Technical points of Ilizarov external mini-fixator for the treatment of phalanx fractures

Author: Tian Lin, Chen Weiwei, Qu Long
Journal: Гений ортопедии @geniy-ortopedii
Section: Оригинальные статьи
Article in issue: 3 т.27, 2021.
Free access
The Ilizarov external mini-fixator (IEMF) has become an effective tool for the treatment of acute and chronic hand and foot injuries and deformity correction due to its advantages of easy fixation, good holding power, and artful appearance. However, there are relatively few clinical reports on this technique. Materials and methods From June 2019 to March 2021, we preformed IEMF on 113 patients with open phalanx fractures as emergency surgery, and all patients had 3-6 months follow-up. Results All fractures achieved clinical healing. Among them, pin site infection occurred in 8 fractures (7.07 %), arthrolysis occurred after 6 fractures (5.3 %), and 4° rotation malunion occurred in 3 cases (2.65 %).
Hand, foot, phalanges, fractures, ilizarov mini-fixator, complications
Short address: https://sciup.org/142229725
IDR: 142229725 | UDC: [617.578+617.588]-001.5-089.227.84-08-06 | DOI: 10.18019/1028-4427-2021-27-3-322-324
Технические особенности внешнего мини-фиксатора Илизарова для лечения переломов фаланг
Внешний мини-фиксатор Илизарова (ВМФИ) является эффективным инструментом для лечения острых травм кистей и стоп и их последствий и коррекции деформаций благодаря легкости фиксации, хорошей удерживающей способности и привлекательному внешнему виду. Тем не менее, имеется относительно немного клинических отчетов о применении этой техники. Материалы и методы. С июня 2019 по март 2021 года ВМФИ применен у 113 пациентов с открытыми переломами фаланг в качестве неотложной операции. Все пациенты находились под наблюдением в течение 3-6 месяцев. Результаты. Во всех случаях достигнуто сращение переломов. Из осложнений отмечена инфекция места расположения штифта в 8 случаях (7,07 %), артролиз развился после 4 переломов (5,3 %), неправильное сращение с разворотом фрагментов на 4° произошло в 3 случаях (2,65 %).
Text of the scientific article Technical points of Ilizarov external mini-fixator for the treatment of phalanx fractures
In the 80-s of the 20th century, Ilizarov creatively invented the Ilizarov external mini-fixator (IEMF) for hand diseases [1]. It has fully considered hand’s unique anatomic and functional features, and has gradually been favored by hand surgeons due to its small size, flexible operation, and good holding power. Until now, there are relatively few clinical reports of IEMF [2–8], thus, it still requires more clinical practice and open discussions by surgeons for further optimization.
IEMF technique was first introduced to China by Dr. Long Qu in 2014, and the devices were supplied by Changzhou Holy Medtech Co., Ltd (No. 20190217, Su Chang Machinery Equipment, China) in 2018. Chongqing Greatwall Hospital introduced the IEMF devices in June 2019, and has treated 113 open phalanx fractures so far (March 2021). Among them, 53 were oblique fractures, 25 were wedge-shaped fractures, and 35 were comminuted fractures. After applying IEMF, finger function exercises were carried out according to patients’ recovery condition. All patients were followed up for 3–6 months, and all fractures achieved clinical healing. Among them, pin-site infection occurred in 8 fractures (7.07 %), which was stopped with oral antibiotics and wire cleaning; arthrolysis occurred in 4 fractures (5.3 %), which were improved by functional rehabilitation; and rotation malunion of 4° occurred in 3 cases (2.65 %).
1. Key Technical Points
Based on the clinical practice of IEMF technique in the treatment of phalangeal fractures, we summarize the key technical points as follows:
(1) Entry angle of the wire : the angle between the wire and the surface of the cortical bone should be close to or equal to 90°, and pierce the wire “parallel” or 45° to the palm plane. Every wire needs to penetrate the cortex to
expose a length less than 1.0–1.5 mm. Besides, the same set of fixed wires should be parallel to each other.
-
(2) Entry position of the wire : when inserting the wire, “tendons and ligaments” need to be protected. It can be tested by passively moving the affected finger. If the wire has passed through the ligament, resistance will be felt during the movement.
-
(3) Fixation method : the height of the fixator above the skin is determined by the bending angle of the wire. The smaller the angle, the closer the fixation unit is to the skin. The proper distance between the bottom of the external fixator and the skin is 1–1.5 cm. The central axis of the fixator needs to be parallel to the central axis of the bone.
-
(4) Bending method : the wire can be bent by two methods, namely “C” type (gradually bend 90 degrees) and “L” type (one-moment bend 90 degrees), as shown in Figure 1.
-
(5) Tension principles : the principle of uniform stress distribution should be followed to avoid stress concentration in order to increase the stability of the external fixators.
-
(6) Number of wires : according to the type of fractures, 3–5 wires can be applied on each side of the fixator.
-
2. Treatment of three common types of fractures
For oblique fractures, the wire should be inserted parallel or 45° to the palm plane, and the bending angle and the external fixator should be adjusted to be consistent with the central force line. For comminuted or wedge-shaped fractures, fracture reduction should be applied first, and then the fracture fragments should be fixed with wires to simplify the fracture structure. The fixed wire is bent and fixed to the external fixator, which not only supports the reduction, but also helps to stabilize the fracture. The fixation methods of different types of fractures are shown in Figure 2.
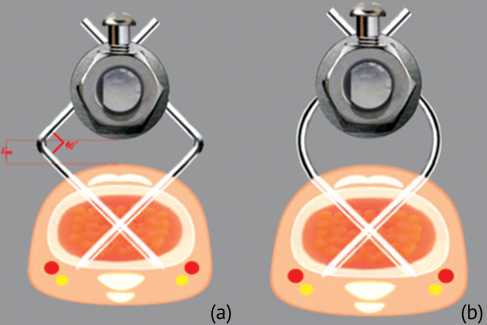
Fig. 1. Bending methods of wires: a – “L” type (acutely bend 90 degrees) bending method; b – “C” type (gradually bend 90 degrees) bending method
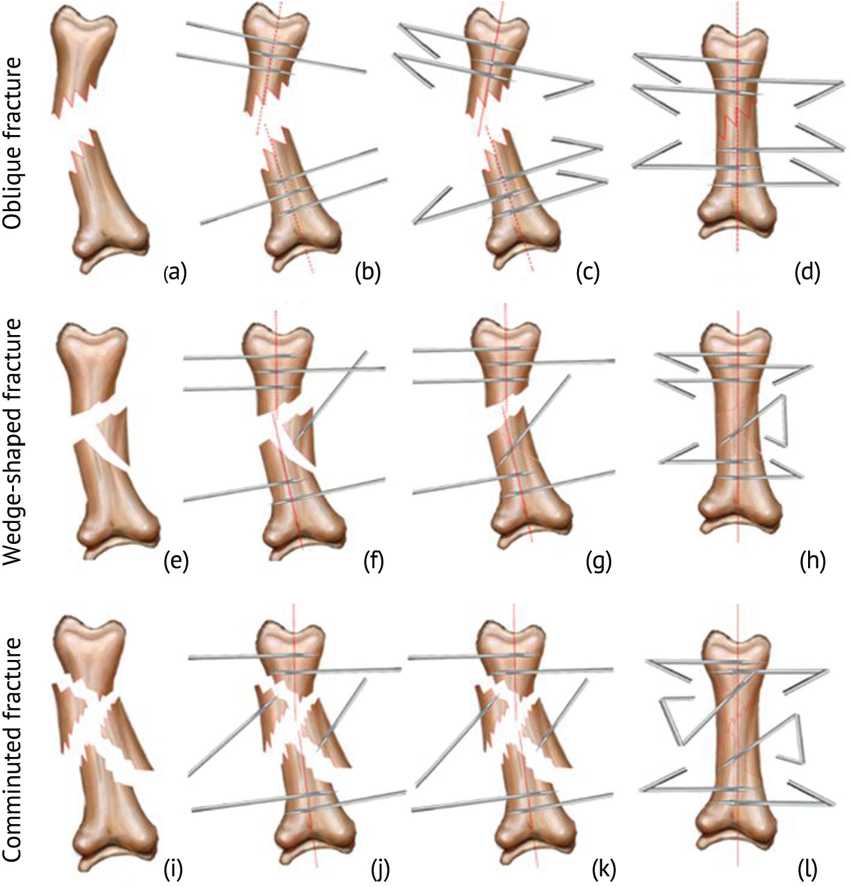
Fig. 2. Schemes of fixation methods of three common types of fractures: a–d – fixation methods for oblique fractures; e–h – fixation methods for wedge-shaped fractures; i–l – fixation methods for comminuted fractures
References Technical points of Ilizarov external mini-fixator for the treatment of phalanx fractures
- IIlizarov G.A. Transosseous Osteosynthesis. Theoretical and Clinical Aspects of the Regeneration and Growth of Tissue / ed. by S.A. Green. Berlin (Heidelberg): Springer-Verlag, 1992. DOI: 10.1007/978-3-642-84388-4
- Danilkin M.Y. Phalangeal Lengthening Techniques for Brachydactily and Posttraumatic Digital Stumps With the Use of a Modified External Mini-Fixator // Tech. Hand Up Extrem. Surg. 2016. Vol. 20, No. 2. P. 61-66. DOI: 10.1097/BTH.0000000000000116
- The effectiveness of distraction lengthening in traumatic hand amputation with Ilizarov mini fixator / T. Kanchanathepsak, H. Gotani, Y. Hamada, Y. Tanaka, K. Sasaki, H. Yagi, Y. Kubota, T. Tawonsawatruk // Injury. 2020. Vol. 51, No. 12. P. 2966-2969. DOI: 10.1016/j.injury.2020.02.080
- Minimally invasive corrective osteotomy with the Ilizarov mini-fixator for malunited fractures of the phalanges: a technical note / Y. Tomori, M. Nanno, S. Kentrao, T. Majima // J. Nippon Med. Sch. 2020. DOI: 10.1272/jnms.JNMS.2021_88-314
- Kataoka T., Kodera N., Takai S. The Ilizarov Mini-External Fixator for the Treatment of First Metatarsal Fracture: A Case Report // J. Nippon Med. Sch. 2017. Vol. 84, No. 3. P. 144-147. DOI: 10.1272/jnms.84.144
- Correction of Severe Contracture of Intrinsic Plus Hand with a Modified Ilizarov Mini-Fixator: Correction with an Ilizarov Mini-Fixator for Severe Hand Contracture / Y. Hamada, K. Sairyo, N. Hibino, A. Kobayashi // J. Hand Microsurg. 2015. Vol. 7, No. 1. P. 161-165. DOI: 10.1007/s12593-014-0134-6
- Zolotov A.S. Open Infected Seymour Fracture // J Hand Surg. Asian Pac. Vol. 2019. Vol. 24, No. 4. P. 488-490. DOI: 10.1142/S2424835519720196
- Clinical efficacy of Ilizarov external mini-fixation in the treatment of open comminuted phalangeal fractures / T. Lin, Y Tan, F. Li // Chinese Journal of Hand Surgery. 2020. Vol. 36, No. 5. P. 330-332.
