A case of surgical extraction of the lower third molars in a cranial series from the Pucar'a de Tilcara fortress (Jujuy province, Argentina)
")
Author: Zubova A.V., Dmitrenko L.M., Pikhur O.L., Obodovskiy A.V., Bessonov V.B., Malyutina A.A., Chugunova K.S., Pozdnyakov D.V.
Journal: Archaeology, Ethnology & Anthropology of Eurasia @journal-aeae-en
Section: Anthropology and paleogenetics
Article in issue: 2 т.48, 2020.
Free access
Short address: https://sciup.org/145145487
IDR: 145145487 | DOI: 10.17746/1563-0110.2020.48.2.149-156
Text of the review article A case of surgical extraction of the lower third molars in a cranial series from the Pucar'a de Tilcara fortress (Jujuy province, Argentina)
Therapeutic tooth extraction is one of the most widespread surgical operations. Today, it is carried out for numerous indications: pericornitis, periostitis, periodontitis, chronic periodontitis and its exacerbations, abnormal position of the third molars in the dental arch, tumors, etc. (Iordanishvili et al., 2016; Steed, 2014).
First cases of deliberate tooth extraction were presumably detected in specimens from Ancient Egypt (Forshaw, 2009: 482), but no data have existed so far on the prevalence of such surgeries in the preHispanic population of the New World. However, it is well established that ancient civilizations of South America possessed medical knowledge fairly well developed for their times, and were capable of carrying out complex surgeries (Marino, Gonzales-Portillo, 2000; Ortiz, Torres Pino, Orellana González, 2016); despite this, the bioarchaeological studies describing the dental practices of the Inca do not provide any evidence of therapeutic extractions of molars. Concurrently, ritual ante-mortem tooth modifications were widespread (Romero, 1970; Ubelaker, 1977, 1987). Only two reliable cases of therapeutic manipulations with teeth have been described so far. Both were identified in specimens from Cusco (ancient capital of the Inca in Peru) and represent manifestations of drilling of the upper canines, likely carried out for curing carious lesions (Ortiz, Torres Pino, Orellana González, 2016).
This study describes the clear signs of a deliberate surgical extraction of the third molars detected during studying the cranial sample from the Pucará de Tilcara fortress in northwestern Argentina. This site was a fortified settlement of the Omaguaca Indians in the central part of the Quebrada de Humahuaca valley, close to the confluence of the Río Huasamayo and Río Grande rivers. The settlement emerged in the 8th century AD as an agglomeration of several smaller villages (Handbook…, 2008: 587). Eventually, it grew into a fortified site covering an area of 17.5 ha, with an average population of slightly over 1600 (Zaburlín, 2010: 197). The city reached its peak in the 11th to 14th centuries AD, when the citadel was one of the main centers of the Inca Empire in its Argentine territory (Greco, Otero, 2015). In 1536, the city was captured by Spanish conquistadors and ceased to exist.
The ruins of Pucará de Tilcara were discovered in the early 20th century by an Argentine archaeologist J.B. Ambrosetti (Zaburlín, Otero, 2014). According to modern researching, bases of stone walls of 588
residential buildings were found there. In some cases, open spaces (likely patios) were observed adjacent to the buildings (Otero, 2013: Fig. 1). Three necropolises were detected near the fortress: on the southern, eastern, and western sides. Burials were often found inside the patios as well. In such cases, the burials were located in corners, or near the walls, and separated by semicircular stone enclosures (Debenedetti, 1930: 47, 52–53). The interments were both single and communal (up to eight individuals), with the deceased buried in a supine or in a flexed position on their sides. The stone enclosures were circular or semicircular, and numerous grave goods were put into the graves: ceramic vessels of various shapes, and wooden, bone, horn or copper items.
The first excavations at the site began in 1908 and went on for three field seasons. In 1908–1910, J.B. Ambrosetti and his student S. Debenedetti excavated a small area in the northwestern part of the site. This part was inhabited in the late period of site’s existence, after its conquest by the Incas (late 15th to 16th centuries) (Zaburlín, Otero, 2014: 212). In 1910, an anthropological collection including 20 artificially deformed skulls, as well as 147 archaeological artifacts from those burials, was purchased by the MAE RAS via an exchange with the Ethnographic Museum of Buenos Aires (Dmitrenko, 2016).
The paleopathological study of this collection, which revealed the case of mandibular surgery described below, started in 2018. This paper discusses the medical diagnosis that was the reason for the extraction of the lower third molars of one of inhabitants of Pucará de Tilcara. We outline the technique of performing the surgery, and its possible outcomes.
Material and methods
The lesions suggesting a surgical extraction of the lower third molars were detected in the mandible of individual No. 5148-9—a man, about 40 years of age (Fig. 1). The age-at-death was determined by the degree of exo- and endocranial suture obliteration, taking into account the possible disruption of the order and rate of obliteration due to the artificial cranial deformation (Gerszten, 1993). Dental wear and the condition of the temporomandibular joint were also taken into account. The sex of the individual was determined by the dimorphic features of the occipital bone, browridge, supraorbital area, mastoid process, and mandible (Alekseev, Debets, 1964: 29–40; Standards…, 1994: 16–21).
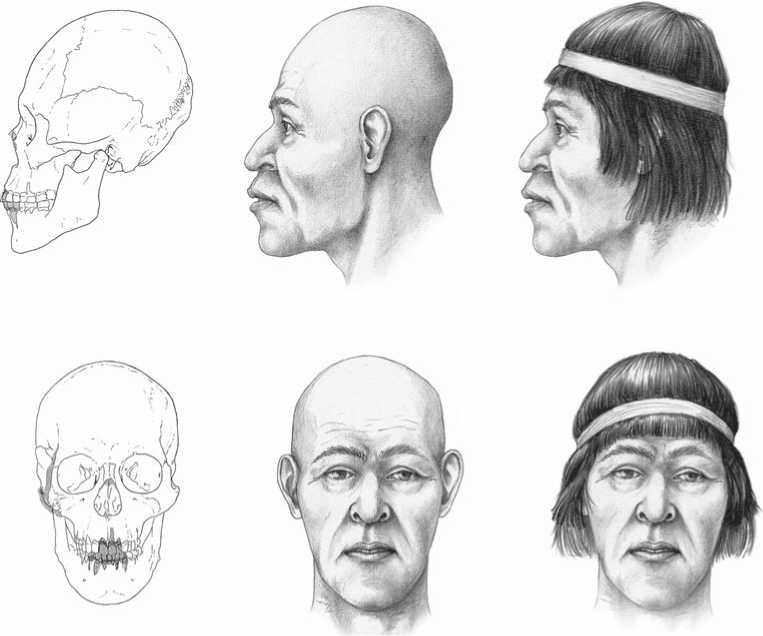
Fig. 1. Skull (missing parts are labeled in gray) and facial reconstruction of the individual.
The skull is well preserved, with only small postmortem damage: the right zygomatic arch is absent, and the nasal bones are broken at the lower margin (Fig. 1). The mandible was originally broken into two parts, but then reconstructed. The lower incisors, canines, and first premolars, as well as both the upper central and second left upper incisors, were lost during the archaeologization process.
Cut-marks and other wounds related to the extraction of the third molars were detected in the mandible. In order to reconstruct the sequence of manipulations by the surgeon in the course of the operation, the lesions were investigated at the Experimental Traceological Laboratory of the Institute of History of Material Culture of the Russian Academy of Sciences, using a binocular microscope MBS-9 (oblique illumination, magnification up to ×98). Canon EOS Utility software was used for multifocal photofixation of the wounds, while Helicon Focus 5.2. was employed for drawing the resulting image.
A number of analyses were carried out at the Department of Scientific and Technical Examination of Works of Art of the State Hermitage Museum, in order to identify the material of the tool used for extracting the molars: optical microscopic examination of the alveolar surface, scanning electron microscopy (SEM), X-ray fluorescence analysis, and X-ray microanalysis. Leica M60 and Zeiss Stemi 508 microscopes were used for the optical microscopic examination, while the SEM study was carried out using the scanning electronic microscope Zeiss EVO-MA-25, with the following settings: U = 20 kV, WD = 30 to 401 mm, and low vacuum for non-conducting samples. μXRF-spectrometer ArtTAX (RÖNTEC, Bruker) was used for the X-ray fluorescence analysis, applying the following protocol: U = 50 kV, I = 700 μA, texp – 40 s, material of the anode of X-ray tube – molybdenum. The X-ray microanalysis was carried out with Oxford Instruments X-MaxN 80 SEM-EDX-analyzer.
The individual’s dentition was visually examined following the existing protocols (Aufderheide, Rodríguez-Martín, Langsjoen, 1998; Ortner, Putschar, 1985), in order to diagnose the pathology that was the indication for the surgery. The mandible was CT scanned using the experimental scanner MRCT-04, constructed at the St. Petersburg Electrotechnical University (“LETI”), applying the following protocol: tube voltage – 140 kV, amperage – 50 mA, no filter, slice thickness – 0.1 mm. The images were processed with the experimental software developed at “LETI”. Both multiplanar (MPR) and volume (VR) modes of reconstruction were employed.
Results and discussion
Reconstruction of the surgery. Manifestations of deliberate tooth extraction were detected at both the third molar sockets. A straight section made in order to remove a piece of bone was observed at the vestibular side of the upper margin of the left socket (Fig. 2). The shape and length of the section cannot be completely reconstructed owing to its obliteration during the regenerative process. The depth of bone removal was not more than 1.5 mm, though the alveolar wall at the lingual side was absent up to 5–7 mm from the margin. However, owing to bone remodeling it is impossible to determine if this part of the alveolar wall was cut off intentionally, or casually damaged, during the extraction. Intensive formation of new bone is observed at the margins of the socket, and the socket itself is filled with cancellous bone. This suggests that the tooth was extracted at least two or three months before the individual’s death.
As manifestations of healing were absent in the socket of the right third molar, it was possible to reconstruct the surgery’s procedures in detail. No signs of preliminary marking of the wound’s contour were detected. The initial penetration of the tool into bone occurred near the disto-vestibular corner of the second molar. This is evident from the presence of an indentation caused by a contact with the tip of the tool, which was oriented perpendicular or slightly obliquely to the bone surface. The socket was surgically expanded in the vestibular direction, for about 4 mm in its mesial part and for 5 mm in the distal part, via removal of a part of the mandible. The macro- and microscopic analyses of the bone’s surface revealed the presence of a section with sharp edges. The cut was made from the mesio-vestibular angle of the socket in the vestibular direction, then toward the ramus and afterwards in the lingual direction till the center of the distal wall of the socket (Fig. 3). After the contour was cut through, bone and soft tissue were removed or scraped out via semicircular incisions, which left short grooves on the internal surface of the vestibular wall of the socket (Fig. 4). The optimal position for making possible such a sequence of cuts is for the patient to rest on his left side with his back turned to the surgeon. When about 1 cm of bone was removed, the tooth was extracted.
Operating tools. In the period that the skulls from the MAE collection belong to, the people from the Quebrada de Humahuaca valley already adopted from the Inca the skills necessary for carrying out fairly difficult surgical operations, such as trepanations, dissection of suppurations, sections for removing snake poison from wounds, etc. (Handbook…, 1946: 55– 56, 637–638). The surgical tools used by the studied population were basically similar to those found in other Inca archaeological assemblages. Metal knives (“tumi”), used for scalping in ritual or for medical purposes, were excavated at archaeological sites of that time in northwestern Argentina (Omaguaca, Calchaquí). Obsidian knives (“escapelos” or “pedernales”) were employed for cutting skin and bone as well (Marino, Gonzales-Portillo, 2000: 947–948).
The size of the surgical perforation and the length of the cut marks suggest that all manipulations during the operation might have been performed by a narrow cutting tool with the blade’s working edge of no longer

0 1 cm
Fig. 2. External view of the alveolus of the lower left third molar, displaying surgical cut marks.
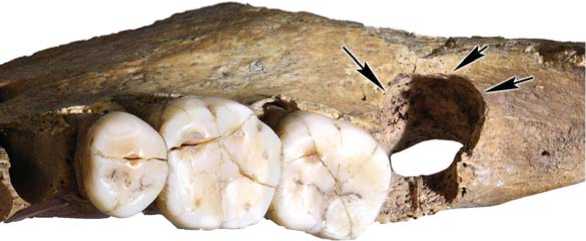
0 1 cm
Fig. 3. Cut marks on the alveolar walls of the lower right third molar.
than 4–5 mm. In archaeological collections from Tilcara stored at MAE RAS, only two types of artifacts correspond to these characteristics: copper plates and obsidian tools (Fig. 5), similar in terms of shape and size to some instruments utilized by Inca surgeons (Ibid.: Fig. 17).
The use of the obsidian tools seems more probable, judging by the results of the optical and electron microscopy, X-ray fluorescence analysis and X-ray microanalysis, which have not detected traces of ancient metal on the surfaces available for observation. Notably, the complex shape of the mandible and the depth of the alveola have obstructed access to the area where traces of the surgical tool could be found. The area could not be reached without destruction of the specimen: the desired signal got partially interfered or/and scattered, and it might be deformed. Therefore, the apparent absence of traces of metal should be interpreted with caution. Nevertheless, the hypothesis that the surgery was carried out using a stone tool remains reasonable, taking into account the fact that traces of modern medical instruments used for the cleaning and probing of a traumatic defect are clearly discernible at the margins and internal surface of the tooth’s socket. These traces are particles of nickel-clad steel, which are visible on back-scattered electron images owing to their contrasting white coloration.
Indications for the surgery. A general assessment of the individual’s dentition was carried out in order to determine what pathological process was the indication for the surgery and what was the cause of his death. The upper dental arch is elongated, with a narrowing in the anterior part; the lower dental arch is U-shaped. Despite the ante-mortem loss of teeth, it was possible to reconstruct that the individual had an open bite: the upper incisors and canines were strongly protruding anteriorly and did not occlude the lower teeth. The molars and premolars of the maxilla and mandible display normal occlusal contact. The upper third molars were formed normally and erupted. The position of the lower third molar sockets and the contact facets on the distal interproximal surfaces of the crowns of adjacent molars demonstrate that the lower third molars formed normally as well, erupted in term, and were functional during the individual’s life. Thus, abnormal eruption as a possible cause of the operation can be excluded.
None of the surviving teeth of the individual exhibit signs of large carious lesions or complications— pulpitis or periodontitis. But manifestations of the initial stages of caries are observed in the central fovea of the occlusal surface of the upper third molars. The lower third molars are absent, but theoretically
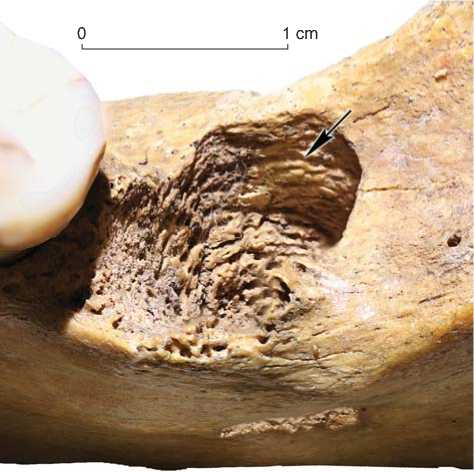
Fig. 4. Traces of scraping on the vestibular wall of the socket of the right third molar.
А
1 cm
Fig. 5. Obsidian tools from the Pucará de Tilcara fortress. A – MAE, No. 1800-129 (16); B – MAE, No. 1800-129 (27); C – MAE, No. 1800-129 (28).
they might have had medium or deep carious lesions. A carbohydrate-rich diet, an absence of due mouth hygiene, and anatomical peculiarities in the position of the third molars are the risk factors of caries for these teeth and their antagonists.
Most teeth of both jaws display small deposits of calculus, mainly localized in the interdental space.
Nevertheless, the individual likely suffered from a disruption of the normal balance of microflora of the oral cavity, because the signs of chronic generalized periodontal disease (I–II degrees) are evident. The roots of all teeth protrude from their alveoli for 1.5– 2.5 mm, the palatal bones are markedly porous. The alveolar septi between the upper first and second molars display manifestations of inflammation. These were also observed around the lower second molars. This observation suggests that an influence of adverse environmental conditions (hypothermia, infection, trauma, psychological stress, etc.) on the individual might have triggered a decrease of immunity and exacerbation of chronic periodontitis.
CT scanning of the mandible has shown that the socket of the left third molar was widened and inflamed in its root part. Resorption of the bottom of the alveolus is observed in the apical area, which also suggests that periodontal disease was progressing. This might have been a complication of caries, which developed into chronic pulpitis, and accompanied by a penetration of infection inside the mandible in the tooth’s root area during the exacerbation. This pathological process was progressing in a background of chronic periodontal disease. Importantly, general status of body defense potential always plays an important role in pathology development, and this potential was likely decreased. In the CT scan of the mandible, traces of a fistulous canal, passing from the bottom of the socket into the body of the mandible, are visible (Fig. 6). The process could have lasted chronically for a while, but at some point it developed a complication accompanied by strong pain and soft tissue swelling. This complication was probably the reason for the surgical intervention, and the tooth was extracted before the infection spread along the mandibular canal and mandibular body. The operation was performed successfully, as no signs of inflammation that might suggest wound infection or post-operative complications are observed.
The picture observed on the right side of the mandible is not as benign. Porosity, which might be a result of inflammation, is observed on the internal surfaces of the socket of the third molar that were not scraped. The development of chronic periodontitis in the third molars began in a background of chronic generalized periodontal disease from both sides simultaneously. These pathological manifestations (pain, swelling) were more pronounced on the left side, and the left molar was extracted earlier. But on the right side, the pathology was progressing for several more months, thus leading to more severe changes. As it can be seen in the CT scan, the exacerbation of chronic periodontitis of the right third molar has led to strong inflammation. The alveolar walls do not display traces of resorption, and signs of inflammation were only detected in its apical part, in the form of cystogranuloma. This led to bone resorption of the bottom of the socket, and to the development of destructive odontogenic osteomyelitis of the mandible. This diagnosis is confirmed by the sequestra around the roots of the right lower molars, visible in the CT scan. The sequestra reach the mandibular canal (Fig. 7).
An outlet of the fistulous canal, 7.75 mm in diameter, surrounded by inflammatory lesions, is located on the internal surface of the mandibular body, near the apex of the root of the right third molar. Together with the presence of a sequestrum between the alveola and mandibular canal, this suggests that infection has spread far beyond its initial locus. It intruded the blood’s circulatory system and the soft tissues of the
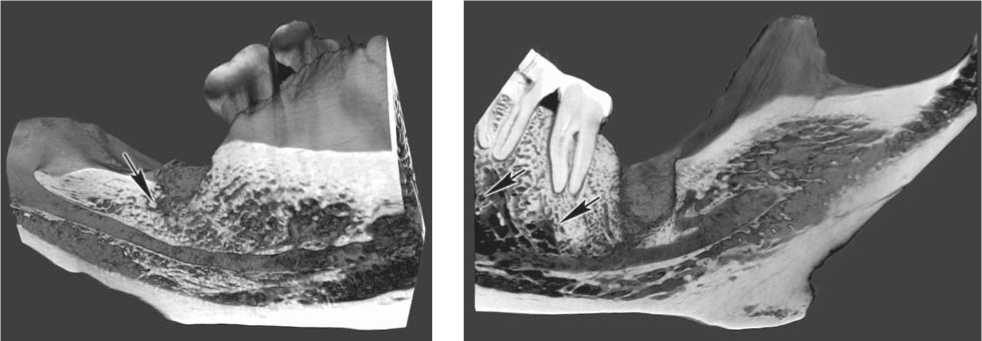
Fig. 6. Resorption of the bottom of the socket of the left third molar.
Fig. 7. Sequestra around the roots of the right lower molars.
face, which likely led to the formation of a phlegmon or an abscess. Possible clinical manifestations of the disease include high body temperature, chills, general weakness, pain, swelling and redness of the soft tissues of the right side of the face, the formation of fistulas with purulent exudate, and contracture of the masticatory muscles (difficulty opening the mouth). In order to release the patient from these symptoms, the molar was removed. But the surgery was carried out too late, which led to irreparable traumatic changes, and the operation did not have the proper therapeutic effect. As is evident from the absence of signs of healing both in the operating field and in the outlet of the fistulous canal, the clinical case was fatal.
Conclusions
Our analysis of the surgical manipulations carried out on the individual from the Pucará de Tilcara fortress has once again shown the high level of medical knowledge of surgeons in the Inca Empire. The individual died after the second operation, but the quality of the surgical interventions was high. The access to the lower third molars was difficult and partially obstructed by the mandibular ramus. Despite this, the surgeon was able to avoid such complications as fractures of the alveolar wall and mandibular body or injury to the temporomandibular joint. The risk of such trauma is high even at present (Deliverska, Petkova, 2016).
As often happens today, an exacerbation of chronic periodontal disease was the indication for a surgical intervention. The teeth were extracted in two stages, as the surgeon likely considered the need for a recovery period after the first operation, in order to make the outcome of the second operation positive. One of the two teeth was extracted successfully without complications. However, despite a highly developed (by the standards of the time) system of medical knowledge available for ancient South American doctors, their surgical skills likely outpaced the diagnostic capabilities. The cause of death of the individual was too long a period between the two operations. This delay was probably a result of underestimation of the degree of severity of the pathological process complicated by osteomyelitis, and of the absence of effective disinfecting pharmacological agents. Some authors suggest that, at least in ancient Peru, Inca healers were aware of the nature of some infectious diseases, and were widely using medicinal plants in their practices (Marino, Gonzales-Portillo, 2000). But either the effectiveness of the known antimicrobial substances was insufficient to heal complicated purulent odontogenic inflammations, or the healers from Pucará de Tilcara were unaware of such agents and could not have provided the patient timely treatment.
Acknowledgement
This study was supported by the Russian Foundation for Basic Research, Projects No. 18-00-00360 (18-00-00511, 18-0000350) COMFR.
