Treatment of clavicle fractures by Ilizarov technique

Author: Bari Mofakhkharul, Shahidul Islam, Shetu Nazmul Huda, Mahfuzer Rahman
Journal: Гений ортопедии @geniy-ortopedii
Section: Оригинальные статьи
Article in issue: 2, 2016.
Free access
Recently, the traditional treatment of patellar fractures is often complicated by infection and insecure fixation. Occurring complications can be treated promptly, which is cost-effective, but limits the function of the joint. The CEF apparatus proposed by us can effectively treat patella fractures with fewer complications. Transverse fractures of the patella with displacement were treated according to the method of compression external fixation, based on the principles of the Ilizarov apparatus with stretched spokes. All patients after the operation were allowed to move in the joints and load. In total, twenty-five fractures were treated with our CEF apparatus. Treatment in 12 patients was by percutaneous procedure. In the treatment of all fractures, a lasting fusion was achieved. The CEF apparatus was removed after 6-8 weeks. In 12 patients the total volume of movements was restored, the average assessment of knee joint function by Insall was 96 points, the average observation period was four years. Mild complications in the form of inflammation in the area of the spokes were observed in five patients, they were treated with local remedies and antibiotics. The CEF technique is a safe and effective method of treating patella fractures, it has advantages over conventional methods in the case of soft tissue deficiency. CEF provides rapid recovery without any additional surgical interventions.
Short address: https://sciup.org/142134614
IDR: 142134614 | UDC: 616.717.2-001.5-089.227.84 | DOI: 10.18019/1028-4427-2016-2-33-35
Text of the scientific article Treatment of clavicle fractures by Ilizarov technique
Despite being a common fracture, representing 5-10 % of all orthopedic fractures [1], evidence of optional treatment of displaced clavicle fracture is still ambiguous [2]. Primary surgical treatment of displaced midshaft clavicle fractures, with locking plate osteosynthesis as the preferred method, to result in good functionally high union rate and few complications [3-5] – the nonunion rate is reported as high as 20 % and close to 30 % of all patients are reported to have symptomatic malunion [3]. Structurally the clavicle is a spongy bone since its internal lumen is filled with cellular bone and there is no intramedullary canal. Our research has shown that an axial wire in the spongy bone provides sufficient rigidity for the fixation of splinters, even in cases of minimum axial compression.
MATERIALS AND METHODS
For the last 17 years (1999-2015) 28 cases of fracture clavicle were operated by the Ilizarov technique. The follow up period was 1-15 years. Male predominated with an average age of 45 yrs. as demonstrated in table 1.
Table 1
Shows sex incidence
|
Sex |
Qty |
Percentage |
|
Male |
20 |
71 |
|
Female |
08 |
29 |
Indications for Ilizarov external fixation are:
-
1. Fractures of various severity levels;
-
2. Fracture-dislocation;
-
3. Dislocation of acromial end of clavicle.
The Ilizarov parts are:
-
1. 2 plates;
-
2. Posts;
-
3. Wire fixators;
-
4. Connecting rods.
2016. № 1. С. 33-35.
Surgical procedure
The patient is administrated regional anaesthesia placed under sedation. The operation is performed with the patient supine, with a cushion along (C7-D7) and his or her forearm behind the back. The patients head is turned in the direction opposite to the injured clavicle but it should not be thrown back, the side of the face must be level with the anterior aspect of the chest. First, the wire insertion points are determined from radiographs in two projections. Radio-opaque markers are placed 2 cm from the joint surfaces of the acromial to the anatomic axis of the bone fragments. Injection needles are also placed to mark the anterior and posterior boundaries of the bone fragments at the insertion levels of the transosseous elements.
Mounting of the device starts from the medial support. The wires are manually fixed in the extreme holes of the connection plate and using wire fixators, so that their guiding ends only slightly protrude over the edge of the plate. The plate is applied onto the skin and the wire directed towards the sternal extremity of the clavicle and manually inserted to the bone. One should again make sure that the wire is located from the upper aspect of the clavicle and in the centre of the bone diameter. A reference point is marked on the wire showing the depth of its insertion and indicating the depth at which it will exit from the lower cortical plate. The bar is then moved away from the skin by 1.5-2 cm. The second wire is inserted until it touches the bone and after making sure that it is located in the centre of the clavicle
Ш Bari M.M., Islam Shahidul, Shetu N.H., Mahfuzer R.M. Treatment of clavicle fractures by Ilizarov technique // Гений ортопедии.
diameter, the first wire is fixed rigidly to the support. After the second wire is inserted and fixed, the support is similarly mounted on the peripheral fragment [14, 15, 16].
Postoperative protocol
In the operating rooms, after the axial compression wires have been tensioned, the skin around the wires is examined. A pressure bandage in the form of a sling is applied to the area of the axial compression wire insertion. During first 3-4 days, dressing are changed daily, then as required but not less frequently than every 7-10 days. X-ray can be done after 10 days. In fracture clavicle, the structure is generally dismantled within 5-6 weeks.
Case illustration
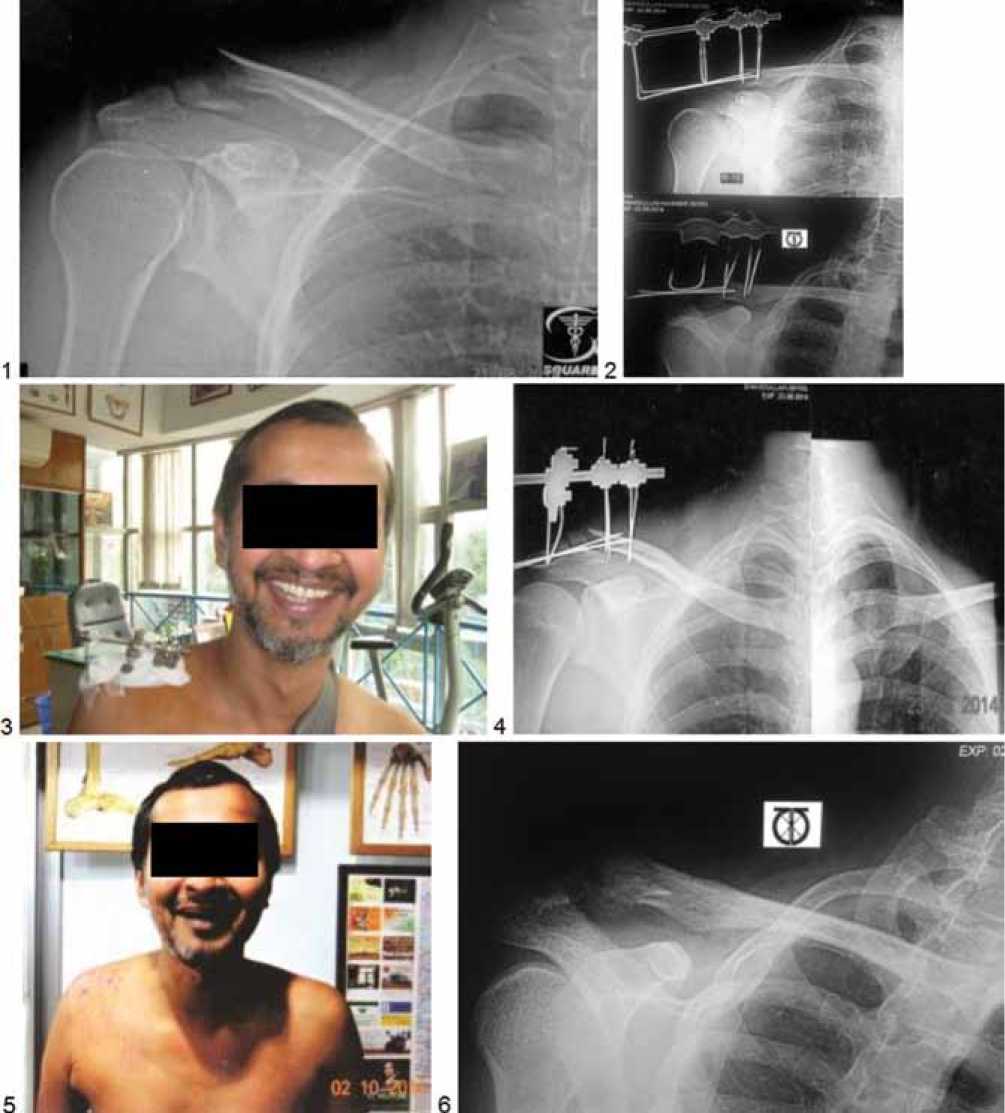
Fig. 1.: 1 – 12 days old fracture proximal right clavicle; 2 – Radiograph of right clavicle after surgery (2nd post-op); 3 – Mini Ilizarov apparatus on the right clavicle of 39 yrs. old male; 4 – Radiograph with union of the fragments after 6 weeks; 5 – Clinical appearance of the patient after removal of the mini Ilizarov apparatus; 6 – Final radiograph of the right clavicle with full consolidation after 2 months follow up
RESULTS
Osteogenesis was achieved in all the 26 patients. Two local care with antibiotics. There were no incidents of patients had a pin track infection which was treated by neurovascular complications.
DISCUSSION
The mini Ilizarov method for the management of fracture clavicle have many advantages. However, several technical problems can arise if the details of the technique are not allowed precisely. The inexperienced surgeons usually fails to carry out of the whole technique. For successful tissue genesis one must follow the rules and processes of Ilizarov technique. It is evident that regeneration of the bone can be obtained safely. The research and review of existing literature revealed few publications for fracture clavicle treated nonoperatively. The factors that could influence development of clavicular nonunion included, presence of fracture comminution, complete fracture displacement, increased age, and fracture shortening. Fracture displacement following a clavicle fracture was reported to predict pain and dysfunction in two studies both with follow up of more than two [6, 7] years. In this study fracture displacement was formed to be a predictor for nonunion in all but one publication reporting on this subject [8, 9, 10, 11, 12]. Shortening of the clavicle following a midshaft clavicle fracture has been found to be associated with inferior clinical outcome [13].
A publication by Nowak et al. recognized fracture comminution as a significant risk factor for pain, strength reduction and cosmetic defects after a clavicle fracture but not as a predictor for nonunion(6). We found two cohort studies of large sample size reporting comminution to be a predictor for nonunion in midshaft fracture [8, 9]. All existing randomized studies comparing surgical and nonsurgical treatment of displaced midshaft fractures favour surgical treatment based on slightly better functional outcome.
CONCLUSION
Fracture clavicle with displacement can be easily treated by mini Ilizarov apparatus. Displacement seems to be the most likely factor that is responsible for nonunion. Treating all clavicle fractures with displacement surgically would inevitably lead to over treatment, which is why future studies need to focus on mini Ilizarov surgery and those who would not. Introducing one K-wire through the fragments and fixing the fragments externally by mini Ilizarov apparatus gives excellent result and better outcome.
References Treatment of clavicle fractures by Ilizarov technique
- Robinson C.M. Fractures of the clavicle in the adult. Epidemiology and classification//J. Bone Joint Surg. Br. 1998. Vol. 80, N 3. P. 479-484.
- Fractures of the clavicle/L.A. Khan, T.J. Bradnock, C. Scott, C.M. Robinson//J. Bone Joint Surg. Am. 2009. Vol. 91, N 2. P. 447-460.
- Clavicle fractures may be conservatively treated with acceptable results -a systemic review/I. Ban, U. Branner, K. Holck, M. Krasheninnikoff, A. Troelsen//Dan. Med. J. 2012. Vol. 59, N 7. P. A4457.
- Operative versus non-operative treatment for clavicle fracture: a meta-analysis/G.D. Liu, S.L. Tong, S. Ou, L.S. Zhou, J. Fei, G.X. Nan, J.W. Gu//Int. Orthop. 2013. Vol. 37, N 8. P. 1495-1500.
- Locking plate osteosynthesis of clavicle fractures: complication and reoperation rates in one hundred and five consecutive cases/M. Fridberg, I. Ban, Z. Issa, M. Krasheninnikoff, A. Troelsen//Int. Orthop. 2013. Vol. 37, N 4. P. 689-692.
- Nowak J., Holgersson M., Larsson S. Can we predict long-term sequelae after fractures of the clavicle based on initial findings? A prospective study with nine to ten years of follow-up//J. Shoulder Elbow Surg. 2004. Vol. 13, N 5. P. 479-486.
- Outcome of clavicular fracture in 89 patients/A. Eskola, S. Vainionpää, P. Myllynen, H. Pätiälä, P. Rokkanen//Arch. Orthop. Trauma Surg. 1986. Vol. 105, N 6. P. 337-338.
- Risk factors for nonunion after nonoperative treatment of displaced midshaft fractures of the clavicle/I.R. Murray, C.J. Foster, A. Eros, C.M. Robinson//J. Bone Joint Surg. Am. 2013. Vol. 95, N 13. P. 1153-1158.
- Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture/C.M. Robinson, C.M. Court-Brown, M.M. McQueen, A.E. Wakefield//J. Bone Joint Surg. Am. 2004. Vol. 86-A, N 7. P. 1359-1365.
- Vertical fragment in adult midshaft clavicle fractures: an indicator for surgical intervention/S.J. Kirmani, S.K. Pillai, B.R. Madegowda, S.A. Shahane//Orthopedics. 2009. Vol. 32, N 10. P. 9-14 DOI: 10.3928/01477447-20090818-06
- Midshaft fractures of the clavicle with a shortening of more than 2 cm predispose to nonunion/M. Wick, E.J. Müller, E. Kollig, G. Muhr//Arch. Orthop. Trauma Surg. 2001. Vol. 121, N 4. P. 207-211.
- Hill J.M., McGuire M.H., Crosby L.A. Closed treatment of displaced middle-third fractures of the clavicle gives poor results//J. Bone Joint Surg. Br. 1997. Vol. 79, N 4. P. 537-539.
- Deficits following nonoperative treatment of displaced midshaft clavicular fractures/M.D. McKee, E.M. Pedersen, C. Jones, D.J. Stephen, H.J. Kreder, E.H. Schemitsch, L.M. Wild, J. Potter//J. Bone Joint Surg. Am. 2006. Vol. 88, N 1. P. 35-40.
- Ilizarov G.A. Transosseous osteosysthesis. Theoretical and Clinical Aspects of the Regeneration and Growth of Tissue. Springer-Verlage, 1992. P. 450-452.
- Bari M.M. A color atlas of limb lengthening, surgical reconstruction and deformity correction by Ilizarov technique. 2013. P. 75.
- Treatment of fracture clavicle by Ilizarov Technique/M.M. Bari, S. Islam, N.H. Shetu, M. Rahman//Orthop. Rheumatol. Open Access J. 2015. Vol. 1, N 2. ID 555560.
