Spatial development of social service in the northern region

Author: Dmitrieva Tamara Еvgenevna, Buryan Margarita Stepanovna
Journal: Economic and Social Changes: Facts, Trends, Forecast @volnc-esc-en
Section: Social development
Article in issue: 6 (18) т.4, 2011.
Free access
The article examines the parameters and features of medical and educational service in the northern region, for example in the Komi Republic. The author gives evaluation of the issues relating to functioning of the major elements of territorial framework of social service and determined by low-density, great distances and poor connectivity of space. The spatial development directions are emphasized in the context of development of different medical and educational service centers and reinforcement of net cooperation between them.
Social service, spatial development, territorial framework
Short address: https://sciup.org/147223313
IDR: 147223313 | UDC: 911.3:
Text of the scientific article Spatial development of social service in the northern region
The methodological base of research
Theoretical and methodological outline of problems and strategies of spatial development of social services in the northern region indicate the general and spatial trends of world development which are important from the position of the role, structure and territorial organization of the social services.
The increasing role of services sector
Going to the post-industrial society is an undisputed global vector. Among the most important features of post-industrial society Daniel Bell highlights the central role of theoretical knowledge as a basis for technology innovation, the growth of knowledge carriers’ class (technicians and professionals); the domi- nance of people interaction with one another rather than with the nature and artificial objects in the character of labour; the transition from goods production to service production and the emergence of new services in the field of intellectual and human areas [1].
Service sector is an important element of post-industrial society, because according to Daniel Bell, it is determined by the life quality measured by services and various amenities that are desirable and affordable for everyone. The fundamental things for new life are health and education which is necessary for the growth of technical demands and professional skills. Health care service, education, research and management activities – it is their growth and development which are crucial factors for a post-industrial society.
A peculiar indicator of movement toward a post-industrial society is diversification of the services sector. According to the enlarged sectors typology proposed by A. Fisher in 1934 and specified by K. Clark in 1940, the construction and service industries (trade, finance, transportation, public health services, entertainment) as well as science, education and management were attributed to the tertiary sector of economy. When improving the category of the tertiary sector, D. Bell mentioned P. Hatta’s and N. Foote’s contributions, who in 1953 identified the “quaternary” and “quinary” sectors, they linked the changes in the employment structure with characteristics of social mobility and emphasized critical value of “quinary”, or intellectual, sector [1].
In the Hutt-Foote-Bell’s scheme the tertiary sector proper includes transportation and communal services, the quaternary sector includes trade, financial services, insurance and real estate activities, and the quinary sector includes health care system, education, research, entertainment and public administration.
A widespread classification (Browning and Sinqelmann, 1975) divides services into distribution ones (transport, communications, trade), productive ones (finance, insurance, business services), social ones (health, social security, education and science, postal service, management), public ones (personal services, hotels and restaurants, entertainment, repair) [2]. Based on this classification, we combine the first and the second groups as an industrial service and the third and the fourth groups – as a social service.
For the post-industrial transformation of the region economy, as it was shown by A.N. Pilya-sov, the main role is played by the intellectual part of the social services segment and the scientific and technical part of business services segment (consulting, technical service, etc.) [3].
Basic service sector contribution into the life quality determines its environment-forming role. The post-industrial transformation is impossible without the formation of local and external flow of human capital, without relying on the creative class, sensitive to life activity conditions. Creating a highly organized environment that meets the high-tech ideas of comfort and service is especially important in the northern regions to stop the outflow and fixation of population.
The post-industrial society is a service economy with increased demand for services, attention to a human being, to comfortable environment, to the possibility and necessity of lifelong education of population.
The report on the 2009 world development 2009 “A new view of economic geography” prepared by the World Bank Group says that the development for the benefit of whole population with objectively unequal economic growth provides the alignment of consumption (living standards) and the distribution of benefits from the concentration of production [4].
This thesis, on the one hand, reflects recognition of the uneven economic development related to the objective conditions of forming the profit due to the proximity to resources, the effect of agglomeration and the concentration of other market factors.
On the other hand, it emphasizes the priority of the criterion of social justice of the economic development - wherever people live, they should be equal in their capabilities and life quality.
The alignment of consumption (living standards) is implemented largely by increasing the power and the uniformity of generation and transfer of public services by the service sector that is possible due to the flow of funds from the effective concentrated production.
Space development and spatial development
It is possible to distribute the benefits of concentrated growth and alignment of goods and services consumption in the space by economic integration - economically pulling the lagging areas to the leading ones. The economic integration is carried out through market mechanisms of agglomeration, migration and specialization with special attention to the land, labour and goods markets. The tools for promoting economic integration include the following measures of public policies:
о geographically neutral — institutions (the legal standards for the use of land, labour force, social services);
о geographically binding — infrastructure (policies and investments in the construction of roads, ports, communication systems);
о geographically targeted — incentives (social programs, tax remissions and preferences) [4].
An example of active integration is the European policy of “uniting the territory”, its motto is “turning territorial diversity into strength” [5]. Its content specifies the transition from the regional economic development policy (aimed at compensation of the regions for their adverse conditions) to the policy projecting regional growth and competitiveness and aimed at controlling their factors.
The terms of development and application of economic integration tools and at the same time the indicators of its transformative effect on the economy and the economic geography of the territory define three dimensions of space development: density, distance, and isolation named by the socio-economic development factors in the World Bank report.
Challenges of low-density, long distances, high disconnection of space impeding the progress of economic and social development are opposed to such principles of the territorial cohesion policy as the concentration of economic activity, connectivity, interaction [6, 7]. The targeted implementation of these principles makes it possible to change qualitatively the space of functioning of different processes of life activity and to improve their performance.
In contrast to the space development that characterizes the “relief” in which the process takes place, the spatial development is the concept “adjusted” to control. Generalizing the definition by P. Shchedrovitskii and V. Gla-zychev given to the country [8], we define the spatial development as identifying a real spatial framework of development of objects, including the advance growth nodes and the links between them, planning the areas of advance development of these nodes and links.
The “carcass” approach to the spatial development in the post-industrial terminology can be interpreted as a “network” approach, which reveals the morphology of the flow space, which M. Castells contrasts the site space historically rooted [9]. The material form of the flow space is composed of three layers:
-
• the first layer consists of communication network, technology infrastructure, fundamental spatial configuration;
-
• the second layer consists of nodes, where the strategically important functions are performed in the area, and communications centers that coordinate the interaction of elements in the network;
-
• the third layer relates to the spatial organization of dominant managerial elites performed the managerial functions, with an organized space being built around them.
Detection and parameterization of these layers, inclusion of areas (hinterland) in a network of centers, interaction intensity (distances in the network) depending on the location of the points – all these positions, unconditionally, are productive and require an empirical study in the context of the spatial development of social service.
Functional-and-territorial organization of social service of the Komi Republic
Among all elements of the social services we consider the medical and educational services determined the conditions of people’s life and their development to a large extent.
The system of medioprophilactic institutions of the republic includes the levels of primary outpatient and polyclinic aid in the urban and rural areas and specialized care profiled by groups of diseases (cancer, mental health, tuberculosis, drug abuse, etc.), as well as specialized high technology medical aid.
Primary health care is provided by independent health care agencies and outpatient and polyclinic units which are the parts of medical institutions. In the rural areas they are outpatient clinics (general practitioner’s department), medical and obstetric posts (MOPSs), nursing homes, emergency medical stations (offices).
Specialized in-patient and out-patient and polyclinic medical services are provided by specialized clinics and city hospitals in the cities and by the oblast and district hospitals in the rural areas. Highly skilled and high-tech medical care is provided by five health care institutions situated in Syktyvkar.
Designed to provide every citizen with the possibility to obtain basic knowledge, to pass professional retraining or to get new specialty, the education system includes pre-school, school elementary, primary, secondary and higher vocational education. In the republic the school network is represented by primary, elementary and secondary public, municipal and private schools, some of which as the resource and support education centers serve the educational and methodical functions. Practically all stationary and branch institutions of primary and secondary vocational education are located in the urban areas. The centers of concentration of stationary higher education institutions are the cities of Syktyvkar, Vorkuta and Ukhta.
Taking into account both the nature determined by completeness (species diversity) and the services area (geography and number of receivers), we’ll interpret the above mentioned functional-and-status types as territorial-hierarchical ones fixing the basic types of service centers in the medical and educational network of the republic.
Settlement service centers provide primary health care and educational services. There are MOPSs, outpatient clinics, local hospitals, primary, elementary and secondary schools that serve people living in rural and urban communities of municipalities, as well as administrative-territorial entities of city districts.
Base service centers situated usually in the capitals of municipal districts and city districts or their “second” centers (the points distinguished in the municipality by its production capacity), in the oblast hospitals (OH) provide wider range of medical services, particularly in the urban hospitals. The profiled agencies (blood transfusion stations, neuropsychiatric institutions, tuberculosis clinics) provide specialized medical services as well. In the base centers along with the secondary schools there are support schools equipped with up-to-date hardware and staffed with highly qualified teaching staff. These centers are characterized by the service of primary and secondary vocational education.
Complex service centers is notable for the most complete set of services, first of all, the specialized ones, which are characterized in the segment of health care by uniqueness for this region, technology, highly qualified staff. These services are provided by Cardiology Clinic, Cancer Clinic, Perinatal Center, and Eye Microsurgery Center.
The complex centers include resource centers of general education retransmitting the experience of introducing profile education, using health saving technology, etc., as well as institutions of higher vocational education. At the present time the complex social service centers are the cities of Syktyvkar, Ukhta, Vorkuta.
The problems of spatial development of social service
The function of the region social sector is to ensure timely and equitable access to the maximum complete (within a specific region) set of services. The integrated accessibility criterion includes not only the service availability, but also its quality and cost. This means both physical and economic accessibility.
The present level of logistical and personnel of state, network availability don’t meet enough full generation and transfer of medical and educational services. The analysis based on the parameters of activity density; distances affecting the transport accessibility of services; isolation / disconnection of the services space, will make it possible to identify the peculiarities and to formulate the problems of social service. The main positions of density, distance and disconnection influence on hierarchical space of medical and educational services are represented in table 1 in general.
As the table shows, the large and almost insuperable distances in the Komi Republic, as well as in any other northern region are critical factor of development space.
We have identified differentiation of the Komi Republic territory by the level of internal (from the settlements to the settlement center) and external (from the settlements centers to the centers of metropolitan districts) transport accessibility on the basis of a specially developed method [10]. The interpretation of its results for the analysis of the space of development of social service has helped to clarify the groups of administrative territories of the base service centers and to choose the pilot ones among them.
By the ratio of territories with different types of transport accessibility we have sorted out 6 territories with the most adverse connection conditions among the 20 municipalities of the republic. At the same time we took into account the share of dispersed territories (the settlements with great distances to the settlement centers) and territories distant from the municipal center.
Table 1. The peculiarities of medical and educational services space
|
Space development parameters |
Specifics of the network (spatial framework) of social service Description of distribution of service centers |
||
|
Primary |
Base |
Complex |
|
|
Service density |
Distribution of the centers with MOPSs and schools generally corresponds to a system of population settlement and satisfies the requirements for the services availability |
Distribution of the centers with the OH and secondary schools generally satisfies the needs The local imbalances in the services of primary and secondary vocational education |
Distribution of the centers with specialized medical services doesn’t meet modern requirements. The imbalance by the structure of higher vocational education specialties |
|
Distances – transport accessibility of services |
Low availability of service centers in the outlying villages, districts, areas and in their groups because of the remoteness of the settlements, unsatisfactory roads and river crossings, unstable bus service |
||
|
Isolation – unequal access to qualitative services |
Essential differentiation of physical and economic services accessibility because of differences in logistic condition of MOPSs, hospitals, schools, staff, in the transport cost to get the centers with necessary services |
||
The disadvantaged areas are peripheral Izhma, Ust-Tsilma, Troitzko-Pechorsk, Ust-Kulom, Udora and Priluzsky areas. To compare the characteristics from the group of favourable municipalities we have taken Ust-Vym and Koygorod areas as a conditional reference group.
The problem of providing services of the primary network of social service is not so much a lack of centers, but in their unsatisfactory condition reducing the quality of medical care and general education.
On the whole, distribution of MOPSs, outpatient clinics (OC), local hospitals (LH), and schools are in line with the population settlement system, and it is close to the consumer. Their density is non-uniform and depends on the population number, the compactness / dispersion of distribution of the localities, the state of transport links and availability of seasonal or year-round connection. The features of configuration of rural dispersion in the northern region reflect the influence of natural and economic factors. Mostly a linear character of the arrangement of localities in the underdeveloped areas is related to valley dispersion, and in the developed areas – to route dispersion. The southern areas where dispersed forest and agricultural activities developed geographically and historically have greater density and, hence, smaller distances in the dispersion system, but small population number in the settlements.
In distribution of the health care objects we can emphasize the areas of high density of primary network of health care agencies marked by intense quality background at the schematic map (fig. 1) . At the same time the types of distribution of primary centers are different and reflect the character of settlement, the pilot areas can demonstrate it.
The valley type is characteristic of the lower areas of the Pechora (Ust-Tsilma and Izhma areas) with the river system of dispersion and poor transport network. Taking into account a relatively great number and rarity of localities in each of the settlements in these areas, there are from three to six medical institutions serving from 100 to 700 people. In half of the settlements medical care is available in all localities, and in other settlements - almost in all (except one or seldom two small villages).
The route-valley distribution of primary service centers are typical of the areas located in the upper reaches of the rivers – the Pechora (Troitsk-Pechorsk), the Vychegda (Ust-Kulom), the Mezen (Udora) – and having one or two district roads. As in the lower areas of the Pechora, there the health care agencies are situated in three or four settlements. Big and small villages without medical facilities are close enough to MOPSs and outpatient clinics except for two or three localities per a district, their population is restricted when obtaining primary medical aid.
The peculiarities of the Priluzsky area, the southernmost district of the republic, are dense small settlement dispersion and as a transport axis – federal highway “Vyatka”. Here the route type of distribution of the primary health care centers providing the services to the population of more than one locality prevails. The population of the two localities is restricted in the first medical aid because of the barriers and the distance.
The network of first-aid services being adequate form the dispersion point of view, their quality is restrained by worn-out and obsolete material and technical basis. On the whole, all over the republic more than half of medical institutions buildings are wooden. In some areas from 60 to 80% of the wooden buildings MOPs have a 100% depreciation. 54% of fixed assets have over 50% depreciation, and in the outlying districts these figures are 100% and 70% respectively.
The distribution of school network depends on the demographic structure of population and the transport accessibility of settlements with schools. The students living far from schools, can get to the schools by special buses. The primary schools are as close as possible to the places of residence.
Figure 1. Distribution of the health care agencies of the Komi Republic

In the areas with the river system of dispersion the secondary schools are located in all settlements (one in four or five localities), with one secondary school and one-two elementary schools in settlement. The number of settlements without schools is two or four per a settlement.
In the areas with mixed valley-route type of distribution of the first-aid services there is one secondary school per two or four, more rarely five or six localities, there are settlements only with the primary school (one school per two or three settlements), the number of settlements without schools reaches 3-5 per a settlement.
In the areas dominated by the route distribution of the primary first-aid centers per one secondary school there are on the average three or seven, sometimes ten or more settlements, but with the primary or secondary school in the settlement. Many localities have no schools.
The main problems of giving the general education services – the lack of teaching staff and its aging, the poor material and technical basis – are especially acute in rural outlying schools, where low level of services and utilities, high wear of wooden buildings, there are no teachers of Foreign Languages and Computer Science, the teachers of retirement age work there.
The declining demographic situation (decline in the birth rates, aging of populations in towns and villages, their depopulation), the outflow of population from the northern regions and from the rural areas to the urban ones claimed optimization of school network. Over the past 10 years the number of schools has decreased significantly and the number of towns and villages without schools has increased. The republic has acquired the experience in searching for deliberate and non-conflict decisions when combining the set of conditions – finding schools in the place of children’s residence, acceptable (no more than an hour and without risk of boat crossing) distances for conveying, ensuring the required level of education (teaching all subjects, proper equipment). In this case it is clear that taking into account the social role of rural school, it is important to preserve the existing network, technically updating the old schools or building the new small modernly equipped and comfortable schools, using the new technology. These solutions are relevant not only for hard-to-reach localities, but also economically and demographically stable localities.
The main problem of the basic level of social service network is low availability of centers, which applies mainly to medical service. In the basic centers there is a lack of primary and secondary vocational education institutions training the skilled workers for the industries of the republic’s specialization - logging, timber, oil-and-gas producing industries – which solves this problem by shift workers from other regions.
The limitations of transport accessibility of district hospitals because of their long distances, the barriers to movement by the reason of unsatisfactory state of roads and river crossings, rare and unstable bus-communication cause discrimination of the part of population in obtaining timely and skilled medical care, profiled by diseases.
To evaluate the accessibility of basic service centers we have grouped the settlements of outlying districts and compared them with conditionally reference districts. The thresholds of group intervals differentiation were chosen with the period of aid for cardiovascular diseases taken in the Komi Republic – 40 minutes (or 30 km of local roads). The localities up to 30 km from the district center were the short-distance group, more than 30 km – the long-distance group. Regardless of the distance the “barrier” groups are the localities situated beyond the water barrier, which is often overcome by the bridge requiring the repair or (and) the unstable boat, ferry or seasonal ice crossing.
The evaluation results have showed the following features of accessible services of central hospitals located in the municipalities with low internal connection (fig. 2) :
-
• the share of population living outside of standard time for medical care is varied from 50 to 80% and is greater than the corresponding value in the conditionally reference area;
-
• the population concentration in the district center (51% in the Troitzko-Pechorsk district and 30% in the Ust-Tsilma and Priluzsk districts) increases the proportion of the population living in the nearby settlements;
-
• the increased proportion of the population form the barrier localities in the Ust-Tsilma and Izhma districts is associated with predominance of the valley type of dispersion;
-
• the southern Priluzsky district has two principles of dispersion: “state farm – some villages” and “many small villages”; and it is reflected in high specific weight of hard-to-reach localities, which is proportional to the total number of localities in the district.
Figure 2. Transport availability of basic service centers in weakly connected areas of the Komi Republic
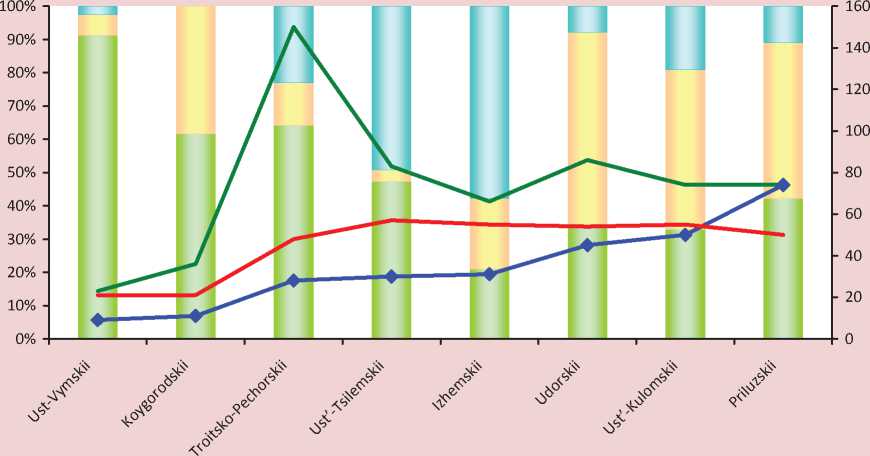
■ ■ Population of short-distance localities Population of long-distance localities
■ __ ■ Population of barrier localities ♦ Number of hard-to-reach localities
^^^Average distance to the district center, km Weighted average distance to the district center, km
The average distance from the locality to the district center characterizes the physical distance of accessible medical services. The peak of the Troitsko-Pechorsk district curve reflects the inaccessibility of Mitrofan-Dikost settlements, people living there have to go 350 km through two municipalities to get to their central hospital due to the lack of year-round communication. The average weighted distance gives an idea of the real load on the lines of communication, taking into account the territory population. We should note that the factors of population density and population employment were taken into account in the detailed assessment of transport accessibility of 2616 communes (municipalities) of Belgium as resistance to communication [11].
A high proportion of people discriminated by the conditions for obtaining timely medical services, suggests the need for reducing critical situation with transportation access by reducing the barrier by force of bridge construction, for ensuring smooth operation of river crossings, for road construction improving the internal connection in Troitzko-Pechorsk, Udora and Ust-Kulom districts.
The problem of specialized services at this stage is connected with their almost total concentration in Syktyvkar. Syktyvkar eccentricity causing 200-1000 km remoteness of the district centers from the capital and the lack of railway exits in many municipalities make it very difficult to obtain and increase the cost of proper services. Unfortunately, many localities of the republic did not even have a two-hour accessibility to the railway station that is adverse according to the European standards. In American researchers’ calculations, the fee for medical services due to poor transport activity increases by 30 times with increasing distance by four times [12]. Unfortunately, the examples of such progression of reducing the economic services availability are currently feasible for many people in the Komi Republic.
The directions of the spatial development of social service
In accordance with the claimed content the purpose of the spatial development of social services is to build a framework of the sector to improve service of the republic population, increasing the quality and accessibility of medical and education services throughout the territory.
As noted above, the challenges of “low density”, “large distances” and “strong disconnection”, distorting the object development space can be answered by economic activity concentration, connection and co-operation or networking. The concretization of these principles in planning the areas of the development of centers and communications of medical and education services segment of social service in the Komi Republic are generally presented in table 2 .
The proposed areas can be implemented by the activities outlined in strategic documents of the republic modernization of the health system and education [13, 14, 15].
Compaction of the service center network
The primary medical centers are strengthened by replacing the old MOPs and reconstructing the outpatient clinics and local hospitals. Over the past four years more than 20
modular MOPs serving from 400 to 600 people have appeared in many municipal areas. The objects of primary (closest) medical aid are repaired and are planned to be repaired, first of all, in the localities situated in the outlying districts with hard-to-reach settlements – Troitzko-Pechorsk, Udora, Izhma, Ust-Kulom, Ust-Tsilma districts etc. Networking the general medical practice and complex districts covered by a therapist will help to strengthen the primary medical services.
New elements in the framework of medical service will be inter-district centers: rural and urban diagnostic and medical ones (fig. 3) .
The diagnostic centers are organized on the bases of several rural central hospitals and are equipped with mobile complexes for early diagnosis and selection of risk groups of socially significant diseases (cardiovascular disease, respiratory disease, diabetes, glaucoma, breast cancer). The work of mobile diagnostic complexes will be implemented mainly in remote and hard-to-reach localities. The rural diagnostic centers (Sysolskii, Ust-Kulomskii, Ust-Vymskii, Izhemskii), the activities of which will have more than 33% of the republic population, will strengthen substantially the basic centers in these districts and raise the level of medical aid in all municipal districts.
Table 2. Strengthening of the spatial framework of social service
|
Spatial development principles |
Areas of service center development and co-operation |
||
|
Primary |
Basic |
Complex |
|
|
Concentration – quantitative and qualitative compaction |
Reconstructing, constructing, technical and staff renewal of MOPs, outpatient clinics, local hospitals, schools Optimization of primary network for dispersion and people’s interests |
Reconstructing, up-to-date equipment, staff for central hospitals Making addition to primary and secondary vocational education with training the specialists for TPC and FEC* in the centers of proper districts |
Organizing new centers and kinds of specialized medical services Training highly skilled specialists for the needs of the region |
|
Connection – Improving the transport service accessibility |
Reducing physical and economic (transport expenses) distances due to improving the transport infrastructure (roads, bridges, crossings, bus service and local air communication), appearing some new centers, using the mobile diagnostic complexes |
||
|
Co-operation and networking – access to qualitative sevices |
Reducing the disconnection of service space and equalizing the consumer opportunities all over the territory by delivering the service to the consumer (making TV medicine and distance education as well as health and education internet systems), expending the range and capacity of free high-tech services |
||
|
*TPC – timber processing complex, FEC – fuel-energy complex. |
|||
Figure 3. Complex medical service centers
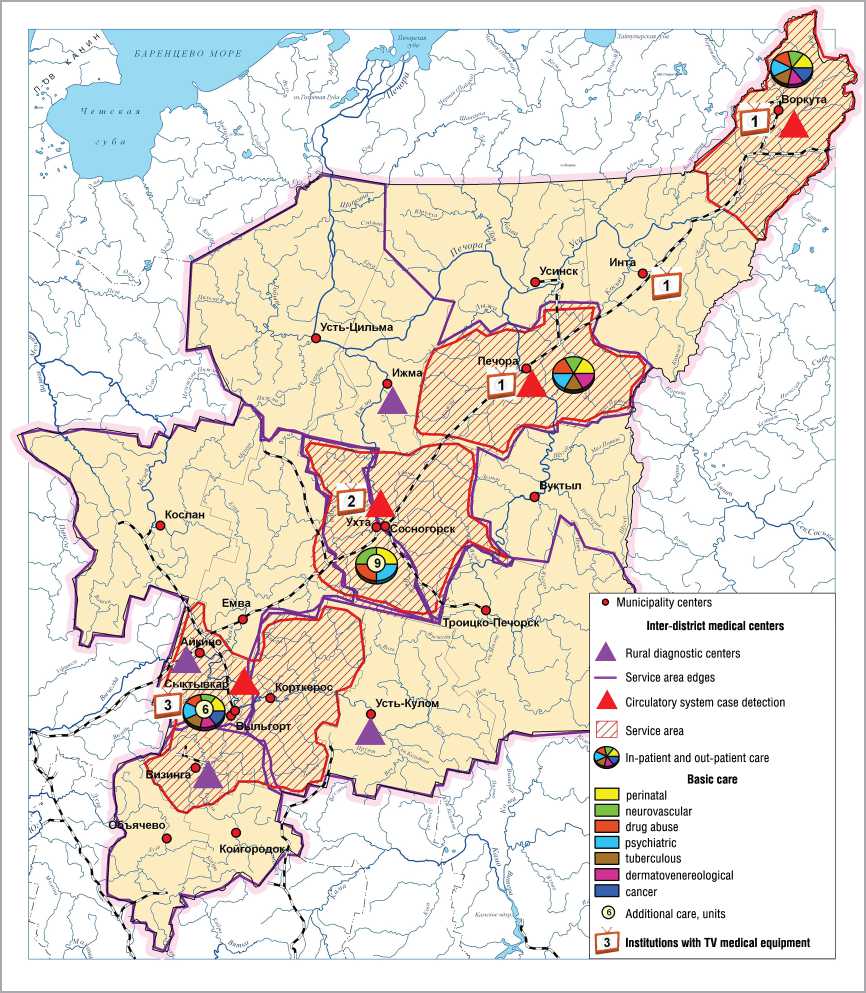
For early detection of circulatory system cases there is organized a vascular center in Syktyvkar and primary vascular departments in the cities of Vorkuta, Pechora, and Ukhta, having its own service area and routes of timely (within 40 minutes) convey of patients with insulin and heart attack and covering two thirds of the population.
Inter-district health care centers located in Syktyvkar, Ukhta, Pechora, and Vorkuta will provide inpatient and outpatient help in many basic and additional directions. The most diversified services in hospitals, as well as adult and child outpatient care are offered by Syktyvkar and Ukhta centers.
Thus, the combination of new medical facilities concentrated in the largest cities of the republic will strengthen Syktyvkar center and will create new centers of integrated health services. Their uniform distribution over the transport and economic axis will set the territorial imbalances of metropolitan centralization right and will improve the accessibility of the population to specialized high-quality medical care significantly.
Improved transport access to the services
In 2010 36% of the rural settlements of the republic did not have paved roads to reach the means of public communication. At the same time almost a third of them is located near the railway station or landing pier.
To improve transport connectivity of the territory the strategies are defined as follows: 1) keeping the existing public communication network, bringing its condition to the level corresponding with the standards and bridging over the rivers; 2) providing reliable transport links in a number of directions from municipal centers to the centers of settlements and some certain settlements by building new sections of roads and bridges [16].
Within the scope of the first task the improvement of transport connectivity can be achieved by:
о keeping a little intense exploitation of railway lines Sosnogorsk – Troitzko-Pechorsk, Mikun – Koslan – Vendinga;
о improving the quality of highway network, overhauling the bridges over medium and small rivers, bridging over the rivers;
о establishing a regular bus service between the support settlements and the municipal centers, constructing the approaches to the settlements;
о improving the state and the quality characteristics of the waterway of the Pechora and the Vychegda river basins and ensuring the stable operation of socially important passenger shipments;
о further developing intra- and interregional air transport.
Sustainable transport links between the settlements with municipal centers and the settlement centers will contribute to the reconstruction of existing road sections and construction of new ones.
Not only internal but also external accessibility of peripheral areas will be improved by reconstructing and constructing the highway sections in the areas Ukhta (Sosnogorsk) – Troitsko-Pechorsk – Komsomolsk – Yaksha – further to Solikamsk, Perm, and Pechora – Vuktyl – Troitsko-Pechorsk – Ust-Kulom – Koygorodok – federal highway “Vyatka”, which will become new transport corridors of the republic.
When the road construction Syktyvkar – Ukhta – Pechora – Usinsk – Naryan-Mar and Aikino – Koslan is finished, more than 200 thousand people in five municipalities will receive access to the support public highway network.
Co-operation and networking
The development of service sector and the growth of comfortable environment in the rural hard-to-reach settlements requires a change of the principle of services delivery. The current situation where the rural consumer has to obtain the necessary health care or education services far from home and at a high price, that is “delivery of the consumer to the service” should be changed by mobile “delivery of the service to the consumer” on the basis of TV medicine, distance learning and other forms of service, taking into account the service specific.
The project on the development of TV medicine technologies that make it possible to connect the complex and basic service centers has been implemented in the republic since 2007. Now the appropriate equipment is available in Cardio-logical Clinic, the Komi Republican Perinatal Centre, the Komi Republican Hospital (Syktyvkar), the city hospital and city clinics (Ukhta); city emergency hospital (Vorkuta); city hospital (Inta), central district hospital (Pechora).
The control and coordination are performed by the Republican medical information and analytical center (see fig. 3).
This system, which saves the cost of air medical service and patients’ finance, is used by prenatal diagnostics of congenital malformations; advice on keeping pregnant and patients with cardiac pathology; emergency consultations to provide skilled care to the patients who are in critical condition; prehospital counseling to specify the provisional diagnosis, treatment and hospitalization; remote training of specialists.
For schools in remote settlements the distance learning is perspective. Using Internet technologies makes it possible to give the best teacher to every school and every home. Such form of learning requires a special individual educational programs and new organizational forms of support from the federal and regional education centers, which can arrange insession part-time and full-time education of gifted children in specific areas.
A new form of education has been launched in the republic since 2010 on the basis of the Distance Education Centre for the disabled children in all municipal centers that are connected to fiber optic communications. Within the pilot project the distance education has gone to small schools in the settlements of Irael (Sosnogorsk district) and Yb (Syktyvdinsk district).
The infrastructure of new connection becomes crucial factor in promoting new cooperation technologies and e-connectivity in the network of social service. First of all, it is the completion of commutation to the fiber optic link of all centers of the municipalities followed by adjoining peripheral settlements, which will provide broadband access and significantly improve the quality of communication with all basic and many primary centers providing medical and education services.
In conclusion we fix the following main points of the spatial analysis of social service.
When equalizing the living standards to achieve social justice with objectively unequal economic development, social service and, above all, health and education and services play a leading part.
Provision of services depends on the level of service development and on the availability of services for the population, which is determined by the ratio of such parameters of development activity space as density, distance and connectivity (or disconnection).
In the Komi Republic, a typical northern region, timely access to quality services provided by different centers of a hierarchical network is difficult because of:
-
✓ insufficient material and technical condition of the primary service centers, the nearest ones to the consumer;
-
✓ low transport and economic affordability of basic centers with profiled health care and it restrains more than half of municipal residents living in remote locations in obtaining the services;
-
✓ remoteness of the most population from the specialized high-tech medical services because of their concentration in the capital.
Taking into account the revealed problems, the content of spatial development of social service of the republic should be:
О compaction of the network (framework) by updating the primary medical and general education instaurations and forming new medical centers of specialized services of diagnosis and treatment;
О growth of connectivity and cooperation of the space of medical and education services reducing the time of their provision and expanding the reach of high quality services by improving transport infrastructure as well as the active introduction of electronic forms of services delivery – TV medicine and distance learning.
References Spatial development of social service in the northern region
- Bell, D. The coming post-industrial society. Experience in social forecasting/D. Bell. -M.: Academia, 1999. -956 p.
- The handbook of Service Industries/ed. by John R. Bryson and Peter W. Daniels. London: Edvard Elgar. 2007. -504 p.
- Pilyasov, A.N. And the last will be the first: the northern periphery towards the economy of knowledge/A.N. Pilyasov. -M.: Knizhny dom “LIBROKOM”, 2009. -544 p.
- A new view at the economic geography. Report on the world development for 2009/World Bank. -Washington, 2009.
- Green Paper on Territorial Cohesion, the way ahead//en Inforegio panorama. -2008. -№ 28. -December.
- Growing Regions, growing Europe -Fourth report on economic and social cohesion/European Commission, Luxembourg: Office for Official Publications of the European Communities, 2007. -222 p.
- Investing in Europe’s future -Fifth report on economic and social cohesion/European Commission, Luxembourg: Publications Office of the European Union. -2010. -298 p.
- Russia: spatial development. Report of 2004. -M.: Architectura-C, 2004. -128 p.
- Castles, M. The Information age: economy, society and culture/M. Cartels. -M.: GU-VSh, 2000. -608 p.
- Dmitrieva, T.E. Transport availability of local systems/T.E. Dmitrieva//Atlas of the Republic of Komi. -M.: Feoria, 2011. -Pp. 280-282.
- Vandenbulke, G. Mapping accessibility in Belgium: a tool for land-use and transport planning/G. Vandenbulke, T. Sneerberger, I. Thomas//J. Transport Geography. -2009. -Vol. 17. -№1. -Pp. 39-53.
- Bugromenko, V.N. The modern geography of transport and transport accessibility/V.N. Bugromenko//Proceedings of the RAS (Geographical Series). -2010. -№ 4. -Pp. 7-16.
- The program for modernizing the health care system of the Komi Republic for 2011 -2012 . -Available at: http://minzdrav.rkomi.ru
- State report on the health status of the Komi Republic in 2010 . -Available at: http://minzdrav.rkomi.ru
- The concept of preschool, general and additional education of the Komi Republic for 2011 -2015: project . -Available at: http://www.komiedu.ru/legislation/info
- The main directions of the development of transport system in the Republic of Komi up to 2020: project . -Available at: http://minprom.rkomi.ru
