Working conditions and occupational risks of migrant women (CTM textile factory case study)
")
Author: Jasrotia B., Sharma R.
Journal: Регионология @regionsar
Section: Социальная структура, социальные институты и процессы
Article in issue: 2 (127) т.32, 2024.
Free access
Introduction. Gender inequality in the workplace is not a new phenomenon, yet gender differences in working conditions and womenʼs involvement in the workplace are poorly understood. Women are often discriminated against in the workplace and their working conditions and wages are substandard. On their own, they are not always able to improve their working and social life and achieve better protection at work. This study aims to explore the working conditions and risks faced by migrant women working in one of the oldest and largest STM textile factories in Jammu and Kashmir, India.
Women migrants, working conditions of women migrants, gender discrimination, womenʼs occupational risks
Short address: https://sciup.org/147243834
IDR: 147243834 | UDC: 349.24-055.2:314.7 | DOI: 10.15507/2413-1407.127.032.202402.263-277
Условия труда и профессиональные риски женщин-мигрантов (на примере текстильной фабрики CTM)
Введение. Гендерное неравенство на рабочем месте - явление не новое, тем не менее гендерные различия в условиях труда и вовлеченности женщин в производственную деятельность мало изучены. Женщины часто подвергаются дискриминации на работе, их условия труда и заработная плата не соответствуют нормам. Самостоятельно они не всегда способны улучшить свою трудовую и социальную жизнь и добиться повышения уровня защиты на производстве. Цель исследования - изучить условия труда и риски, с которыми сталкиваются женщины-мигранты, работающие на одной из старейших и крупнейших текстильных фабрик СТМ в Джамму и Кашмире (Индия).
Text of the scientific article Working conditions and occupational risks of migrant women (CTM textile factory case study)
Контент доступен под лицензией Creative Commons Attribution 4.0 License.
This work is licensed under a Creative Commons Attribution 4.0 License.
Conflict of interest. The authors declare no conflict of interest.
Acknowledgement. The authors would like to thank all female respondents for participating in the study and for sharing their personal experiences. The authors also thank the reviewers for their valuable comments, which improved the quality of the manuscript.
Условия труда и профессиональные риски женщин-мигрантов(на примере текстильной фабрики CTM)
Б. Джасротия1, Р. Шарма2 Н
-
1 Колледж Халза ( г. Амритсар, Индия )
-
2 Университет Гуру Нанак Дев ( г. Амритсар, Индия ) Н rachana.sociology@gndu.ac.in
Введение. Гендерное неравенство на рабочем месте ‒ явление не новое, тем не менее гендерные различия в условиях труда и вовлеченности женщин в производственную деятельность мало изучены. Женщины часто подвергаются дискриминации на работе, их условия труда и заработная плата не соответствуют нормам. Самостоятельно они не всегда способны улучшить свою трудовую и социальную жизнь и добиться повышения уровня защиты на производстве. Цель исследования ‒ изучить условия труда и риски, с которыми сталкиваются женщины-мигранты, работающие на одной из старейших и крупнейших текстильных фабрик СТМ в Джамму и Кашмире (Индия).
Материалы и методы. Целенаправленная выборка включала 240 женщин-мигрантов с текстильной фабрики СТМ. Они были опрошены в четырех рабочих колониях и внешних жилых районах с помощью серии интервью. В исследовании используются смешанные методы - количественные и качественные. Наблюдение, серия интервью применялись для количественной оценки данных и предоставления детальной качественной информации.
Результаты исследования. Анализ ответов женщин свидетельствует, что условия труда на фабрике СТМ не соответствуют международным нормам: отмечались случаи травматизма, отсутствие денежной компенсации за них, не все работницы обеспечены необходимыми средствами защиты для работы с опасными химическими веществами и токсинами, поэтому сообщают о плохом самочувствии, недомоганиях, язвах, усталости и судорогах. Выявлено, что женщины-мигранты подвергаются дискриминации по половому признаку, преследованиям, физическому насилию. Определены также и другие факторы, угрожающие психическому, эмоциональному и физическому здоровью на рабочем месте.
Обсуждение и заключение. Авторы пришли к выводу, что женщины-мигранты продолжают работать в неподобающих условиях, подвергая свое здоровье опасности и становясь жертвами эксплуатации. Полученные результаты подчеркивают необходимость проведения инклюзивной политики и вмешательства, а также переоценки существующей трудовой практики для решения проблем, которые способствуют уязвимости трудящихся-мигрантов. Материалы статьи будут полезны региональным властям, защитникам прав трудящихся и женщин, которые заинтересованы в решении конкретных проблем этой уязвимой группы населения. Данное эмпирическое исследование может принести пользу ученым, интересующимся темами гендера, миграции, условиями труда.
RUSSIAN JOURNAL OF REGIONAL STUDIES. Vol. 32, no. 2. 2024 J^ Для цитирования: Джасротия Б., Шарма Р. Условия труда и профессиональные риски женщин-мигрантов (на примере текстильной фабрики CTM) // Регионология. 2024. Т. 32, № 2. С. 263–277.
Introduction. The study of migrant women workers in developing countries and their employment conditions and occupational hazards is of a great relevance as the issues of gender dynamics intersect with labour migration patterns. Although, the employment scenario in India is transforming yet issues of women’s employment remain complex and deeply entrenched in social-cultural norms, economic structures and is mentally dominated by historically formed conditions such as caste.
According to ‘ Women in The Informal Economy ’ report India’s informal sector, which employs nearly 90% of its labour force, constitute of the 9.6 crore women who are involved in wide range of activities and contribute to the national economy as ‘invisible labour’1. Migrant women workers are largely engaged in the informal or semi-formal economy with a large absorption in the construction sector (nearly 15‒20%), domestic work (80%), garment and textile (60‒70%), agriculture (30%) and various other informal activities.
The key objective of this paper is to examine the workplace vulnerabilities, risks and occupational health hazards that migrant women workers face while working at CTM.
Occupational Hazards. Occupational hazards have been defined as any form of long- or short-term dangers/ risks associated with unhealthy workplace environments [1] and pose health and safety risks not only to individuals but also impacts the economy and organizations at large. Occupational Safety and Health Administration (OSHA)2 identifies 6 categories of occupational hazards: safety, chemical, biological, physical, ergonomic, work organization hazards.
Studies of women workers in developing countries point out that women largely ignore their health and other personal concerns3 and succumb to exploitative conditions for living. Researches on labour migration sensitise us on the plight of the migrant workers who are exposed to a variety of occupational hazards, suffer from work related problems, diseases, disorders, psycho-social stresses and are injured or die because of accidents at work. They also inform us that women are more vulnerable to such dangers and vulnerabilities at work, and are more likely to make concessions at work and in their personal life, leave their positions, and be subjected to harassment.
M. Nihila revealed that women workers in India work in precarious conditions which have adverse effects on their health [2; 3]. Similarly, long working hours, absence of leave facilities, overcrowded and harsh working conditions affect the health of women workers [4]. P. Majumder emphasised that women workers face a double burden of work for wages4. Due to the overburden of work women workers do not get enough time for rest which leads to continuous fatigue, headache, back ache and sometimes fever too. S. Pathy finds out that due to shortage of time and long working hours, women generally neglect their health and mostly suffer from severe backache, dwindling of eye sight, mental and physical strain and other regular health issues such as cold, fever, jaundice, gastroenteritis and anaemia5. Furthermore, it was also found that due to the unaffordability and lack of knowledge women workers ignore reproductive health which results in permanent sterility and chronic pelvic inflammatory diseases6. A. Hogh and E. Viitasara elaborated that work place violence adversely affects the health of women workers such as poor mental health, fatigue and many more [5]. Therefore, the occupational hazards vary from the nature of activities, sectors women workers are involved in. Similar is observed in A. Biswas’s et al. review of fifty-eight studies on ’Sex and Gender Differences in Occupational Hazard Exposures’ concluded that men and women face different occupational hazards, and these differences may not only be due to the gender distribution of the labour force by occupation [6].
Although, the central Government and State Governments have enacted various acts and rules to safeguard the rights of the workers. The Factory Act 1948 (India) provides a list of provisions under various sections such as working environment of the workers should be clean and hygienic with proper ventilation and temperature, in case of dust and fumes employers should install exhaust appliances, no overcrowding, facility of drinking water, separate latrines and toilets for male and female workers and spittoons at workplaces (,. Yet, workers engaged in the informal sector become victims of occupational hazards.
Migrant Women Workers in Chenab Textile Mill (J&K). Migration inflow in Jammu and Kashmir has increased in the last two decades, despite the limited growth of large-scale industries especially in Kashmir region and development of the industrial sector in the plain areas of Jammu region. The first industrial policy of UT
RUSSIAN JOURNAL OF REGIONAL STUDIES. Vol. 32, no. 2. 2024 J^ of Jammu and Kashmir was announced in 1995 and then in 1998 and a comprehensive industrial policy for J&K was announced in 2004 and later in 2016. As a result, the industrial sector in the Union Territory (UT) is rapidly developing. Presently, there are approximately 25000 micro, small and medium enterprises in the UT that contribute to around 60 per cent of the total investment. Industrial activity is concentrated largely in three districts i.e., Jammu, Samba and Kathua of Jammu division. Census 2011 reveals that there are 28,09,629 million migrants from the states of Bihar, Uttar Pradesh, West Bengal, Madhya Pradesh, Rajasthan, Punjab and Haryana in Jammu and Kashmir7. The availability of work and high wages in Kashmir valley and the relatively secure and semi-permanent jobs in industries of Jammu attract labourers towards this region8 [7]. Migrant men and women are engaged in both organized and unorganized sectors in J&K.
Chenab textile mill is the largest and oldest industry (1961) of Union Territory (UT) of Jammu and Kashmir. Not only in the UT but also in Asia it is the largest single automatic mill which produces cotton yarn, textile yarn, dyed yarn, polyester yarn and acrylic yarn and exports its diversified products to large scale companies in India as well in foreign countries. The yarn manufacturing process involves about 13 steps and operations on several machines. The mill produces natural fibre and man-made fibre yarns. CTM currently employs more than 10,000 workers and around 1,000 staff members. A considerable number of migrant women workers, nearly 1266 (as per the factory record) are working as regular workers and casual workers (not on fixed term basis) since several years in CTM. There are many hazards at work that ladies in various jobs and machinery face on a regular basis. Despite the fact that CTM is the largest and oldest factory, no study has been conducted on the working conditions of workers, particularly migrant women workers, in such a large organised unit.
Literature Review. There are many review and meta-analysis articles written on occupational health and prevalence of violence against women workers in industrial settings both at international level as well as in India. However, there is a dearth of actual empirical works on the status of women workers in industrial settings and most of the research is very old (although they do not appear out-dated as not much significant changes have been noticed in the quality of work life in the industrial settings). Most of the works available are confined to Bangladesh, India and China.
S. I. Hasan et al. in his study provides an overview of the mental health outcomes among migrant workers in his meta-analysis of research from 2015 to 2021 [8]. Along With many other factors he also studies occupational factors (workplace psychosocial stressors, poor working conditions, salary and benefits issues, abuse) that impact mental health outcomes in migrant workers. Likewise, G. D. Brown also examines income disparities, working risks, disproportionate impact of gender-based violence and harassment on women workers in garment manufacturing units [9]. L. Miles et al., uses feminist lens to document how factory women migrant workers manage health needs in Malaysia [10]. Similarly, A. Gibbs’s in his research on workplace violence in Bangladesh’s garment industry brings out experiences of workplace violence (WVP) and its association with depression, intimate partner violence, and other struggles faced by the women workers [11].
Ch. Gannagé studies the worsening conditions of work, health and safety concerns of immigrant women workers in Toronto’s sportswear industry with the adoption of new Government and Managerial Strategies [12]. R. Fincher et al. writes in their paper series about the gendered experience of industrial labour. According to them, manufacturing labour in Australia is seen differently by immigrant men and women. They point out that women have greater levels of industrial segregation and occupational immobility9. Also, the types of training that women and men get after arriving in Australia, including language and job-related training and credentials, differ by gender. E. Küçük studied the health perception and lifestyle behaviour of female workers in food factory and found 20.9% as smokers, 36% slightly overweight and having average HLSB score at a medium level [13] in her work on the new class of workers, the Dagongmei, or working girls in factories (electronics factory in southern Chinaʼs Guangdong province) of China.
P. Ngai in his research discusses the workplace resistance and transgression concluding that chronic pains such as backaches and headaches that many of the women experience are as indicative of resistance to oppressive working conditions as they are of defeat [14]. S. Moyce and M. Schenekar discusses the occupational health and safety of migrant workers [15]. He calls their works as 3-D jobs‒dirty, dangerous, and demanding (sometimes degrading or demeaning). Also, the War on Wants report examines the common story of the insecure lives of female migrant workers in Thailand, Cambodia, and Malaysia, as well as the abuse and exploitation they experience at the hands of unscrupulous employers10.
In the context of India, following studies were found related to the situation of women workers in industrial settings. P. Verma and S. Agarwal’s study on the dangers that migrant workers experience in Lucknowʼs informal sector brings out the problems of musculoskeletal disorders, respiratory issues, and slips while working in factories [16]. S. Saima et al. investigate the health-related empowerment of 25 female workers in Sri Lankaʼs export-processing sectors [17]. The findings of this study show that, while the women workers at Katunayake EPZ were suffering from various types of physical and psychological health problems, there was a substantial variation in how they decided to deal with their health issues. Taking sick leave and investing in a better socioeconomic position in the future are two factors used to assess the empowerment of female EPZ employees. Another cross sectional descriptive study by V. Karvadi et al. on the health conditions of women working in garment in Bengaluru city inferred that musculoskeletal problems were the most common problems present among the study participants as they worked in standing posture for a longer time [18]. A. Mishra et al., also writes about the issue of work/labour, gender, and health and how work processes and conditions affect both their physical and mental wellbeing that gets manifested in somatic symptoms including chronic pain, irregular menstruation and constant pressure on the mind and body [19]. R. Lakhani et al. evaluate the frequencies of occupational health issues among women workers in the construction sector [20]. Respondents reported headaches and backaches, as well as limb pain, work-related injuries, respiratory, eye, and skin disorders, and noise-induced hearing loss (NIHL) as a result of exposure to hazards such as dust, noise, heat and cold, non-ionising radiation, and dry cement, glass and adhesives, tar, and paint.
Hence, on the basis of the review of the secondary literature following may be drawn:
-
a) several academics have reported on the social and economic precocity of women workers, the dangerous operation of industries, and the inadequate execution of safety regulations. Because many companies pay low salaries and often do not need heavy lifting owing to automation, women are increasingly engaged in the industrial environment at low-level positions;
-
b) violence against women in Indiaʼs factories is not well recorded, although it is a common occurrence in the lives of women who work in these industries. Young women, particularly single women, are especially exposed to assaults by their superiors. While reviewing the literature, incidences of ʻdeathʼ and ʻsexual assaultsʼ were noted in some of the most prominent global brands and companies which point out that it is easy for even the prestigious companies to save their shoulder when it comes to violations of rights of their workers.
Materials and Methods. For meeting key objective, 240 women migrant workers from CTM, Kathua (J&K) were interviewed from the workers colonies: CTM labour colony (336 total), and colonies outside the factory i.e., Rishi Nagar (90 total), Chaudhary Colony (110 total), Chak Ram Singh (95 total), Ram Nagar (82 total). Thirty respondents were selected from each area.
The factory’s database having the names and details of the workers was used as a sampling frame, in case of those respondents who were living in the CTM labour colony and every third house was interviewed through systematic sampling. However, in case of those living outside the CTM colony, purposive sampling method was used. Some of the respondents were also interviewed at the workplace to get more insights to the issues. A detailed interview schedule was used for interviewing the respondents. Some case studies from the sample were drawn for getting qualitative insights, no separate set of schedules was used for it.
Both qualitative and quantitative research methods were used in the present study. This helped in selecting participants who were relevant to the study and get deeper insights into the varied factors and complexity of the problems faced by the migrant women workers.
Results. The profile of the respondents indicates that most of the women working in CTM were in the age group of 18 to 37 years. Majority of the respondents, i.e., 38.33% belong to scheduled caste. About 30.83% of respondents belong to Other Backward Class followed by 25% from general caste. Only 5.84% of the respondents constitute Scheduled Tribes. Nearly, 64.16% of the women workers were illiterate and around three-fourth of the total respondents were found to be married. It was observed that around 27.50% of the total respondents had their monthly income up to 5000. Majority of the respondents, 70.42%, were having a monthly income between 5001 and 7000. Only 2.08% had monthly income above 7000. Table 1 provides context for the current study, which analyses the health difficulties that migrant women workers discovered after working in CTM.
T a b l e 1. Health Issues Noticed after Working11
|
Health Issues Noticed after Working Responses |
Per cent |
|
Weakness in body, swelling in hands and feet, frequent headache, pain in 238 whole body, anaemic Gastric, heart problem, respiratory problems 139 Heavy flow during periods, irregular periods, leucorrhoea, urinary tract infection 166 Skin diseases and allergy 9 Miscarriages 6 Total 558* |
42.65 24.91 29.74 1.62 1.07 99.99 |
Multiple Responses .
The problems stated above might appear to be common issues faced by women coming from poor socioeconomic backgrounds and it is possible that these health problems are related to inadequate nutrition or harsh treatment or patterns of socialization within the family. Yet, when the respondents were asked to differentiate between the pre-work and present work status and health concerns they were certainly able to state the differences that the long working hours, overtime work, exposure to chemicals, and other poor conditions of working had negatively impacted their health.
It was found that 42.45% of them felt weakness, pain in the whole body and frequent headache which somewhat might be due to various other reasons making it difficult to assess yet, the respondents attributed it to their current work. During field work, it was also observed by researchers that the majority of respondents were pale, looked anaemic and weak which also explains the health conditions of women coming from weaker sections in India and high prevalence of anaemia among them. Some of the respondents reported that weakness and standing for long hours cause swelling in their hands and feet. There were 24.91% of the respondents who had observed gastric, respiratory and heart related problems. A study by R. N. Ali et al. on women workers also inferred that mostly women suffer from frequent illness, headache, gastritis, earache and eye pain only after joining the garment industry [4]. Furthermore, 29.74% respondents were suffering from gynaecological problems like heavy flow during periods, irregular periods, leucorrhoea, and urinary tract infection.
-
11 All tables and figures in this article are compiled by the authors based on the materials of the conducted research.
Malti (23 years old), a single mother with four children, works as a casual worker in the Mixing unit. She mentioned that she was not feeling well on the first day of her period, but the needs of her children compelled her to go to work. She stated, “Once, while mixing the fibre, she began bleeding profusely and collapsed unconscious.” Then, with the assistance of other workers, they carried her to the hospital, and after receiving two bottles of glucose, she was able to walk. She went on to say that labourers work all day and only receive 20% of their pay. They are compelled to work in order to achieve both ends.
Lalita (26 years old), lives with her three children and husband. She and her husband work as regular salaried workers in CTM. They are happy after earning their livelihood. She said that after migration she has observed some health issues like Leucorrhoea and Urinary tract infection due to which there is continuous fatigue and pain in the whole body. She said she had visited many doctors but there was not any improvement as doctors suggested she use clean toilets to avoid infection. At CTM there are common toilets for both men and women and they are unhygienic too and even in the living place all the migrants share the toilet. In this situation, it has been impossible for her to recover from this problem.
These case studies show us that due to heavy workload migrant women workers were suffering from gynaecological problems. Similar findings were reported in another study that women workers suffer from malnutrition, anaemia, gastric, dysentery, diarrhoea, respiratory problem, gynaecological problems, tuberculosis and urinary tract infection [19]. Only 1.62% of respondents stated that they were suffering from skin disease and allergy. It was reported by one of the respondents that during the production process dust and cotton particle residues flow in the unit which cause allergy and respiratory problems among the workers. A small proportion of the respondents that is 1.07% had miscarriages. These respondents were newly married and of small age group. One of the respondents shared her experience, Asha (20 years old) got married three years ago. She migrated to Kathua after a few months of her marriage. Her brother-in-law and sister-in-law were already working in another factory in Jammu. With their help she also started working as a regular salaried worker in CTM. She said before she started working, her periods were regular but now she was facing the problem of irregular periods and even she had four miscarriages. She said due to financial crises she cannot take rest. She requested and pleaded to her husband to delay planning for the baby by one year, but he did not agree. She went on to say that every day, her spouse forces her to have a relationship, “but my body is not ready to bear a child, so I miscarry every time. Whenever I go to the doctor, she scolds me for not being aware. “I donʼt know what to do; a woman's life is so difficult”.
From these cases, it can be concluded that migrant women workers are helpless due to financial crises. They cannot leave their work despite health issues. In patriarchal society the burden of work life and household chores and reproduction further affects the health of migrant women workers.
Source of Treatment. It is noticed that the workplaces, like factories, industries where thousands of workers are engaged in the production process, do not have health facilities. However, it is the responsibility of employers to provide basic facilities like free health check-ups, tests and medicines to the workers so that they do not miss their duties.
As far as the regular check-up of the workers is concerned it was found that the factory administration does not provide any facility of regular check up at the workplace. Even in the factory premises there was no availability of a doctor or nurse to look after the emergency cases. Thus, in case of health issues respondents need to take treatment from other sources. However, the factory administration does not provide any treatment or regular check-up and tests to the workers. It is an unpleasant fact that in case of health problems, the workers have to go to different sources according to their convenience. It was found out that in order to save money and time, the workers prefer to visit local unqualified doctors and pharmacies.
Workers visit government hospitals, ESIC centres and medical stores etc. for treatment (Fig. 1). It was noticed in a study that women workers are unable to get treatment in the public hospitals because the officials do not behave properly and sometimes charge extra money from them [21]. It is true that visits to medical facilities by women may depend somewhat on their living conditions, educational status, financial status and other such variables but at the same time the work conditions also influence the health, health seeking behaviour and utilization of health services.
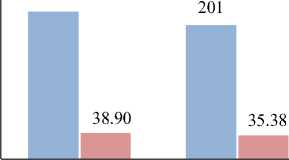
Unqualified Medical Chemist Shop
Practitioner

Government Hospital ESI Dispensary
-
■ Responses ■ Per cent
F i g. 1. Sources of Treatment
The figure given above reveals that the majority of the respondents i.e., 38.90% visit unqualified medical practitioners as they considered it easy to approach for immediate relief without missing their duties. There were 35.38% of the respondents who said they visit medical stores for medicines without any prescription from a doctor. It was found that 18.14% of the respondents got treatment from the government hospital. Only 7.57% of the respondents stated that they visited the ESIC dispensary for treatment. One of the respondents (25 years, from Bihar), narrated that, whenever there is any health issue like fever or pains in the body she prefers to visit a medical store or local doctor. She said her husband never takes precautions during intercourse thus many times she gets pregnant and takes medicine from the local doctor to eliminate the unwanted pregnancy. She further said, “In the ESI dispensary, medicines are not of good quality and even though it is far off place so many workers prefer to visit chemist shops and local doctors.”
Furthermore, when the researcher enquired this from medical store owners it was found that it is true that majority of migrant women depend on painkillers, paracetamol and even in case of unwanted early pregnancy women reach out to take medicines from chemist shops without any consultation. It can be analysed that the majority of the
RUSSIAN JOURNAL OF REGIONAL STUDIES. Vol. 32, no. 2. 2024 J^ respondents avoid visiting hospitals because the visiting hours of the hospitals and the working hours of the workers were the same. Secondly, workers did not trust the doctors and treatment provided by the ESI dispensaries. Even the majority of the respondents narrated that medicine given by the ESI dispensaries were not of good quality. It is necessary to clarify here that under the Indian Government Flagship health insurance scheme AB-PMJAY all poor and migrants are entitled to health cover of up to ₹5 lakhs per family per year. Number of poor has been benefited through this scheme yet there are several concerns and areas to be improved in order to make the healthcare system and services truly reach the most excluded groups and make it poor friendly.
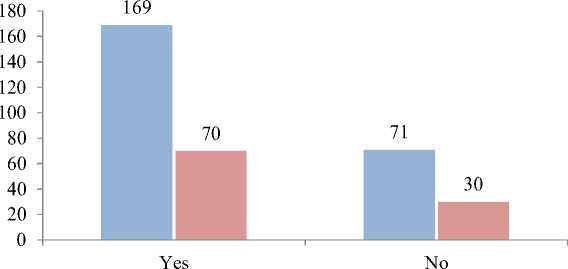
Work during Illness . In the above discussion it was found that migrant women workers were not conscious about their health. Majority of them did not visit professional doctors to identify the reasons behind health problems. Generally, they preferred to visit chemist shops for immediate relief by taking painkillers or paracetamol. They do not go for permanent solutions to get their health problems cured. Studies also reveal that due to long working hours and heavy workload women workers generally neglect their health12. Thus, here an attempt is made to understand the reasons for delivering duties even during illness (Fig. 2).
■ Responses ■ Per cent
F i g. 2. Working during Illness
It was revealed from the data that 70.42% of the respondents go to work even during illness as shown in Figure 2. As far as the reasons (Table 2) of delivering duties even during illness is concerned it was found that respondents largely ignore their illness and perform duties because of poverty and financial issues. They do not have any financial security thus they are left with only one option that is to work for survival.
T a b l e 2. Reasons of Working during Illness
|
Reasons of Working during Illness |
Responses |
Per cent |
|
Due to Poverty |
86 |
50.88 |
|
Demand for Labour |
2 |
1.18 |
|
Due to Financial Problems |
81 |
47.93 |
|
Total |
169 |
99.99 |
12 Majumder P. Health Impact of Women’s Wage Employment... ; Pathy S. Political Economy of Female Migrant Labour: A Case of Jari Workers in Surat.
Out of the total respondents that is 70.42%; it was found that more than half of the respondents go for work even during ailment. Around 48% of the respondents worked during illness only for financial reasons. It may be said that respondents work in order to run the expenses of their family. If the factory administration provides them financial assistance in case of illness it will increase the overall performance of respondents in the production process. Only 1.18% of the respondents stated that they come to work even during illness because the factory administration demands so.
It can be analysed from the above data that respondents are not conscious about their health because their economic conditions do not allow them to miss their duties and go for check-ups in the hospitals. Due to this reason, they prefer to visit unqualified medical practitioners or visit chemist shops to get immediate relief to be able to work the next day. These medicines may give immediate relief to the worker but in the long run it creates bigger health issues. It can be estimated from their situation that majority of the respondents do work even during serious illness.
Besides the problems like daily hardships, heavy workload, and health issues faced by migrant women workers, it was found that the majority of them, that is 74.17%, were satisfied with their work. In response to this question, respondents narrated that they have no other option except work in precarious conditions. The meaning of satisfaction here for the respondents, is to earn and feed their families. The majority of respondents (74.17%) were satisfied because they were earning and feeding their family. In other words, it can be said that to earn their livelihood was the primary need for rest; it did not matter under what circumstances they worked.
Role of Labour Union. As far as the trade union is concerned, in context to the present study, it was found that there is no trade union or women association that work for the rights of workers in this region. Before 1998, there was a body called, Centre for Indian Trade Unions (CITU), working for the rights of workers but after the series of protests organized by CITU demanding high wage rate for the workers it was banned by factory administration and the members were shown the way out. Consequently, workers could not muster courage after the silencing of the unionization and also their lack of information about the significance of trade unions has also been one of the reasons which discouraged them from forming a new body that could address the rights or demands of workers, especially women workers. R. Jamaly and Wickramanayake also state in their work that generally workers are not aware of trade unions or even if they are aware of it, they are afraid of talking about trade unions [22]. It was also found in the present study that the women who are involved in the trade unions or come forward as leaders or empowered women are always prime targets of supervisors and managers, especially the single women. Industry officials find excuses to target such union members in many ways. This discourages women workers from coming forward and demanding their rights and voicing their concerns despite the presence of their husbands on the same work site.
Discussion and Conclusion. From the above findings, it can be concluded that the female labour force constitutes a huge part of the industrial sector and plays a significant role in the manufacturing and production sector of the Indian economy. However, their working conditions remain difficult, vulnerable and precarious. Due to vulnerability and insecurity and employment in low-paying jobs without adequate
RUSSIAN JOURNAL OF REGIONAL STUDIES. Vol. 32, no. 2. 2024 J^ protection and security at workplaces, migrant women remain socially, economically and medically at risk.
The findings of the study fit well into the six-fold categorization of Shaw’s occupational hazards at workplace13. As it was found that there were cases of injuries at work reported by the migrant women workers at CTM. Only in a few of the serious cases employees were monetarily compensated. Not all employees are provided with the essential protection kits for dealing with the hazardous chemicals and toxins therefore poor health, ailments and sores, fatigue, cramps were majorly reported by the respondents. Hence, biological, physical and Ergonomic hazards were part of the working condition of workers at CTM. Discrimination on the basis of gender, conditions of harassment, physical violence and other workplace hazards to mental, emotional, and physical health were reported by the migrant women workers too. The paper therefore eliminates a certain vacuum of information on the status of women from poor background working in the industrial sector and their specific health and emphasises the need of forming a supportive community for migrant women workers within factory environments, and ensure fair treatment and protection of migrant workers by adopting guidelines of the Interstate Migrant Workers Act.
In the end it may be said that this research exposes the poor implementation of labour laws relating to safety, health and working conditions in India which also places women workers on the margins of social-economic protection and safety. The practical relevance of this article lies in the fact that it points towards the need to implement anti-harassment policies at the workplace in a stringent manner and direct the formal and informal organisations to comply seriously with the guidelines laid by the Government. There is also a need to promote workplace safety measures and provide access to healthcare facilities and health cover to workers. irrespective of the nature of employment. The article would be of great use to policymakers, employers and organisations to take positive measures to make the workplaces more inclusive and safe so as to empower workers who would be able to positively contribute to the global workforce.
References Working conditions and occupational risks of migrant women (CTM textile factory case study)
- Schulte P.A., Pandalai S., Wulsin V., Chun H. Interaction of Occupational and Personal Risk Factors in Workforce Health and Safety. American Journal of Public Health. 2012;102(3):434-448. https://doi.org/10.2105/AJPH.2011.300249
- Nihila M. Growing Industries, Sick Workers: A Study of Leather Tanning Industry of Dindigul from an Occupational Health Perspective. Review of Development and Change. 1999;7(1):134-166. https://doi.org/10.1177/0972266120020104
- Nihila M. Marginalisation of Women Workers: Leather Tanning Industry in Tamil Nadu. Economic and Political Weekly. 1999;34(16/17):21-27. Available at: http://www.jstor.org/stable/4407876 (accessed 26.01.2024).
- Ali R.N., Begum M.M., Salehim K.S., Farid K.S. Livelihood Pattern of Rural Women Garment Workers at Dhaka City. Journal of the Bangladesh Agricultural University. 2008;6(2):449-456. https:// doi.org/10.3329/jbau.v6i2.4846
- Hogh A., Viitasara E. A Systematic Review of Longitudinal Studies of Nonfatal Workplace Violence. European Journal of Work and Organizational Psychology. 2005;14(3):291-313. https://doi. org/10.1080/13594320500162059
- Biswas A., Harbin S., Irvin E., Johnston H., Begum M., Tiong M., et al. Sex and Gender Differences in Occupational Hazard Exposures: A Scoping Review of the Recent Literature. Current Environmental Health Reports. 2021;8(4):267-280. https://doi.org/10.1007/s40572-021-00330-8
- Turrey A.A. Migrant Labour Inflows and Risk-Employment in Kashmir Valley. International Journal of Scientific Research in Multidisciplinary Studies. 2019;5(12):95-101. Available at: https:// www.isroset.org/journal/IJSRMS/full_paper_view.php?paper_id=1660 (accessed 26.01.2024).
- Hasan S.I., Yee A., Rinaldi A., Azham A.A., Mohd Hairi F., Amer Nordin A.S. Prevalence of Common Mental Health Issues among Migrant Workers: A Systematic Review and Meta-Analysis. PLoS One. 2021;16(12). https://doi.org/10.1371/journal.pone.0260221
- Brown G.D. Women Garment Workers Face Huge Inequities in Global Supply Chain Factories Made Worse by COVID-19. New Solutions: A Journal of Environmental and Occupational Health Policy. 2021;31(2):113-124. https://doi.org/10.1177/10482911211011605
- Miles L., Freeman T., Wan Teng, L., Mat Yasin S., Ying K. Empowerment as a Pre-Requisite to Managing and Influencing Health in the Workplace: The Sexual and Reproductive Health Needs of Factory Women Migrant Workers in Malaysia. Economic and Industrial Democracy. 2022;43(4):1676-1698. https://doi.org/10.1177/0143831X211024725
- Gibbs A., Jewkes R., Willan S., et al. Workplace Violence in Bangladesh's Garment Industry. Social Science & Medicine. 2019;235:112383 https://doi.org/10.1016/j.socscimed.2019.112383
- Gannage C.M. The Health and Safety Concerns of Immigrant Women Workers in the Toronto Sportswear Industry. International Journal of Health Services. 1999;29(2):409-429. https://doi. org/10.2190/TFB6-7Q7B-E4DK-X6FL
- Kujuk E. Health Perception and Healthy Lifestyle Behaviors of Female Factory Workers. Archives of Environmental & Occupational Health. 2016;71(4):216-221. https://doi.org/10.1080/1933 8244.2015.1058237
- Ngai P. Made in China: Women Factory Workers in a Global Workplace. Duke University Press; 2005. https://doi.org/10.2307/j.ctv125jkt6
- Moyce S.C., Schenker M. Migrant Workers and their Occupational Health and Safety. Annual Review of Public Health. 2018;(39):351-365. https://doi.org/10.1146/annurev-publhealth-040617-013714
- Verma P., Agarwal S. Workplace Hazard Faced by Vulnerable Migrant Workers Working in the Informal Sector at Lucknow City. Journal of Ecophysiology and Occupational Health. 2021;21(1):46-51. https://doi.org/10.18311/jeoh/2021/26481
- Shams Hirani S., Karmaliani R., McFarlane J., Asad N., Madhani F., Shehzad S., et al. Development of an Economic Skill Building Intervention to Promote Women's Safety and Child Development in Karachi, Pakistan. Issues in Mental Health Nursing. 2010;31(2):82-88. https://doi. org/10.3109/01612840903254859
- Karvadi V, Nair N.S., Manj unatha S. Health Problems Prevailing among the Female Workers in a Garment Factory, Bengaluru. International Journal of Advanced Community Medicine. 2019;2(1):30-40. https://doi.org/10.33545/comed.2019.v2.i1a.08
- Mishra A., Joseph R., Gangadhara M., Lobo R. Body as Machine: Health Vulnerability of Women Garment Factory Workers in India. SSM - Qualitative Research in Health. Volume 2023;4:100301. https://doi.org/10.1016/j.ssmqr.2023.100301
- Lakhani R. Occupational Health of Women Construction Workers in the Unorganised Sector. Journal of Health Management. 2004;6(2):187-200. https://doi.org/10.1177/097206340400600209
- Akhter S., Rutherford S., Chu C. Sufferings in Silence: Violence Against Female Workers in the Ready-Made Garment Industry in Bangladesh: A Qualitative Exploration. Women's Health. 2009;15. https://doi.org/10.1177/1745506519891302
- Jamaly R., Wickramlanayake. Women Workers in the Garment Industry in Dhaka, Bangladesh. Development in Practice: An Oxfam Journal. 1996;6(2):156-161.
