Some intense and standardized stomach cancer disease indicators in the Kyrgyz Republic

Author: Toigonbekov Aivar, Akhunbaev Stalbek, Umetov Maksat, Tumanbaev Arstanbek
Journal: Бюллетень науки и практики @bulletennauki
Section: Медицинские науки
Article in issue: 7 т.6, 2020.
Free access
The article addresses issues oncological diseases in Kyrgyzstan. Incidence of gastric cancer in the Kyrgyz Republic is examined and the risks are analyzed. Statistics are given for regions and groups of residents. It is noted that, despite preventive measures, the number of diseases is growing. It is noted that in the Kyrgyz Republic the incidence among men is 2 times higher than among women. Stomach cancer morbidity rate increases with aging. The sickness peak is noted in age groups of 65-69. Supposedly, it is tied up to the etiological factors of risk.
Oncological disease, stomach cancer, cancer patients, incidence
Short address: https://sciup.org/14117785
IDR: 14117785 | UDC: 616.33 | DOI: 10.33619/2414-2948/56/20
Text of the scientific article Some intense and standardized stomach cancer disease indicators in the Kyrgyz Republic
Бюллетень науки и практики / Bulletin of Science and Practice
UDC 616.33
Scope of interest
Stomach cancer (SC), regardless of decrease in the sickness rate, still remains one of the most commonly occurring diseases in the world with about 1 mln new registered cases every year. In most countries men’s predisposition to the SC is 2 times higher in comparison to women’s rate. The morbidity rate fluctuates within broad limits [7; 8]. Thus, according to the most recent data derived from MAIR pub. “Cancer in 5 continents” (vol.7), it’s absolutely obvious that the SC morbidity rate is dependent on diet of population.
The availability in diet of enough vegetables and fruits, animal and vegetal proteins significantly reduces risks of SC.
The example of the USA is most prominent; within last 7 decades of healthy-diet promotion they have reduced the SC rate many times as less. Note, significant reduction of SC risks is found in Japanese emigrants permanently living in the USA, especially those of 2nd or 3rd generation. Russia is among countries with high SC morbidity rate, where new 50 thousand SC cases are registered every year [9].
However, there is a downward trend of SC sickness rate in Russia. Since 1990, the rate of morbidity has decreased for every 10 thousand people (16%) and now makes 48.2 per thousand people. In the oncologic diseases structure among men the SC goes 2nd (11.4%), among women goes 3rd (7.7%), and in the structure of death rate ranks 1st (16.3%) [1].
Due to the data presented above, the problem of epidemiology of the SC, its early diagnosis and prophylaxis have specific relevance. Russia goes 2nd for men and 3rd for women in the group of 45 countries under the level of mortality. Despite morbidity reduction during the last decade the mortality rate on 1st year of disease development is even increased. This is due to the proportion of patients with IV phase and reduction of oncologic aid to the population of Russia. [1; 2]. The highest rate of survival is registered in Japan — 53%, in other countries it’s not higher than 15-20% [5].
The proportion of early detection of SC in Japan is highest as well and is up to a half of all cases, whereas in Europe, the USA and other countries it’s no more than 20 %. Existing facts lead to a hypothesis that Japanese type of SC has distinct differences from SC in Europeans. However, further studies in molecular biology revealed fallacy of this hypothesis, and Japan is successful in survival with SC due to mass screening of the whole population and implementation of national programs of resistance to cancer [9].
Stomach cancer in Kyrgyz Republic goes 3rd in structure of oncologic morbidity and has 11,8% 000. SC is in the 1st place among males – 16,1%000, and 3rd place among females – 7,4%000. According to data on mortality rate, SC in Kyrgyz Republic ranks 1st (10,0%000). Early diagnosis indicators remain low (17,6%); neglect indicators (35,3%) and one-year mortality (81,7%) are high. [6]
Materials and Methodology
We have conducted a research, including analysis of conditions of intense indicators of morbidity in Kyrgyzstan, taking 687 patients with SC in 2017.
All registered SC cases have additional information about general number and gender breakdown of the population of a region in question.
Besides, there is used information about number of adult population in different age-groups (15–19, 20–24, 25–29, 30–34 … 80–84, 85 and >).
This matching is available after collection of data, including information about registration and hospitalization of patients with pancreas cancer. Age-indicators are calculated as a ratio of pancreas cancer cases to corresponding population number multiplied by 100 000. Standardized morbidity indicators are defined by a direct method of morbidity indicators’ standardization with the use of international standardized method.
This method of standard error determination under the direct method of standardization of morbidity indicators is called the method of Poisson. The ratio of 2 age-indicators of morbidity is defined as correlation of ASR 1 to ASR 2 (SRR - standardized rate ratio) and ensures understanding of relative risks of morbidity of one group of population in comparison to another.
Results and Discussions
According to data of NCOH for 2017, the SC is in the first place in the structure of oncologic morbidity in Kyrgyzstan with number of — 10.0 to 100.000 people. Breast cancer (8.5) goes second, followed by cervical cancer (7.2). In comparison to 2001 the SC rate decreased from 13.6 [3] per 100.000 down to 10.0. Perhaps, this is tied to a low rate of early diagnostics and poor organization of registration of new oncologic cases.
Table 1 INCIDENCE OF MALIGNANT TUMORS OF GENERAL LOCALIZATIONS
IN POPULATION FOR 2016-2017 (to 100.000 people)
|
Regions |
Years |
Total |
Esophagus |
Stomach |
Lungs |
Breast |
Cervix |
Rectum |
Prostate |
Skin |
|
Kyrgyz |
2016 |
3585 |
2,6 |
10,9 |
7,4 |
7,1 |
7,2 |
1,8 |
2,4 |
1,0 |
|
Republic |
2017 |
3501 |
2,4 |
10,0 |
6,8 |
8,5 |
7,2 |
1,5 |
1,0 |
1,1 |
|
Chui oblast |
2016 |
777 |
2,5 |
13,3 |
12,0 |
16,3 |
15,2 |
2,5 |
6,5 |
4,4 |
|
2017 |
706 |
2,4 |
11,1 |
11,7 |
10,5 |
12,9 |
3,0 |
2,2 |
2,1 |
|
|
Talas oblast |
2016 |
151 |
3,5 |
15,0 |
7,5 |
4,7 |
9,5 |
0,3 |
0,7 |
0,7 |
|
2017 |
155 |
3,5 |
10,5 |
7,7 |
5,5 |
11,7 |
1,1 |
0,3 |
0,3 |
|
|
Issyk-Kul |
2016 |
323 |
2,5 |
14,7 |
8,2 |
9,6 |
10,0 |
2,3 |
1,4 |
1,2 |
|
oblast |
2017 |
344 |
2,7 |
12,0 |
8,9 |
7,8 |
11,1 |
2,0 |
1,1 |
0,8 |
|
Naryn |
2016 |
238 |
3,2 |
19,6 |
12,5 |
9,4 |
10,1 |
2,5 |
1,4 |
2,5 |
|
oblast |
2017 |
216 |
3,8 |
15,5 |
7,0 |
7,2 |
20,8 |
1,4 |
1,0 |
1,4 |
|
Osh oblast |
2016 |
785 |
5,3 |
12,9 |
7,7 |
4,1 |
5,5 |
1,8 |
0,7 |
0,7 |
|
2017 |
689 |
3,3 |
10,1 |
6,3 |
5,4 |
4,1 |
1,1 |
0,6 |
1,4 |
|
|
Jalal-Abad |
2016 |
488 |
1,9 |
9,1 |
4,8 |
6,0 |
6,0 |
0,7 |
0,5 |
0,6 |
|
oblast |
2017 |
537 |
2,6 |
9,5 |
4,7 |
6,9 |
6,3 |
0,8 |
0,5 |
0,9 |
|
Batken |
2016 |
184 |
2,0 |
6,0 |
3,2 |
3,2 |
6,9 |
0,8 |
- |
1,2 |
|
oblast |
2017 |
162 |
2,1 |
5,5 |
3,5 |
4,0 |
5,2 |
1,1 |
- |
0,7 |
Age group
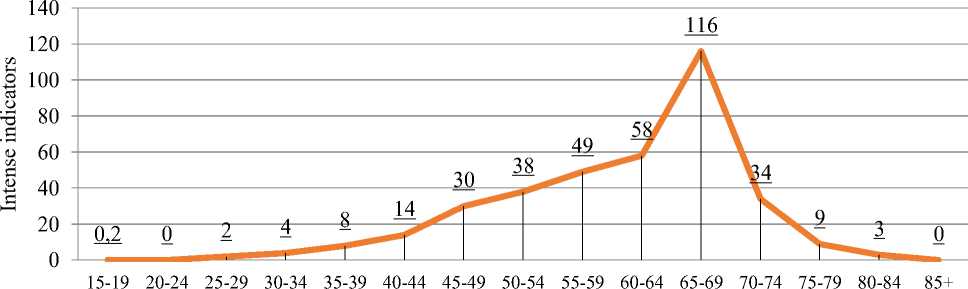
Figure 1. Age morbidity indicators for stomach cancer in 2017.
The Figure 1 shows that the SC morbidity age indicators have highest numbers at the age of 65-69 (116 to 100.000). Another essential fact is the high morbidity rate is detected at ages 55–59 and 60–64 (48,6 – 58 to 100.000 resp.).
Table 2 shows that the standardized age indicator is 16.5 to 100.000 of population, while the standardized international indicator is 13.8 to 100.000.
Table 2
MORBIDITY INDICATORS (BOTH GENDERS) OF STOMACH CANCER STANDARDIZED BY AGE IN THE KYRGYZ REPUBLIC FOR 2017
|
Age index (i) |
Age group |
Number of registered cases (ri) |
Age indicator for adults (ri/ni) |
World’s standard population (wi) |
Standardized indicators for world’s standard population |
|
1 |
0-4 |
0 |
0 |
12000 |
|
|
2 |
5-9 |
0 |
0 |
10000 |
|
|
3 |
10-14 |
0 |
0 |
9000 |
|
|
4 |
15-19 |
1 |
0,200517737 |
9000 |
|
|
5 |
20-24 |
0 |
0 |
8000 |
|
|
6 |
25-29 |
8 |
1,376005559 |
8000 |
|
|
7 |
30-34 |
18 |
3,682201466 |
6000 |
|
|
8 |
35-39 |
29 |
7,551985 |
6000 |
|
|
9 |
40-44 |
46 |
13,56360002 |
6000 |
|
|
10 |
45-49 |
95 |
30,00811799 |
6000 |
|
|
11 |
50-54 |
110 |
37,71747554 |
5000 |
|
|
12 |
55-59 |
126 |
48,60079844 |
4000 |
|
|
13 |
60-64 |
100 |
57,98916762 |
4000 |
|
|
14 |
65-69 |
132 |
116,412382 |
3000 |
|
|
15 |
70-74 |
16 |
34,18949528 |
2000 |
|
|
16 |
75-79 |
5 |
8,665511265 |
1000 |
|
|
17 |
80-84 |
1 |
3,160656152 |
500 |
|
|
18 |
85+ |
0 |
0 |
500 |
|
|
Total: |
687 |
16,47154164 |
100000 |
13,84457349 |
|
Table 3
AGE INDICATORS FOR STOMACH CANCER (MEN) IN KYRGYZSTAN IN 2017
|
Age index (i) |
Age group |
Number of registered cases (ri) |
Number of population (ni) |
Age indicator (ri/ni) |
|
1 |
0-4 |
0 |
400132 |
0 |
|
2 |
5-9 |
0 |
337249 |
0 |
|
3 |
10-14 |
0 |
270624 |
0 |
|
4 |
15-19 |
0 |
253845 |
0 |
|
5 |
20-24 |
1 |
287184 |
0,4 |
|
6 |
25-29 |
0 |
292326 |
0 |
|
7 |
30-34 |
6 |
245586 |
2,4 |
|
8 |
35-39 |
15 |
192495 |
7,8 |
|
9 |
40-44 |
19 |
166054 |
11,4 |
|
10 |
45-49 |
32 |
153212 |
20,9 |
|
11 |
50-54 |
77 |
138110 |
55,8 |
|
12 |
55-59 |
81 |
120612 |
67,2 |
|
13 |
60-64 |
82 |
76677 |
107 |
|
Age index (i) |
Age group |
Number of registered cases (ri) |
Number of population (ni) |
Age indicator (ri/ni) |
|
14 |
65-69 |
59 |
47679 |
123,7 |
|
15 |
70-74 |
73 |
18987 |
384,5 |
|
16 |
75-79 |
12 |
21733 |
55,2 |
|
17 |
80-84 |
4 |
10980 |
36,4 |
|
18 |
85+ |
1 |
9025 |
11,1 |
|
Total: |
462 |
2034505 |
22,7 |
|
|
Table 3 shows that men have relatively high intense indicator of 22.7 to women (Table 4) have intense indicator of 10.5. |
100.000, whereas Table 4 |
|||
|
AGE INDICATORS FOR STOMACH CANCER (WOMEN) IN KYRGYZSTAN IN 2017 |
||||
|
Age index (i) |
Age group |
Number of registered cases Number of (ri) population (ni) |
By-age indicators (ri/ni) |
|
|
1 |
0-4 |
0 |
378270 |
0 |
|
2 |
5-9 |
0 |
322832 |
0 |
|
3 |
10-14 |
0 |
260263 |
0 |
|
4 |
15-19 |
0 |
244864 |
0 |
|
5 |
20-24 |
0 |
276386 |
0 |
|
6 |
25-29 |
0 |
289067 |
0 |
|
7 |
30-34 |
2 |
243252 |
0,8 |
|
8 |
35-39 |
3 |
191510 |
1,6 |
|
9 |
40-44 |
10 |
173089 |
5,8 |
|
10 |
45-49 |
14 |
163369 |
8,6 |
|
11 |
50-54 |
18 |
153532 |
11,7 |
|
12 |
55-59 |
29 |
138643 |
20,9 |
|
13 |
60-64 |
44 |
95769 |
45,9 |
|
14 |
65-69 |
41 |
65711 |
62,4 |
|
15 |
70-74 |
59 |
27811 |
212 |
|
16 |
75-79 |
4 |
35967 |
11,1 |
|
17 |
80-84 |
1 |
20659 |
4,8 |
|
18 |
85+ |
0 |
16696 |
0 |
|
Total: |
225 |
2136325 |
10,5 |
|
Comparing intense indicators, morbidity rate in men is 2 times higher than in women almost in all age groups. (Figure 2).
Stomach cancer morbidity rate in Kyrgyzstan is high and roughly it is 16.5 per 100.000 in 2017, whereas in the international area it is only 13.8 to 100.000. In the Kyrgyz Republic men’s morbidity rate is 2 times higher than women’s — 22.7 and 10.5 per 100.000 resp.
Stomach cancer morbidity rate increases with aging. The sickness peak is noted in age groups of 65-69 (116 to 100.000). However, high morbidity rate is detected in age groups of 55-59 and 6064 as well (48.6 – 58 per 100.000 resp.). Supposedly, it is tied up to etiological factors of risk.
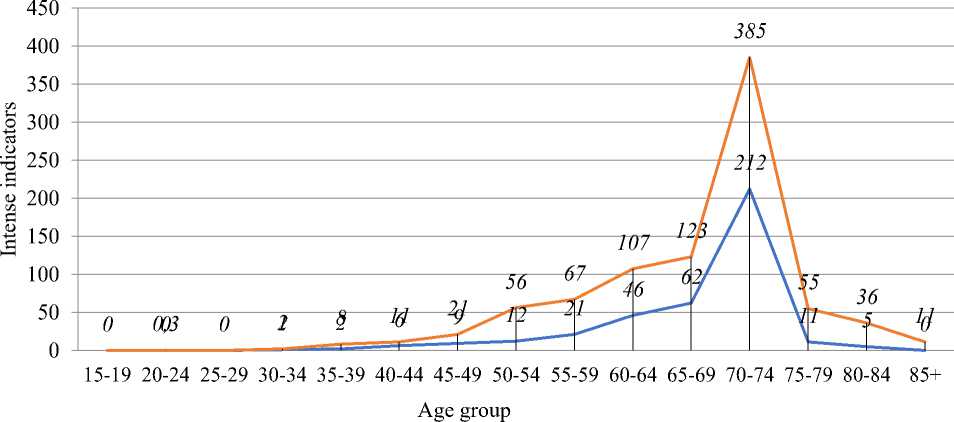
Figure 2. Relative characteristic of SC age morbidity indicators in both genders
References Some intense and standardized stomach cancer disease indicators in the Kyrgyz Republic
- Dolgushin B. I., Virshke E. R., Kosirev V. Y., Trofimov I. A., Kukushkin A. V., Cherkasov V. A.,.. Shishkina N. A. Transcatheter Arterial Chemoembolization with Doxorubicin Loaded Microspheres in Management of Nonresectable Hepatocellular Carcinoma (Long term results) // Int. J. Cancer. 2010. V. 127. №12.
- Давыдов М. И. Тер Ованесов М. Д. Современная стратегия хирургического лечения рака желудка // Современная онкология. 2000. Т. 2. №1. С. 4-12.
- Zaridze D. G. Epidemiology and etiology of malignant tumors // Carcinogenesis. 2000. P. 21-56.
- Бондарев А. В., Ефетов С. В., Олексенко В. В., Черипко О. Н., Джемилев Т. Р., Алиев К. А. Хирургическое лечения раннего рака почки // Таврический медико-биологический вестник. 2010. №16. C. 262-270.
- Самсонов Д. В. Прогностические факторы и результаты хирургического лечения местнораспространенного рака желудка: автореф. дис.. канд. мед. наук. СПб., 2010. 22 с.
- Айдарбекова А. А., Сулайманова А. А., Соодонбеков Э. Т., Миненков Г. О., Тургунбаев У. А. Совершенствование системы оказания специализированной онкологической помощи населению Кыргызской республики // Проблемы Науки. 2017. №17(99). C. 92-96.
- Мерабишвили В. М. Рак желудка: эпидемиология, профилактика, оценка эффективности лечения на популяционном уровне // Практическая онкология. 2001. №3(7). С. 3-8.
- Чиссов В. И., Старинский В. В., Петрова Г. В. (ред.). Состояние онкологической помощи населению России в 2011 году. М., 2012. 240 с.
- Gotoda T., Yanagisawa A., Sasako M., Ono H., Nakanishi Y., Shimoda T., Kato Y. Incidence of lymph node metastasis from early Gastric cancer: estimation with a large number of cases at two large centers // Gastric cancer. 2000. V. 3. №4. P. 219-225. DOI: 10.1007/PL00011720
