The effectiveness of postoperative rehabilitation protocol following pectoralis major tendon repair

Author: Lychagin A.V., Gritsyuk A.A., Zhidilyaev A.V., Garkavi A.V., Lipina M.M.
Journal: Кафедра травматологии и ортопедии @jkto
Article in issue: 4 (42), 2020.
Free access
Abstact Background.In recent years the occurrence rate of pectoralis major tendon injury has grown which is explained by an increasing interest in, and promotion of, a healthy lifestyle and a growing popularity of gyms, but early surgical treatment, even nowadays, not administrated in every case, especially with correct rehabilitation protocol.The aim of the study was to assess the effectiveness of postoperative rehabilitation protocol following PMT repair Materials and methods.The study includes the results of treatment of 33 patients, average age was 28.5±4.0 years. Treatment results were assessed in groups with surgical and conservative treatment at 6 and 12 months. In both groups, the outcomes were assessed using the basic DASH scoring questionnaire (Disabilities of the Arm, Shoulder, and Hand - a scoring scale designed to assess the degree of incapacitation of the upper extremity) and its supplement that focuses on sportsrelated functions Results. After 6 months postoperative rehabilitation in Group 1, the average score according to the basic DASH questionnaire and its sports-focused supplement was 4.38±2.42 and 5.58±3.58, respectively; the same indices for Group 2 were 15.00±3.00 and 27.50±5.50, respectively. Following 12 months, we observed a deterioration of the results attained in both groups. In Group1, the average score was 6.31±2.43 for basic DASH questionnaire, and 7.37±4.72 for supplementary DASH questionnaire; in Group 2 20.43±3.82 and 41.25±9.50, for both DASH scores, respectively. In Group 2 treatment results were reliably worse both 6 months and 12 months after the injury. Conclusion. Surgical treatment exceeds conservative treatment in efficiency, even in case od old ruptures
Musculus pectoralis major, tendon ruptures, surgical treatment
Short address: https://sciup.org/142229608
IDR: 142229608 | UDC: 617.3 | DOI: 10.17238/issn2226-2016.2020.3.43-48
Эффективность протокола послеоперационной реабилитации после восстановления сухожилия большой грудной мышцы
Введение.В последние годы увеличилась частота повреждений сухожилия большой грудной мышцы, что объясняется растущим интересом и пропагандой здорового образа жизни и растущей популярностью тренажерных залов, но раннее хирургическое лечение, даже в настоящее время, проводится не во всех случаях. особенно при правильном протоколе реабилитацииЦелью исследования было оценить эффективность протокола послеоперационной реабилитации после восстановления сухожилия большой грудной мышцы.Материалы и методы. В исследование включены результаты лечения 33 пациентов, средний возраст которых составил 28,5 ± 4,0 года. Результаты лечения оценивали в группах с хирургическим и консервативным лечением через 6 и 12 месяцев. В обеих группах результаты оценивались с помощью базового опросника DASH (инвалидность руки, плеча и кисти - шкала оценки, предназначенная для оценки степени нетрудоспособности верхней конечности) и дополнения к нему, в котором основное внимание уделяется спортивным функциям.Результаты. Через 6 месяцев послеоперационной реабилитации в группе 1 средний балл по базовому опроснику DASH и его спортивному дополнению составил 4,38 ± 2,42 и 5,58 ± 3,58 соответственно; аналогичные показатели для группы 2 составили 15,00 ± 3,00 и 27,50 ± 5,50 соответственно. По прошествии 12 месяцев мы наблюдали ухудшение достигнутых результатов в обеих группах. В Группе 1 средний балл составил 6,31 ± 2,43 для основного опросника DASH и 7,37 ± 4,72 для дополнительного опросника DASH; во 2-й группе - 20,43 ± 3,82 и 41,25 ± 9,50 по обоим показателям DASH соответственно.Во 2-й группе результаты лечения были достоверно хуже как через 6 месяцев, так и через 12 месяцев после травмы. Заключение.Хирургическое лечение по эффективности превосходит консервативное даже при застарелых разрывах.
Text of the scientific article The effectiveness of postoperative rehabilitation protocol following pectoralis major tendon repair
Background . Rupturing the pectoralis major tendon (PMT) is a rare type of injury that most often occurs in weightlifters. This injury is also encountered among boxers, arm wrestlers and other sportspeople, however, they are exclusively male, and mostly between 20 and 40 years old [1, Ошибка! Источник ссылки не найден. ]. In recent years the occurrence rate of this type of injury has grown which is explained by an increasing interest in, and promotion of, a healthy lifestyle and a growing popularity of gyms [2-5]. Injuring the PMT results in being unable to do sports to the full capacity and limits the motion range of the upper extremity corresponding to the location of the injury. Surgical treatment has been observed to produce excellent results from the perspective of restoring muscular strength of the upper extremity [1, Ошибка! Источник ссылки не найден. ]. Therefore, for patients wishing to return to their sporting activities, surgical treatment should be the preferred choice. It is obvious that surgery alone will not be sufficient to ensure that muscular strength is fully restored. Surgery must always be complemented by a suitable rehabilitation plan.
Anatomy and the Specifics of Biomechanics
Understanding of anatomy and biomechanics of the pectoralis major may be of great assistance when deciding on an individual rehabilitation plan. The pectoralis major plays a significant role in ensuring the proper functioning of the upper extremity. It is involved in shoulder abduction, internal rotation, and flexion. The insertion sites of this muscle are as follows: proximally – clavicle, sternum, costal cartilage of the first six ribs and the fasciae of the rectus abdominus muscle, distally – the crest of the greater tubercle of the humerus. The muscular fibres of the pectoralis major cover the pectoralis minor muscle and most of the anterior thoracic surface. The insertion of the PMT to the humerus is specific. The tendinous fibers are twisted relative to the axis of the tendon: the lower fibres are inserted into the upper part of the crest, while the upper fibers are inserted into the lower part of the crest. Wolfe S.W. et al. have experimentally demonstrated that the inverse insertion of the PMT results in excessive tension of the lower portion of the tendon when it is extended while significant force is applied. This inverse insertion is therefore a risk factor in rupturing the PMT. The lower portion of the tendon is disproportionally extended in the final stretch of shoulder extension, at a point within the final 30º of the motion range [ Ошибка! Источник ссылки не найден. ].
The aim of the study is to assess the effectiveness of postoperative rehabilitation protocol following PMT repair.
Materials and methods
The study includes the results of treatment of 33 patients, average age was 28.5±4.0. 5 (20 – 38) underwent treatment for PMT ruptures.
28 patients underwent surgical treatment, 5 patients refused from surgical treatment, so they were assigned a physiotherapeutic rehabilitation procedure. 5 of them had old (neglected) ruptures, i. e. over 6 months after the injury. All patients were treated conservatively over the period of 8 to 20 weeks before surgery in different orthopedic centers. In all cases, the patients had been receiving inadequate treatment because they had been initially diagnosed with rotator cuff tears.
Surgical technique and rehabilitation protocol
The postoperative rehabilitation consisted of four consecutive stages. The ultimate goals of postoperative rehabilitation were defined as follows: 1) restoring the functional motion range in the shoulder joint; 2) restoring the maximum strength in the extremity possible (at least 90% of the strength of a healthy extremity); 3) reengaging in physical and routine activity at the pre-surgery level.
The first stage begins immediately after the surgery and lasts 3 weeks. The upper extremity is immobilized in sling. During the first 24 hours after the operation, it is very important, to mobilize the extremity as early as possible. On the other hand, it is crucial not to compromise the integrity of the tendon in the setting of the postoperative oedema and local underperfusion. The aims of the first stage of rehabilitation can be formulated as follows: 1) retaining the result attained via surgery; 2) resolving the postoperative oedema; 3) eliminating the pain syndrome; 4) retaining muscle tone. Starting from the 2nd week, patients begin to perform passive flexion of the shoulder joint (up to 45–50º), as well as abduction of the same joint (up to 30–35º), and external rotation of the joint to a physiologically neutral position. It is not allowed to perform active movements, including isometric exercise. Having encountered a stable oedema that lasted 10 days (1 case), we applied electrical stimulation to a positive result.
The second step begins after immobilization and lasts 3 weeks. The aims of this period are as follows: 1) increasing the motion range; 2) restoring muscular strength.
Table 1
Schedule: Restoring Shoulder Range of Motion in Postoperative Rehabilitation
|
Week after the surgery |
External rotation from a physiologically neutral position |
Flexion |
Abduction |
|
1 |
Immobilization in Sling |
||
|
2 |
0 |
45-50 |
30-35 |
|
3 |
5 |
50-55 |
35-40 |
|
4 |
10 |
50-65 |
40-45 |
|
5 |
15 |
60-75 |
45-50 |
|
6 |
20 |
65-80 |
50-55 |
|
7 |
25 |
70-90 |
55-60 |
|
8 |
30 |
75-105 |
60-65 |
|
9 |
35 |
80-110 |
65-70 |
|
10 |
40 |
90-120 |
70-75 |
|
11 |
45 |
95-130 |
75-80 |
|
12 |
50 |
100-150 |
80-90 |
Week 6 following the operation saw the onset of the third, 6 weeks, stage of the rehabilitation plan. The main aims of this stage are postulated as restoring the complete motion range and partially restoring muscular strength. The volume of both passive and active movements in the shoulder joint was consistently increased at the same speed as before, which is by 5º per week. During Week 6, isometric exercise for the pectoralis major with the upper extremity adducted were introduced (performed at partial capacity). In Weeks 7–8 patients are introduced to exercises from the prone position, with the upper extremity outstretched forward. By Week 12, the isometric strain of the pectoralis major was performed from the abduction position: in two of the cases, a 90º abduction was attainable, and in the remaining cases the abduction range varied from 70º to 80º.
Rehabilitation as a Method of Conservative Treatment
The aims of rehabilitation remained largely unchanged if surgical treatment was discarded as a treatment option: 1) restoring the functional motion range in the shoulder joint; 2) restoring the maximum strength possible; 3) reengaging in physical activity at the pre-surgery level. Due to objective reasons, the third aim above did not imply that the patient was expected to be able to resume power exercise at the pre-surgery level immediately following the completion of the rehabilitation plan. In this case, rehabilitation also consisted of four stages with the following differences (Table 2):
Table 2.
Restoring Shoulder Motion Range in Conservative Treatment
|
Week after the surgery |
External rotation from a physiologically neutral position |
Flexion |
Abduction |
|
1 |
Immobilization in Sling |
Immobilization in Sling |
Immobilization in Sling |
|
2 |
0 |
45-50 |
30-35 |
|
3 |
0 |
50-55 |
35-40 |
|
4 |
5 |
50-65 |
40-45 |
|
5 |
10 |
60-75 |
45-50 |
|
6 |
15 |
65-80 |
50-55 |
|
7 |
20 |
70-90 |
55-60 |
|
8 |
25 |
75-105 |
60-65 |
|
9 |
30 |
80-110 |
65-70 |
|
10 |
35 |
90-120 |
70-75 |
|
11 |
40 |
95-130 |
75-80 |
|
12 |
45 |
100-150 |
80-90 |
Treatment results were assessed in both groups at 6 and 12 months after treatment. In both groups, the outcomes were assessed using the basic DASH scoring questionnaire (Disabilities of the Arm, Shoulder, and Hand – a scoring scale designed to assess the degree of incapacitation of the upper extremity) and its supplement that focuses on sports-related functions, which consist of 30 and 4 items respectively.
Statistical assessment
For the statistical analysis of results, Statistica 10.0 for Windows (StatSoft Inс., USA) was used. Quantitative variables were described using standard variation statistical methods, for which the arithmetic mean (М), standard deviation (δ), 25th and 75th percentiles, and median patient number were calculated. The average values were presented as М + δ. The qualitative variables were described as absolute and relative frequency ratios (percentages). Differences were considered significant at р < 0.05. To evaluate results, the statistical analysis methods used included Student’s t-test.
Results
At first point of assessment – before surgery the average DASH (basic) score for patients in Group 1 (surgical treatment) was 54.04±5.8 and 84.60±7.57 DASH (sports-focused questionnaire) score. In the Group 2 (conservative treatment), the average scores were 52.66±6.49 and 85.00±7.00 respectively.
After 6 months postoperative rehabilitation in Group 1, the average score according to the basic DASH questionnaire and its sports-focused supplement was 4.38±2.42 and 5.58±3.58, respectively; the same indices for Group 2 were 15.00±3.00 and 27.50±5.50, respectively.
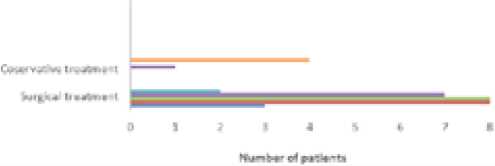
Following 12 months, we observed a deterioration of the results attained in both groups. In Group1, the average score was 6.31±2.43 for basic DASH questionnaire, and 7.37±4.72 for supplementary DASH questionnaire; in Group 2 20.43±3.82 and 41.25±9.50, for both DASH scores, respectively.
In Group 2 treatment results were reliably worse both 6 months and 12 months after the injury.
After 6 months, the average improvement in Group 1 was 13.99 points (p=0.00318) greater according to the basic questionnaire and 20.85 points (p=0.03761) greater according to the supplementary questionnaire (Figure 1).
After 12 months, in Group 1 were better according to the basic questionnaire in 17.48 points (p=0.00026) better and in 32.59 points (p=0.01095) according to the supplementary questionnaire (Figure 2). Over the period of 12 months after surgery, no complications whatsoever, including any infectious complications, were observed. We did not observe any cases of PMT rupture relapse, either. In all cases, we were able to eliminate the cosmetic defect (Figure 2).
-
Figure 1. DASH score (6 months after treatment).
D SIH 5 CT HE 16 *«Q4TH1 AFTER TREATMENT ■ 44 ™я и fH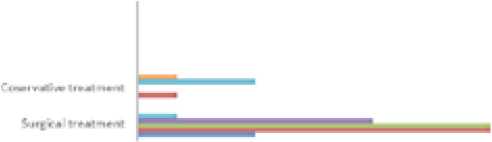

Discussion
The reasons underlying the rupture of the tendon remain difficult to establish accurately. However, it is known that most frequently, the injury occurs when applying eccentric force, or during extension, when the muscle stretches while working in the yielding mode, specifically, when performing bench-presses [1-5]. Another mechanism whereby this injury may occur is an abrupt simultaneous abduction and external rotation of the arm [2,7]. Ruptures of the pectoralis major tendon because of direct injury usually occur in skateboarders, rugby players and American football players. Some researchers report a correlation between the occurrence rate of these ruptures and the intake of anabolic steroids [Ошибка! Источник ссылки не найден.].
-
Figure 2. DASH score (12 months after treatment).
омм icon I (it moni hs *11 ie rm aim ini)
*
Many authors also mention that the PMT rupture diagnosis is established clinically, with MRI often becoming the method of choice to confirm the diagnosis [ Ошибка! Источник ссылки не найден. ], and the doctor uses it solely to ascertain the correctness of their conclusion that is based on the patient’s complaints and the clinical examination data. In some cases, the diagnosis can be confirmed via ultrasound scanning. It is also noteworthy that traditional radiographic scanning is of limited diagnostic value.
Interestingly, in some cases due to the rare occurrence of this type of injury, doctors misdiagnose it as muscle sprain and assign conservative treatment even when presented with complaints typical of PMT rupture and matching clinical evidence [ Ошибка! Источник ссылки не найден. ]. Simultaneously, many authors point out that surgical treatment is preferable when addressing both acute and old ruptures [ Ошибка! Источник ссылки не найден. , Ошибка! Источник ссылки не найден. ,5].
Conservative treatment helps the patients achieve a better quality of life and partially increase muscular strength, especially by using externally applied orthopaedic devices – orthoses [8-9]. However, conservative treatment techniques do not correct the cosmetic defect [ Ошибка! Источник ссылки не найден. ], and using orthoses cannot compare to restoring muscular strength in the long-term postoperative perspective.
Various techniques of early surgical treatment are known to practitioners. One technique implies decorticating of the humerus in the projection of tendon insertion and attaching the tendon with screws or anchors (3 to 5), or with button fixators. Another technique is as follows: a bone fragment is resected in the humerus in the projection of tendon insertion, and then the tendon is attached within the cavity created in the bone using fixators of various types. Using all these techniques, it is feasible to achieve good and excellent postoperative outcomes, which also provides the surgeon with a certain degree of freedom in choosing the method of treating this injury [1].
Conclusions
-
1. While establishing the diagnosis, demographic markers may point to a PMT rupture. The typical patient is a man between 20 and 40 years old who engages in power and/or high-energy kinds of
-
2. Statistical analysis data attest to the fact that treatment results as assessed following 6 and 12 month after the injury are verifiable better in patients who have undergone surgery as opposed to those who were only treated conservatively. It is interesting to note that the maximum result is achieved after 6 months of treatment, and then a deterioration is observed. However, that deterioration is more prominent in the conservative treatment group, and after 12 months the gap between treatment outcomes in the two groups under examination widens still further.
-
3. With all the above in view, it can be stated that from the perspective of short-term observation, surgical treatment exceeds conservative treatment in efficiency; and thus, in our opinion, surgical treatment is preferable for PMT ruptures. It should not go without mentioning that the statistical sample in this study is rather small and further research is required to confirm the findings herein.
sports. To confirm the diagnosis, shoulder joint MRI should be used, and if that is not available, it should be replaced with ultrasound scanning, although the former method is preferable. Traditional radiology has no diagnostic value regarding PMT ruptures.
Лычагин А.В., Грицюк А.А., Жидиляев А.В., Гаркави А.В., Липина М.М., ЭФФЕКТИВНОСТЬ ПРОТОКОЛА ПОСЛЕОПЕРАЦИОННОЙ РЕАБИЛИТАЦИИ ПОСЛЕ ВОССТАНОВЛЕНИЯ СУХОЖИЛИЯ БОЛЬШОЙ ГРУДНОЙ МЫШЦЫ// Кафедра травматологии и ортопедии. 2020.№4. С. 43-48. [Lychagin A.V., Gritsyuk A.A., Zhidilyaev A.V., Garkavi A.V., Lipina M.M., The effectiveness of postoperative rehabilitation protocol following pectoralis major tendon repair Department of Traumatology and Orthopedics. 2020.№4. pp. 43-48]
Финансирование: исследование не имело спонсорской поддержки
Funding: the study had no sponsorship
References The effectiveness of postoperative rehabilitation protocol following pectoralis major tendon repair
- Wolfe S.W., Wickiewicz T.L., Cavanaugh J.T. Ruptures of the pectoralis major muscle, an anatomic and clinical analysis. Am J Sports Med 1992; 20:587-593. DOI: 10.1177/036354659202000517
- Uchiyama Y., Miyazaki S., Tamaki T., Shimpuku E., Handa A., Omi H., Mochida J. Clinical results of a surgical technique using endobuttons for complete tendon tear of pectoralis major muscle: report of five cases. Sports Medicine, Arthroscopy, Rehabilitation, Therapy & Technology 2011, 3:20. DOI: 10.1186/1758-2555-3-20
- Butt U., Mehta S., Funk L., Monga P. Pectoralis major ruptures: a review of current management. Journal of Shoulder and Elbow Surgery 2015; 24(4):655-662. DOI: 10.1016/j.jse.2014.10.024
- Provencher M., Handfield K., Boniquit N. et al. Injuries to the Pectoralis Major Muscle: Diagnosis and Management. American Journal of Sports Medicine 2010; 38(8):1693-1705. DOI: 10.1177/0363546509348051
- Kavalersky G.M., Sereda A.P, Nikiforov D.A., Koshelev I.M., Kapyshev S.V. Ruptures of the pectoralis major muscle and its tendon: review of the literature and our experience in the treatment. Traumatology and Orthopedics of Russia. 2015; (2):117-131.
- Bayon O.A., Sandoval E., Mora V.M. Acute Pectoralis Major Rupture Captured on Video. Case Rep Orthop 2016; 2016:2482189. DOI: 10.1155/2016/2482189
- Manske R.C., Prohaska D. Pectoralis major tendon repair post surgical rehabilitation. N Am J Sports PhysTher 2007 Feb; 2(1):22-33.
- McIntire S., Boujie L., Leasiolagi J. Pectoralis Major Injury During Basic Airborne Training. J Spec Oper Med 2016 fall; 16(3):11-14.
- Moore J. Functional orthosis post pectoralis muscle rupture. Journal of Hand Therapy. 28 (2015) 325e328. DOI: 10.1016/j.jht.2014.11.005
