Social and economic damage due to population's mortality from suicides

Author: Morev Mikhail Vladimirovich, Lyubov Evgeny Borisovich
Journal: Economic and Social Changes: Facts, Trends, Forecast @volnc-esc-en
Section: Social development
Article in issue: 6 (18) т.4, 2011.
Free access
The paper presents an analysis of the social and economic burden of suicide death rate in Russia, conducted by research team of ISEDT RAS in research “Social health of the population” in cooperation with the Federal State University “The Moscow Scientific Research Institute of Psychiatry” of the Health Ministry in Russian Federation. The place of suicide in the structure of mortality is defined. It is shown that Russia is a country with the highest suicide rate in Europe. Social and economic costs of suicide in different age and gender groups at the regional and state levels are counted. Its highest level is among men aged 20 to 29 years. The regions with the highest number of lost years of productive life due to suicide are concentrated in the south of Russia (the Volga, Urals and Siberian federal districts). A comparative assessment of suicides burden in the rankings with the common mortality causes from natural and external causes is given. By the level of socio-economic loss suicides far exceed the other causes of the class, “Accidents, injuries and poisoning” and are comparable to the losses caused by coronary heart disease.
Suicide, social and economic damage
Short address: https://sciup.org/147223302
IDR: 147223302 | UDC: 314.174
Text of the scientific article Social and economic damage due to population's mortality from suicides
The demographic situation in Russia throughout last two decades is characterized by a high death rate and poor health quality of the population. The urgency of the problem is caused by the fact, that it takes a stage of “the long stagnation”. In the long term “population estimations have mainly pessimistic character” [13]. Possibilities of maintaining and health strengthening often are a subject of scientific discussions, but only in recent years the scientists began to address to economic aspects of this question. “This is the understanding of that circumstance that the population of the country forms, perhaps, its most important resource, and it is a basis of the future economic growth and scientific and technical development, that is why it requires careful research and from the point of view of economy” [16].
Various aspects of the economic damage from health losses were considered by:
-
1. S.N. Bobylev, V.N. Sidorenko, J.F. Safonov (they studied ecological costs for health of the population connected with water pollution and atmospheric of air).
-
2. D.I. Shmakov, B.B. Prokhorov (they developed a technique for estimation of losses health capital, as a component of the human capital, due to morbidity and mortality of the population in the working age).
-
3. A.A. Afanasev, B.P. Maksimenko (they considered various kinds of energy losses, including the negative influence of the production of electricity energy on human health).
-
4. V.P. Korchagin, V.L. Narozhnaya (they analyzed the population losses because of natural and manmade accidents, failures and natural disasters).
Currently, the negative demographic situation in Russia defines an increased death rate from “external causes” among which the considerable share is occupied with suicides. The increasing attention is paid to suicidal behavior, however basically the researchers address to its demographic or psychological aspects. Meanwhile, the death rate of the population from suicides has also essential social and economic consequences caused by the fact, that suicides widespread among persons of working age. One of such consequences is the high level of a social and economic damage, which estimation is the basis of this research.
The improvement of mental health of the population is noted as one of the fundamental tasks in the World Health Organization program “Health – 21: policy of health achievement for all in the European region of the WHO”.
In particular, it is underlined that “improvement of mental health – especially decrease in number of suicides – requires the most steadfast attention to questions of strengthening and a mental health care throughout the life, in particular, in groups of the population being in disadvantaged economic and social situations” [5].
During the period from 1950 to 1995 the prevalence of suicides has increased in the world on 60%. In the USSR the statistics of suicides was secret, that’s why authentic can consider only the data which were published by the Department of Moral Statistics in 1926 (then the level of suicides was 6.4 on 100 thousand people), and the data for 1965, published during the period of Khrushchev (the level of suicides was 17.1 on 100 thousand people) [2]. Thus for the period from 1965 to 1995 the death rate from suicides increased in Russia on 42% (from 17 to 41 cases per 100 thousand population).
In the European region suicide is now a leading cause of death among young and middle age men. Among causes of death in the age group from 15 till 35 years the suicides take the second place after road and traffic accidents [10]. In the Russian Federation (by data of 2009) in this specified age category suicides were on the first place, being ahead of the number of deaths due to road and traffic inquiries on 10% (13.7 and 12.4 thousand cases accordingly).
It should be noticed that suicide behavior is a wider problem, than population’s mortality from suicides. The perpetrators of parasuicide are associated with it (the attempt of the suicide, which was not ended with the lethal outcome), close relatives of such person, all people having thoughts about suicide.
According to the formula of the WHO experts, at n completed suicides are accounted for 10 – 20 n parasuicides, 8 n close relatives (they enter into a group of the raised suicide risk), 100 n people, thinking of suicide or carrying out destructive actions on subconscious level [3].
Thus, on 37,580 suicides (1.9 of total mortality), officially registered in the Russian Federation in 2009, are accounted, by calculations, 0.4% of inhabitants of the country, who were trying to commit suicide, 0.2% of people from among the nearest environment of the suicident and 2.7% of the persons having “the internal suicide discourse”. In general, the problem of suicide behavior can be turned to 4.7 million persons that makes 3.3% of the population of the country.
According to the World Health Organization, Russia during the last 20 years constantly is among the top five countries having the most high death rate of the population from suicides (in 1990 and 2010 Russia took the 6th place; tab. 1 ).
The trends of suicide activity of the population in 1990th were explained with critical events for the country in 1991 and 1998. Dis- integration of the Soviet Union has made more essential influence on the mental health of the population, than the economic crisis of 1998. This explains the long-term period of growth of suicides level (1991 – 1994 and 1998 – 1999, respectively).
As is noted by the chief specialist of the Federal State Employment Service of the Republic of Karelia, Ph.D. in Economics T.M. Shumilova “economic impact of the crises are leveled much faster than the consequences of personality’s social exclusion” [18].
Despite the positive trend of decrease, observed from the beginning of 2000th, the average death rate from suicides in Russia exceeds the critical value, established by the World Health Organization (20 cases on 100 thousand people; fig. 1 ).
Table 1. Ranging of the countries – the leaders on a death rate from suicides (a number of deaths per 100 thousand people; the sample size – 53 countries) [4]
|
1990 |
1995 |
2000 |
2005 |
2009 |
|
1. Hungary (38.1) |
1. Lithuania (47.9) |
1. Lithuania (46.7) |
1. Lithuania (37.0) |
1. Lithuania (31.5) |
|
2. Finland (29.1) |
2. Russia (41.6) |
2. Russia (37.8) |
2. Russia (29.8) |
2. Kazakhstan (24.5) |
|
3. Slovenia (28.0) |
3. Estonia (40.9) |
3. Belarus (34.2) |
3. Belarus (29.0) |
3. Russia (24.1) |
|
4. Estonia (27.6) |
4. Latvia (40.7) |
4. Kazakhstan (32.7) |
4. Kazakhstan (26.8) |
4. Hungary (21.8) |
|
5. Lithuania (27.2) |
5. Kazakhstan (33.3) |
5. Latvia (30.7) |
5. Hungary (23.2) |
5. Latvia (20.7) |
|
6. Russia (27.0) |
6. Belarus (32.3) |
6. Hungary (29.2) |
6. Latvia (22.5) |
6. Slovenia (18.7) |
Figure 1. A correlation of suicides level in the Russian Federation [9] and the critical value index of suicides according to the WHO (who have died on 100 thousand people) [4]
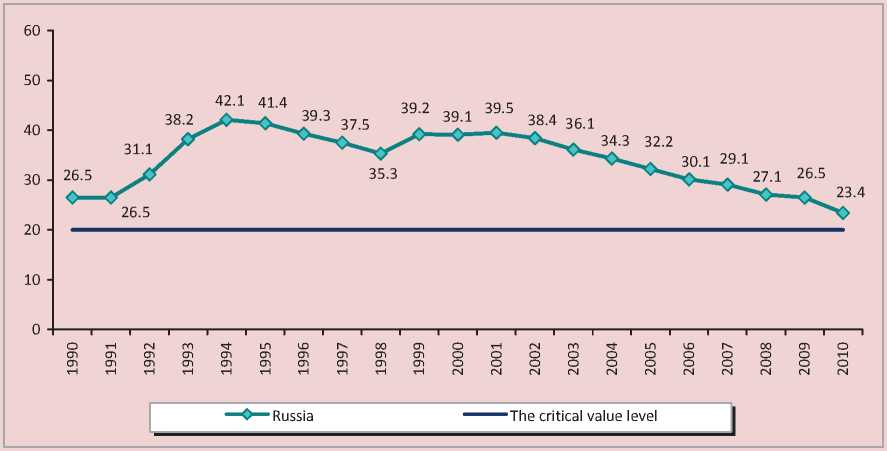
For comparison: in European countries the average number of suicides is 17.5 on 100 thousand people [3].
The external reasons of death rate, which include suicides, took the 3rd place on prevalence in structure of death rate of the population in the Russian Federation. At the same time, within the given class the maximal number of deaths fells on the suicides, despite the downward trend in their numbers during the period from 1990 till 2009 ( tab. 2 ).
Thus, distribution of suicides is an actual problem for the Russian Federation, and not only with demographic, but also from the economic point of view. According to the data for 2009, 50% of suicides were made by the people in the age till 40 years, with this maximum number of suicides were in the age group 25 – 29 years (4231 units). In other words, suicide behavior is widespread among the youngest, working population categories, what causes not only consideration of psychological and demographic aspects of the given problem, but it is also necessary to analyze it as a factor causing an essential economic damage due to early death rate and losses of productive years of life.
For calculation of losses of productive years of life because of suicides we used the World Health Organization YLL indicator (Years of Life Lost, the lost years of life because of premature death rate) [8]. The statistical assumption was made in the case of the absence of the information about the exact age of the person at the time of committed suicide. The person had a medium-average age of 12 years in group from 10 till 14 years, 17 years in group from 15 till 19 years etc.
YLL = N XL, where N – number of deaths;
L – average life expectancy at the age of death (in years). In our case the retirement age was accepted for this indicator (54 full years for women and 60 years for men).
To express in economic terms, each lost year is multiplied on the average GRP of studied year. According to the received data, GRP losses in consequence of LYPL (the lost years of potential life) from suicides considerably exceed the losses from other reasons of a class “Accidents, injuries and poisonings», and also they are compared with losses from the most widespread causes of death (neoplasms and an ischemic heart trouble; tab. 3 ).
Table 2. Changes in structure of death rate of the population in the Russian Federation in 1990 – 2009* [10]
|
Class of the death reasons |
Number of deaths on 100 thousand people |
In % from all reasons of death |
||||
|
1990 |
2000 |
2009 |
1990 |
2000 |
2009 |
|
|
Structure of the general death rate |
||||||
|
All reasons |
1119.1 |
1529 |
1416.78 |
100.0 |
100.0 |
100.0 |
|
illnesses of blood circulation system |
618.7 |
846.1 |
800.98 |
55.3 |
55.3 |
56.5 |
|
neoplasms |
194.4 |
204.7 |
206.89 |
17.4 |
13.4 |
14.6 |
|
the external reasons |
134 |
219 |
158.25 |
12.0 |
14.3 |
11.2 |
|
illnesses of the digestive system |
28.7 |
44.4 |
62.69 |
2.6 |
2.9 |
4.4 |
|
illnesses of the hole damping |
59.4 |
70.2 |
56.00 |
5.3 |
4.6 |
4.0 |
|
some infectious and parasitic illnesses |
12.1 |
24.9 |
24.03 |
1.1 |
1.6 |
1.7 |
|
The reasons of death rate |
Number of deaths on 100 thousand people |
In % from the external reasons |
||||
|
1990 |
2000 |
2009 |
1990 |
2000 |
2009 |
|
|
Structure of death rate from the external reasons of influence |
||||||
|
The external reasons |
134 |
219 |
158.25 |
100.0 |
100.0 |
100.0 |
|
suicides |
26.5 |
39.1 |
26.48 |
19.7 |
17.9 |
16.7 |
|
all kinds of transport accidents |
– |
– |
21.22 |
– |
– |
13.4 |
|
accidental poisonings of alcohol |
10.9 |
25.6 |
15.04 |
8.1 |
11.7 |
9.5 |
|
murders |
14.3 |
28.2 |
15.06 |
10.7 |
12.9 |
9.5 |
|
* Ranked by the value of the index in %. |
||||||
Table 3. Social and economic damage due to LYPL (the lost years of potential life) (2009)
|
Territory |
Ischemic heart trouble |
Neoplasms |
Accidental poisonings of alcohol |
All kinds of transport accidents |
Murder |
Suicides |
||||||
|
Q CD |
Q CD |
Q CD |
Q CD |
Q CD |
Q CD |
|||||||
|
Regions with the highest level of a social and economic damage from suicides |
||||||||||||
|
Republic the Bashkortostan |
26779 |
0.659 |
16905 |
0.416 |
3064 |
0.075 |
15952 |
0.393 |
7657 |
0.189 |
36508 |
0.899 |
|
The Perm Territory |
10693 |
0.395 |
12338 |
0.456 |
6811 |
0.252 |
12623 |
0.467 |
12694 |
0.469 |
23612 |
0.873 |
|
The Chelyabinsk area |
12818 |
0.365 |
15669 |
0.447 |
5246 |
0.150 |
13126 |
0.374 |
10361 |
0.295 |
22712 |
0.647 |
|
The Irkutsk Region |
15765 |
0.630 |
12514 |
0.500 |
4159 |
0.166 |
12949 |
0.517 |
13131 |
0.524 |
22580 |
0.902 |
|
The Sverdlovsk Region |
15704 |
0.357 |
19239 |
0.438 |
6459 |
0.147 |
14025 |
0.319 |
14405 |
0.328 |
22525 |
0.513 |
|
Regions with the least level of a social and economic damage from suicides |
||||||||||||
|
The Republic of Ingushetia |
214 |
0.042 |
1101 |
0.215 |
0 |
0 |
1331 |
0.260 |
2311 |
0.451 |
39 |
0.008 |
|
The Chechen Republic |
2205 |
0.176 |
4497 |
0.359 |
0 |
0 |
3915 |
0.312 |
272 |
0.022 |
42 |
0.003 |
|
The Republic of North Ossetia-Alanija |
4008 |
0.571 |
2253 |
0.321 |
54 |
0.008 |
3341 |
0.476 |
708 |
0.101 |
378 |
0.054 |
|
Karachay-Cherkessia Republic |
1231 |
0.288 |
1519 |
0.356 |
232 |
0.054 |
2876 |
0.673 |
944 |
0.221 |
533 |
0.125 |
|
The Magadan Region |
937 |
0.578 |
813 0 |
0.502 |
401 |
0.247 |
646 |
0.398 |
736 |
0.454 |
651 |
0.402 |
|
Across Russia |
675369 |
0.476 |
640249 |
0.451 |
229896 |
0.162 |
580350 |
0.409 |
350586 |
0.247 |
645061 |
0.455 |
Regional features of formation of a social and economic damage from suicides require the deepest analysis (next stage of researches will be devoted to this question), in the present time we can say that the regions with the highest losses of LYPL from suicides are concentrated in the south of Russia (the Volga, the Urals and the Siberian Federal Districts), that is caused by the raised level of suicides in these areas among representatives of the youngest age groups (till 30 years; fig. 2 ).
The minimum losses of LYPL are marked in the republics of the North Caucasus. In our opinion, it can be connected with influence of the religious factor (Islam strictly forbids a suicide and, thus, rigidly enough supervises private life of a person).
The highest LYPL losses from suicides arise in the earliest age groups (20 – 29 years; as a whole, 37% of all LYPL losses from suicides fell on the given group; tab. 4). The similar situ- ation is observed only concerning transport accidents that can be connected with the raised death rate of children and teenagers from road accident because of non-observance of traffic regulations.
For comparison: the greatest losses from the leading reasons of death rate are in the later age groups (from murders – in group from 25 till 35 years, from alcoholic poisonings – 30 – 39 years, from neoplasms and ischemic heart troubles – 45 – 55 years). It means that suicide trends start to form and prove themselves at early age. Then, if the situation remains not resolved, it can lead to others forms of deviant behavior – aggressions towards others or drug using, which are factors of death rate from murders, alcoholic poisonings, cancer, illnesses of cardiovascular system.
Among youth (by definition of the WHO it is age group from 15 till 24 years) the LYPL size from suicides is 206972 years, that is higher,
Figure 2. Distribution of the regions of the Russian Federation according to the level of LYPL losses from suicides (2009)
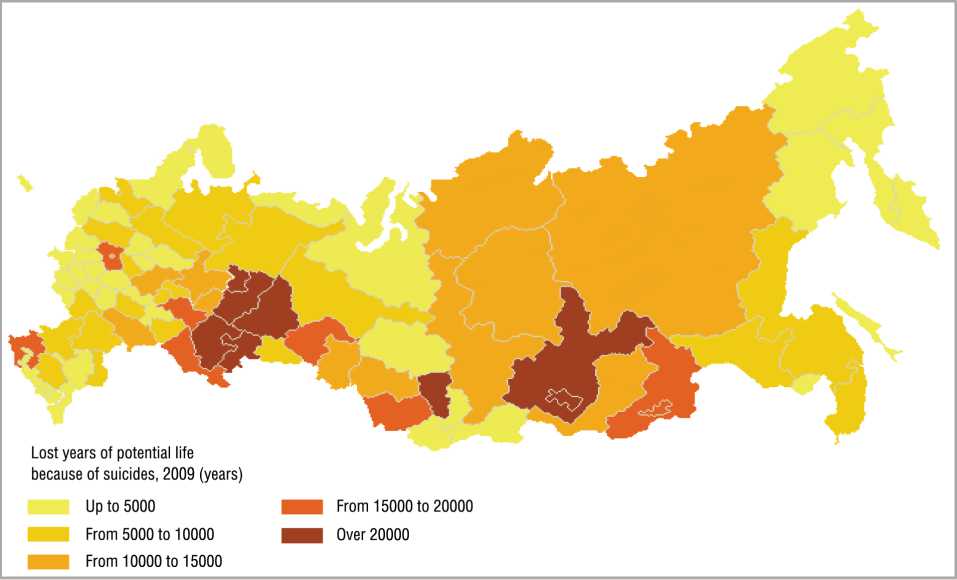
Table 4. Dynamics of LYPL in various age groups of the population in the Russian Federation
For comparison: losses from an ischemic heart trouble account for 2%, from cancer – 15%, from alcoholic poisonings – 7%, from transport accidents – 43%. Thus, suicides, along with road and transport accidents, are those reasons of death rate, which carry the biggest economic damage because of their wide distribution among young people.
Among men, for LYPL losses the suicides concede only ischemic heart troubles, while the death rate from suicides in the given group is about 8 times lower (for the period from 2000 to 2009 it was 56,4 on 100 thousand people, from ischemic illness – 441,5; tab. 5 ). Among female, suicides, despite much smaller prevalence, lead to more essential economic losses, than the other reasons of mortality rate.
Cumulative losses of productive life due to the death rate of the population from suicides across the Russian Federation are 645,1 thou-
Table 5. LYPL and GRP losses among men and women in the territory of the Russian Federation (2009)
|
Cause of death |
Men |
Women |
||||
|
LYPL (in years) |
GRP damage (bill. rub.) |
GRP damage (in %) |
LYPL (in years) |
GRP damage (bill. rub.) |
GRP damage (in %) |
|
|
Ischemic illness |
608686 |
137.568 |
0.429 |
66683 |
15.071 |
0.047 |
|
Neoplasms |
416882 |
94.218 |
0.294 |
223367 |
50.483 |
0.157 |
|
Accidental poisonings of alcohol |
198411 |
44.842 |
0.140 |
31485 |
7.116 |
0.022 |
|
Transport accidents |
468194 |
105.815 |
0.330 |
112156 |
25.348 |
0.079 |
|
Murders |
285510 |
64.527 |
0.201 |
65076 |
14.708 |
0.046 |
|
Suicides |
571575 |
129.180 |
0.403 |
73486 |
16.608 |
0.052 |
Figure 3. Losses of productive life from suicides in territory of the Russian Federation, in years

Men Women
sand years (fig. 3) . From them the share of men is 89%. The reason of such distribution is caused by two factors:
-
1. Firstly, because of the character and type of behavior man traditionally more often, than women, resort to such act, as suicide. This singularity, shown in all age groups, is marked in various researches. For example, men are rarer, than women, address for help to experts in case of psychological problems; in case of suicide attempt select a way with the maximum probability of a lethal outcome (hanging, crossbow).
-
2. Secondly, the high level of losses of productive life due to suicides among the male population is connected with considerable number suicides at a young age (from 10 till 29 years). The share only in this age category is more than half (54%) of all suicides among men.
Suicide behavior among children and teenagers is more often the result of situational-personal reaction (mainly opposition reaction) [16]. Its object are parents, later – teachers and mates. Thus, the high level of suicides among children and teenagers can evidence of negative character of the relationship between these subjects of society.
As a whole, the raised level of suicides among men is marked in many as classical (P. Sorokin, E. Djurkgejm), and modern (D. Vasserman, G.V. Starshenbaum) researches. Scientists agree in opinion, that a primary factor of suicide behavior includes the lack of social integration, psychological feeling of loneliness, mental heartache. That fact is connected with it, for example, that more often suicides are made by men in the age of 45 – 50 years.
At this age they have problems with health, they feel themselves old, against it they cease to feel the support of the spouse, which in this period is as much as possible claimed by children or grandchildren. Except that, men sensitive react to loss of the work, which is the main source of income in the family, to loss of the personal serving, acting as one of the most important social groups for them.
At the territorial level, both among men, and among women, on LYPL losses from suicides the leading positions are occupied by the Volga and the Siberian Federal Districts ( tab. 6 ). It can be explained by the Republic of Bashkortostan, the Republic of Tatarstan, the Perm Territory (the Volga Federal District) and the Krasnoyarsk region, the Irkutsk and the Kemerovo regions (the Siberian Federal District).
It should be noted that GRP loss as a percentage is the most representative and important out of the loss indicators presented in table, because it is relative and does not depend on such characteristics as population size and the absolute value of GRP in rubles.
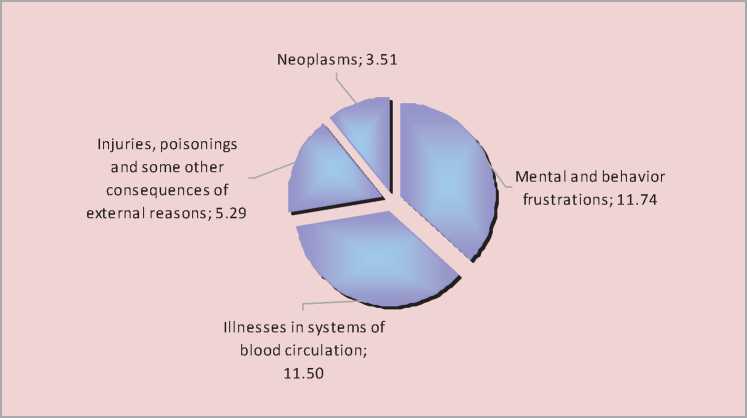
On an example of the Vologda region we have a possibility to compare economic expenses of the healthcare system for treatment of classes of diseases, which correspond to the death rate reasons. Expenses for treatment of illnesses in systems of blood circulation and mental frustrations in 2009 were identical (1.04 and 1.06 billion rub. or 11.5 and 11.7% from the general level of expenses accordingly; fig. 4 ).
At the same time index of LYPL in the Vologda region only on suicides in 2009 was 1532, which is in 13 times higher, than LYPL from an ischemic heart trouble (116 years). It should be noted, that a part of murders, alcoholic poisonings, road and traffic accidents and deaths for unclear reasons is also influenced by a suicide impulse, but for various reasons it isn’t registered as a self-murder.
Thus, the problem of suicide behavior remains very actual in the Russian Federation throughout last 20 years. The high death rate from suicides speaks about insufficient wellbeing of a psychological climate in the country, and also represents the essential social and economic problem, caused by early age of death of the majority of suicidents.
Besides the listed indicators of a social and economic damage, in this work there were not considered the direct costs of healthcare system on the liquidation of negative consequences of parasuicides, and also the indirect costs on the psychological and economic help to the nearest environment of suicident.
However, even in the calculation of losses from officially registered cases of a completed suicide there is obvious an economic benefit, which is possible by realization of the actions, directed on early prevention suicide behavior and decrease of death rate from suicides.
Comprehension by the world community of suicide behavior as the factor, having negative consequences for economy and demo-
Table 6. Territorial distribution of losses LYPL and GRP among men and women (2009)
|
Territory |
Men |
Women |
||||
|
LYPL (in years) |
GRP damage (billion rbl.) |
GRP damage (in %) |
LYPL (in years) |
GRP damage (billion rbl.) |
GRP damage (in %) |
|
|
The Russian Federation |
571575 |
129.180 |
0.403 |
73486 |
16.608 |
0.052 |
|
The Central Federal District |
81448 |
25.113 |
0.219 |
10033 |
3.093 |
0.027 |
|
The Northwest Federal District |
45138 |
11.430 |
0.336 |
7008 |
1.775 |
0.052 |
|
The southern Federal District |
49652 |
7.200 |
0.362 |
6494 |
0.942 |
0.047 |
|
The Volga Federal District |
161155 |
26.312 |
0.535 |
17687 |
2.888 |
0.059 |
|
The Urals Federal District |
63412 |
22.726 |
0.517 |
7666 |
2.747 |
0.062 |
|
The Siberian Federal District |
130878 |
22.692 |
0.669 |
19553 |
3.390 |
0.100 |
|
Far East Federal district |
39892 |
10.705 |
0.618 |
6155 |
1.652 |
0.095 |
Figure 4. Expenses of healthcare system in the Vologda region for treatment of separate classes of diseases (in % from the total costs; 2009)
graphic situation in the country, increases attention to the solution of this problem from the public and authorities. Creation and realization of national strategy for suicide prevention since 1989 are classified by the World Health Organization to a number of priority directions in sphere of public health [15]. Such strategies operate in some European countries (Finland, Estonia, Hungary, Sweden).
In the Russian Federation suicides are one of most often reasons of death rate among the population at working age, however this circumstance isn’t considered in the Concept of long-term social and economic development of the Russian Federation till 2020 by the formation of such strategic direction, as “decrease in death rate of the population, first of all the high death rate of men at working age from external reasons”. Similarly, the mental health aspect isn’t reflected at the realization of the second direction – “the preservation and health strengthening of the population, increasing of a role disease prevention and healthy lifestyle formation” [7].
At the regional level under the modernization health program it is planned to improve forms and methods of the help to the patients with alcoholism, drug addiction, and mental frustration, but the category of suicidents also isn’t selected among priority [12]. Meanwhile, effective steps to the solution of the problem of suicide behavior are possible only in the conditions of the coordinated actions various public and political institutions. This requires the development of special programs (at federal and regional levels), focused on decrease of suicide activity of the population.
Initiatives to establish a system for the prevention of suicidal behavior are fairly common among the subjects of the Russian Federation, but for maximum effectiveness they should be supported at the federal level, what can be achieved through the development and adoption of a single concept of suicide prevention and help to the suicidally inclined.
Similar decisions must be made at the regional level, the following activities should be taken into account in this case:
-
1. Developing a network of crisis and rehabilitation centers, suicidology offices based in hospitals.
-
2. Establishment of statistical information service on the issues related to public mental health and suicidal behavior. Monitoring and development of a data bank on persons exhibiting suicidal tendencies or depression.
-
3. Advanced training of employees in health care and specific areas of activity (social services, children’s homes, penitentiary system, the army, schools, youth organizations, etc.). Development of educational programs of suicidology profile.
-
4. Organization of home poly-professional help to people with mental health problems, based on social assistance centers.
-
5. Development and implementation of a targeted program aimed at promoting a healthy lifestyle among the population and providing the organization of co-operation with the media in covering issues related to suicide, informing the public about the possibilities of overcoming stressful situations, as well as the activities of the specialized services that provide help in case of psychological of problems.
-
6. Stimulation of non-departmental organizations support and protection of human suitsidentov, their families, and individuals exhibiting symptoms of depression.
-
7. Tightening censorship on the Internet, banning sites containing information that may contribute to the development of suicidal tendencies among the population.
-
8. Teaching the basics of Suicidology, methods of adaptation to stressful situations, providing psychological and pedagogical support in crisis situations to school, middle school and high school students within the educational programs (in Life safety, Valeology classes).
Together with the measures aimed at the representatives of the groups of increased suicidal risk it is necessary to implement general social actions (provision of professional employment of the population, constructive realization of leisure among young people, prevention of harmful habits, increasing income level of the most needy population groups).
References Social and economic damage due to population's mortality from suicides
- Bychenko, J.G. Modernization of society and quality of human capital /J.G. Bychenko, L.V. Loginova//News of the Saratov university. -2008. -T. 8. -P. 48.
- Gilinsky, Ya.I. The dynamics of suicides in Russia : an electronic version of the bulletin “Population and Society”/Ya.I. Gilinsky, G.A. Rumyantseva//Demoscope weekly. -№ 161-162. -Available at: http://demoscope.ru/weekly/2004/0161/analit01.php
- Gulin, K.A. Mental health problems of the population /K.A. Gulin, O. Falaleeva, Y.E. Oslopova. -Vologda: Vologda Scientific Coordination Center CEMI RAS, 2003. -71 p.
- Health for all: WHO European Database . -Available at: http://data.euro.who.int/hfadb/shell_ru.html
- Health -21: the politics of health for all in the European region of WHO . -Copenhagen, 1998.
- Kolin, K.K. Human potencial and innovation economy /K.K. Colin//Bulletin of the RANS. -2003. -№ 4. -P. 16-22
- The concept of long-term social and economic development of the Russian Federation till 2020: approved by Governmental Decree from November 17, 2008. -№ 1662-p. -M., 2008.
- A technique for measuring DALY //Official site of the World Health Organization. -Available at: http://www.who.int/healthinfo/global_burden_disease/metrics_daly/en/
- Official site of the Federal State Statistics Service . -Available at: www.gks.ru
- Mental Health: problems and solutions : Report of the WHO European Conference at the ministerial. -Available at: http://whodc.mednet.ru/ru/psihicheskoe-zdorove-i-psihicheskie-rasstroystva/
- Problems of psychological health in Russia : report of physician-psychologist S.V. Boyarintseva at the Round table on the Environment, held in the State Duma March 22, 2010 -Available at: http://3rm.info/publications/2908-problemy-psixologicheskogo-zdorovya-naseleniya.html
- The program for the health modernizing of the Vologda region in 2011 -2012: approved by Resolution of the Regional Government from March 4, 2011. -№ 183. -Vologda, 2011.
- Rimashevskaya, N.M. Russian cross /N.M. Rimashevskaya//The Nature. -1999. -№ 6. -Available at: http://vivovoco.rsl.ru
- Smirnov, V.T. Classification and types of human capital in innovational economy /V.T. Smirnov, I.V. Skoblyakov//Creative industry. -2006. -№ 12. -Available at: http://www.creativeconomy.ru/library/prd165.php
- Social rehabilitation and support for the disabled in Germany : proceedings of Conf., Cologne, January 26 -30, 2010. -Available at: www.dorogavmir.ru/text/Materialy_konferencii.doc
- Psychology of extreme situations : a reader/comp. A.E. Taras, K.V. Selchenok. -Mn.: Harvest, 1999. -480 p.
- Shmakov, D.I. Assessment of economic losses as a result of mortality from accidents, poisonings and injuries /D.I. Shmakov//Proceedings of the Institute of Economic Forecasting RAS. -M.: MAKS-Press, 2003. -Pp. 377-385.
- Shumilova, T.M. Moral principles in modern Russia's labor market/T.M. Shumilova//Supply and demand in the labor market and educational market in the Russian regions: collection of reports on the Second All-Russian Scientific and Practical Internet conference (October 26 -27, 2005). -Book II. -Petrozavodsk: Petrozavodsk State University Publishing House, 2005. -Pp. 192-203.
