Знания врачей стоматологического профиля: результаты специализации

Автор: Азодо К.Ч., Эхигиатор O., Эхизеле А.О., Ололо О.
Журнал: Саратовский научно-медицинский журнал @ssmj
Рубрика: Стоматология
Статья в выпуске: 1 т.6, 2010 года.
Бесплатный доступ
цель исследования: оценить знания врачей различных стоматологических специальностей и определить, как их предыдущий практический опыт повлиял на уровень знаний. Ординаторы и врачи, работающие в Университете базовой клиники г Бенин, Нигерия, участвовали в анкетировании в 2008 г Всего в анкетировании приняло участие 142 врача, 71% опрошенных ответили на вопросы. Приблизительное соотношение женщин и мужчин: 1:2.5. Указание должностей респондентов: старшие ординаторы - 21.8%, ординаторы - 48.6%, врачи - 29.6%. Отделения, ответившие на вопросы анкеты: медицина внутренних органов - 21.1%; хирургия - 19%; педиатрия - 15.5%; семейная медицина - 11.3%; скорая медицинская помощь - 5.6%; радиология - 4.9%; офтальмология - 8.5%; патология - 5.6%; анестезиология - 5.6%; психическое здоровье - 2.8%. Оценка среднего уровня знаний 10.1±3.3 баллов (максимальное количество =21). Только незначительный процент (5.6%) опрошенных подтвердил хорошие знания (выше 16 баллов), 79.6% респондентов показали удовлетворительные знания (815 баллов), 14.8% ответивших имели плохие знания (менее 8 баллов). Врач, обладающий практикой стоматологического лечения, проявил лучшие знания (Р=0.03). Знания врачей, лично не относящихся к различным областям стоматологии оказались неудовлетворительными. Улучшение знаний врачей стоматологического профиля может быть реализовано с помощью семинаров и других видов образовательных работ
Врач, знания, специализация, специальность, стоматология
Короткий адрес: https://sciup.org/14917030
IDR: 14917030
Medical doctors' Knowledge of dental specialty: implication for referral
The research goal is to assess Medical Doctors' knowledge of the various dental specialties and to determine if their past dental experience affects their level of knowledge. Resident Doctors and Medical Officers working in the University of Benin Teaching Hospital, Nigeria were surveyed with self-administered questionnaire in 2008. A total of 142 doctors responded to the questionnaire, giving a response rate of 71%. The female: male ratio was approximately 1:2.5. The designations of respondents were Senior Registrar 21.8%, Registrar 48.6% and Medical Officers 29.6%. The Departments that returned the questionnaire were Internal Medicine 21.1%, Surgery 19%, Paediatrics 15.5% Family Medicine 11.3%, Accident and Emergency 5.6%, Radiology 4.9%, Ophthalmology 8.5%, Pathology 5.6%, Anaesthesiology 5.6% and Mental Health 2.8% The mean knowledge score was 10.1±3.3. (Maximum score =21). Only a small percentage (5.6%) had a good knowledge (scored above 16), 79.6% had a fair knowledge (scored 8-15) and 14.8% had a very poor knowledge (scored less than 8). Doctor with history of previous dental treatment had better knowledge (P=0.03). The knowledge of Medical Doctors about the various areas in Dentistry is presently not satisfactory. Comprehensive care of patients, which includes prompt and appropriate referral, can be optimized by improvement of Doctors' knowledge of dental specialty through seminars and other educational interventions
Текст научной статьи Знания врачей стоматологического профиля: результаты специализации
1 Dentistry is a profession concerned with the evaluation, diagnosis, prevention, and treatment of diseases, disorders and conditions of the oral cavity, maxillofacial area and the adjacent and associated structures and their impact on the human body [1]. The profession is widely considered necessary for complete oral health and has contributed immensely to the quality of life and well-being of humanity. Historically, Pierre Fauchard can be said to be the founder of modern dentistry because he developed dentistry as an independent profession from medicine [2]. Dentistry is now practiced under different specialties such Dental public health, Endodontics, Oral and Maxillofacial Pathology, Oral and Maxillofacial Radiology, Oral and Maxillofacial Surgery, Oral Medicine, Orthodontics, Periodontics, Pediatric Dentistry and Prosthodontics.
Corresponding author — Dr Clement Chinedu Azodo
Department of Periodontics, New Dental Complex, University of Benin Teaching Hospital
Address: P.M.B. 1111 Ugbowo, Benin City, Edo State, Nigeria 300001. Phone: +2348034051699.
Physicians are known to provide some form of care to patients with dental problems. This may include screening and alleviation of pain but Dentists usually provide the definitive treatment [3]. Universally, the healthcare system encourages patients to be seen first by the physician. It is even more likely in a developing country like Nigeria. It can be predicted that Doctors in almost all the specialties would have come in contact with patients whose primary problem is of dental origin. This was substantiated by the fact that 86.6% of referrals to a Nigerian oral and maxillofacial clinic were sent by general medical practitioners and specialist medical practitioners [4]. A previous study also revealed that about three quarters of physicians in Ilorin, Nigeria, had attended to patients with oral diseases in their practice [5].
In Nigeria, accessibility to dental practice is poorer than medical practice because Dentists are fewer in number and the few available dental practices are unevenly distributed. This limited access to Dentist, ignorance and shortage of oral healthcare facility and manpower make the presentation of orofacial conditions to Medical Doctors in the accident and emergency department and general medical practice common [5]. The fear of the Dentist is also a reason why some patients visit the physicians rather than a Dentist for orofacial problems.
In developed parts of the world where dental awareness is better, patients with dental problems usually present first to the Dentist. A survey in 2001 revealed that only 3.1% of the US population who experienced dental problem reported outside of the traditional dental office which included hospital emergency room setting and other medical settings where approximately 2.7% and 7.0% of them received care respectively [6]. Data from developed countries also recorded the prevalence of dental problems documented in emergency departments and general medical practice in United Kingdom and United States of America as 0.3% to 6.5% [3, 7, 8, 9, 10, 11].
The management of some dental conditions is multidisciplinary in nature. There are cases where a physician is expected to co-manage a patient with a dentist.
MEDICAL DOCTORS’ KNOWLEDGE ABOUT DENT .AL SIT Cl ALT IES
Dear Doctor. please answer the following questions
Gender Mile [ ] Female [ ]
Mantal stalls Single [ ] Mamed [ ]
Medical school ofgraduabon:_________________________________________________
Yearof paduaticm ________________
Status Medical officer ( ] Re pi bar [ ] Senior registrar [ ]
Department:______________________
Hare you ever had dental treatment7 Yes [ ] No [ )
Ins true tioru: please circle your best response on the specific dental specialty that handles items listed The categories of response are Maxillofacial/oral surgery (MS). Oral Medicine (OMI Oral Pathology (OP). Restorabve Dertistry (RD). Prosthetic Dertistry (PD) Penodortics (PEL Orthodontics (OR). Paedodortics (PA)Conemiuty Dentistry (CD)
|
Itenfs) |
MS |
ом |
OR |
Rd |
PD |
FE |
PA |
OR |
CD |
|
1. HIV-related oral lesion like major aptahous ulcer |
MS |
OM |
OP |
RI’ |
PD |
PE |
PA |
OR |
CD |
|
2 Aching tooth that needs lobe retained |
MS |
OM |
OP |
RI' |
PD |
PE |
PA |
OR |
CD |
|
3. Aching tooth that needs removal |
MS |
OM |
OP |
RD |
PD |
PE |
PA |
OR |
CD |
|
4 Wart to bleach teeth |
MS |
OM |
OP |
RD |
PD |
PE |
PA |
OR |
CD |
|
5 Scattered teeth that needs arrangement |
MS |
OM |
OP |
RD |
FD |
PE |
PA |
OR |
CD |
|
6 C hare ng of teeth by dertist |
MS |
OM |
OP |
RI' |
PD |
PE |
PA |
OR |
CD |
|
7. Drag reacbonoral lesion or "off and on”mouthulcen |
MS |
OM |
OP |
RI' |
PD |
PE |
PA |
OR |
CD |
|
8 Hole cn too th but no pain |
MS |
OM |
OP |
RD |
PD |
PE |
PA |
OR |
CD |
|
9 Artificial teetl(dertuie)that needs replacemert or repair |
MS |
OM |
OP |
RI' |
Ft' |
PE |
PA |
OR |
CD |
|
10 C hid with clef) lip and palate |
MS |
OM |
OP |
RI' |
Ft> |
FE |
PA |
OR |
CD |
|
11 Orbital blow out fiacture |
MS |
OM |
OP |
RI' |
Ft' |
FE |
PA |
OR |
CD |
|
12. Fractire of mardiih .maxillaor zygomabcbone |
MS |
OM |
OP |
RI' |
Ft' |
FE |
PA |
OR |
CD |
|
13 Tooth is shaking |
MS |
OM |
OP |
RD |
PD |
PE |
PA |
OR |
CD |
|
14 Milk teeth not yet out and permanert tee thcomug out |
MS |
OM |
OP |
RD |
PD |
FE |
PA |
OR |
CD |
|
15. Needs flounde application to pervert toothdecay |
MS |
OM |
OP |
RI' |
Ft' |
FE |
PA |
OR |
CD |
|
16 Bornwithtooth/teeth in the mouth |
MS |
OM |
OP |
RI' |
PD |
PE |
PA |
OR |
CD |
|
17 Talk about peevertion of oral diseases |
MS |
OM |
OP |
RD |
PD |
FE |
PA |
OR |
CD |
|
18 Oral lesion biopsy specimen |
MS |
OM |
OP |
RD |
PD |
PE |
PA |
OR |
CD |
|
19 Replacement of missing teeth |
MS |
OM |
OP |
RD |
PD |
PE |
PA |
OR |
CD |
|
20 Swollen gum |
MS |
OM |
OP |
RI' |
Ft- |
PE |
PA |
OR |
CD |
|
21 Oral tomeur |
MS |
OM |
OP |
RI' |
PI' |
PE |
PA |
OR |
CD |
Thank you for participating in this study
Fig. 1. Questionnaire used for the stud
Such patients may require medical management for a dental procedure or may have a medical condition that will increase the risk of dental disease [12]. It is therefore surprising that dental problems and issues are not part of medicine and surgery undergraduate curriculum. It means most medical doctors will not receive any formal dental education prior to graduation.
Doctors who trained in Universities where Dentists are also trained are expected to be aware of the scope of dentistry based on their interaction with their dental colleagues. This informal dental orientation may not be so significant as presently in Nigeria, only 7 universities offer Dentistry.
Since the dental awareness is still very poor in Nigeria, it is expected that the Medical Doctors will still come in contact with some dental cases first. It is therefore important that Medical Doctors know the various areas of Dentistry as proper referral to the various dental specialty will eliminate unnecessary delay in the management of the patients and consequently improve the care received at a reduced cost. The knowledge of the dental specialty in the tertiary health sector is expected to have a multiplier effect on the overall management of the patients.
Training may therefore be necessary to correct such deficiencies. The first line of action towards achieving this is to have baseline information for proper formulation of the necessary material. The objective of this study is to assess Medical Doctors’ knowledge of the various Dental specialties and to determine if their past dental experience affects their level of knowledge.
Methods. A descriptive cross sectional survey of all the resident Doctors in the University of Benin Teaching Hospital was done using a pre-tested, self administered 23-item questionnaire. The questionnaire was divided into two sections; Section 1 was on demographic variable and history of previous dental treatment. Section 2 elicited knowledge of the Doctors on areas of dentistry where certain oral and dental conditions should be referred to using 21 questions (Figure 1) . Correct answers were scored 1 point while wrong answers or no response were scored zero. A score less than 8 points was rated poor knowledge, 8-15 points fair knowledge and 15 points and above rated good knowledge. Informed consent was obtained from all the 32 participants before the study. Ethical approval was obtained from University of Benin Teaching Hospital ethics committee. Data analysis was done with SPSS version 15.0. The results were presented using pie charts and a bar chart
Results. A total of 142 doctors responded to the questionnaire, giving a response rate of 71%. The female: male ratio was approximately 1:2.5. The designations of respondents were Senior Registrar 21.8%, Registrar 48.6% and Medical Officers 29.6%. Majority of the respondents (83.1%) attended universities training Dentists. The respondents were from Internal Medicine 21.1%, Surgery 19%, Paediatrics 15.5% Family Medicine 11.3%, Accident and Emergency 5.6%, Radiology 4.9%, Ophthalmology 8.5%, Pathology 5.6%, Anaesthesiology 5.6% and Mental Health 2.8% (Figure 2) . A total of 77 (54.2%) had received dental treatment as at the time of this study while 65(45.8%) had not had any dental treatment. The mean knowledge score was 10.1±3.3. (Maximum score =21). Only a small percentage (5.6%) had a good knowledge (scored above 16), 79.6% had a fair knowledge (scored 8-15) and 14.8% had a very poor knowledge (scored less than 8) (Figure 3) . Doctor with history of previous dental treatment had better knowledge (P=0.03). The knowledge of the various den-
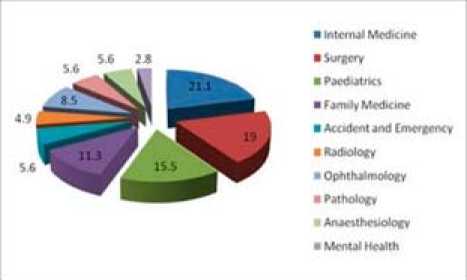
Fig. 2. Department of the respondents
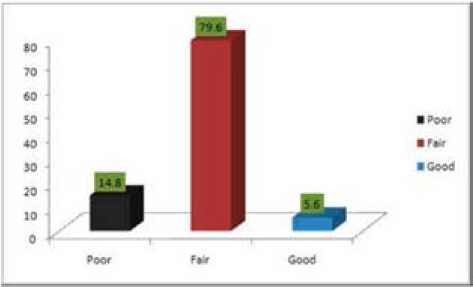
Fig. 3. Knowledge of dental specialty among respondents
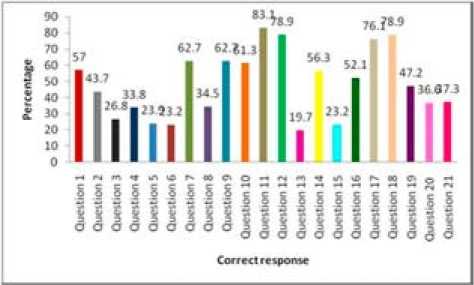
Fig. 4. Percentage of correct response on referral dental specialty tal specialties was not affected by the department, years of experience and medical school of graduation.
Question 11 was the most correctly answered by 83.1% of the respondents. The second most correctly answered were question 12 and question 18 (78.9%). Question 17 was the fourth most correctly answered (76.1%). Question 4 was answered correctly by about one-third (33.8%) of the respondents. Question 13 was least correctly answered by 19.7% of the respondents (Figure 4) . The questions are outlined questionnaire used for the study.
Discussion. This study revealed that that only a small percentage of the Medical Doctors have a good knowledge of dental specialties. This may be because Dentistry is not part of the Nigerian Medical school curriculum. Majority of the respondents had a fair knowledge though and this may be due to the fact that some Doctors may have received some education on the management of dental conditions from revision courses, journals, conferences, workshops and the internet. In the United Kingdom, a survey revealed that only 11 of the 21 medical schools studied had Oral pathology in their curricula [13]. It is therefore not surprising that serious deficiencies in diagnostic awareness of oral diseases have been reported on medical students and Doctors in the UK [13]. In dentistry, an early diagnosis or a prompt and appropriate referral are important objectives as this will improve outcome and reduce the morbidity of treatment in cases. It will also save the patient the agony of going back and forth the healthcare facility, ensure early return of health, improve satisfaction, improve quality of life and ultimately reduce cost. The level of knowledge depicted in this study may result in prolongation of time before patients come in contact with the right dental specialty thereby denying them the opportunity of reaping the benefits of optimal, effective and timely oral care.
Respondents with previous dental treatment experience had higher score in the level of knowledge (P<0.05). The dental visit usually involves proper history taking, extensive examination of all the orofacial structures and radiographic investigations before a diagnosis can be made and the patients referred to the relevant department for definitive management. A medical Doctor who has passed through this routine will probably be better informed about the management of dental cases.
The respondents’ primary department and status was not significantly associated with the level of knowledge in this study. This is surprising because some residents rotate through some departments in dentistry as part of their clinical postgraduate training. Residents in Ophthalmology and Otorhinolaryngology undertake posting in Oral and Maxillofacial surgery while residents in Community health undertake posting in community dental health during.
The well established nature of Oral and maxillofacial surgery, with multidisciplinary consultation, may be the possible reason why a reasonable number of respondents knew cases that should be referred to this specialty. Many respondents on the other hand did not know where to refer patients to for preventive measures and some cosmetic procedures.
A limitation of the study is that questionnaire could not be retrieved from residents in the department of Obstetrics and Gynaecology which constitute one of large number of resident in the studied hospital. Also the find- ings from this study could not be compared with other studies since not much has been done in this area.
Conclusion. This study revealed that doctors’ knowledge of dental specialty in this study was deficient and need to be improved through seminars and other educational interventions. Standard written advice sheets for referral for common dental problems for patients would also be useful. This will ensure that the comprehensive care of dental patients which includes prompt and appropriate referral to dental specialist by Doctors is at its optimal level.
Список литературы Знания врачей стоматологического профиля: результаты специализации
- Dentistry Definitions, hosted on the American Dental Association website. Page accessed 11 December 2007. This definition was adopted the association's House of Delegates in 1997.
- Bird DL, Robison DE. History of Dentistry
- In Chapter 1 Modern Dental Assisting 8th Edition. Elsevier 2006. p 1-38.
- Pennycook A, Makower R, Brewer A, Moulton C, Crawford R. The management of dental problems presenting to an accident and emergency department. J R Soc Med. 1993. 86:702-703.
- Obuekwe ON, Ojo MA, Odai C. Characteristics of referrals to an Oral and Maxillofacial surgery clinic. Annals of Biomedical Science 2002. 1(1): 38-44.
- Sa'adu ZO, Abdulraheem IS. Oral health care practice and socio-demographic findings among the physicians in Ilorin, Nigeria. Niger J Med. 2003. 12(4):211-6.
- Cohen LA, Manski RJ. Visits to non-dentist health care providers for dental problems. Fam Med 2006. 38(8):556-64.
- Haughney MG, Devennie JC, Macpherson LM, Mason DK. Integration of primary care dental and medical services: a three-year study. Br Dent J. 1998. 184(7):343-7.
- Anderson R, Richmond S, Thomas DW. Patient presentation at medical practices with dental problems: an analysis of the 1996 General Practice Morbidity Database for Wales. Br Dent J. 1999. 186:297-300.
- Lockhart PB, Mason DK, Konen JC, Kent ML, Gibson J. Prevalence and nature of orofacial and dental problems in family medicine. Arch Fam Med. 2000. 9(10):1009-12.
- Burt CW, Schappert SM. Ambulatory care visits to physician offices, hospital outpatient departments, and emergency departments: United States, 1999-2000. Vital Health Stat 13. 2004. (157):1-70.
- Robertson J. Oral Problems in Medical Practice. Glasgow, Scotland: Glasgow Dental Hospital. Dissertation 1989.
- Clark MM, Album MM, Lloyd RW. Medical care of the dental patient. Am Fam Physician. 1995. 52(4):1126-32.
- McCann PJ, Sweeney MP, Gibson J, Bagg J. Training in oral disease, diagnosis and treatment for medical students and doctors in the United Kingdom. Br J Oral Maxillofac Surg. 2005.43(1):61-4.
