasitic disease caused by flukes (trematodes) of the genus Schistosoma. After malaria and intestinal helminthiasis, schistosomiasis is the third most devastating tropical disease in the world, being a major source of morbidity and mortality for developing countries in Africa, South America, Europe, the Caribbean, the Middle East, and Asia. And through this article, the most up-to-date and recent research on schistosomiasis has been discussed. We hope that more in-depth research on the treatment and prevention of this disease will be conducted.
References Schistosomiasis of the female genital organs
- Gilbert B. Schistosomiasis (bilharziasis) of the female genital tract and neighbouring tissues. J ObstetGynaecol Br Emp. 1943;50(5):317-36.
- Charlewood GP, Shippel S, Renton H. Schistosomiasis in gynaecology. J ObstetGynaecol Br Emp. 1949 Jun;56(3):367-85.
- Bland KG, Gelfand M. The effects of schistosomiasis on the cervix uteri in the African female.J ObstetGynaecol Br Commonw. 1970 Dec;77(12):1127-31.
- Gelfand M, Ross MD, Blair DM, Weber MC. Distribution and extent of schistosomiasis in female pelvic organs, with special reference to the genital tract, as determined at autopsy. Am J Trop Med Hyg. 1971 Nov;20(6):846-9.
- Kjetland EF, Poggensee G, Helling-Giese G, Richter J, Sjaastad A, Chitsulo L, et al. Female genital schistosomiasis due to Schistosomahaematobium. Clinical and parasitological findings in women in rural Malawi.Acta Trop. 1996 Dec 30;62(4):239-55. RE-HEALTH JOURNAL №3 ЧАСТЬ 2 83.
