A case report of early detection of rare femoral shaft bone metastasis in a penis cancer patient

Author: Ajay K.Ya., Sandip K.M., Suman G., Ganga D.A., Nitu Sh., Pandey Sh.K., Dhakal D., Anil P.
Journal: Сибирский онкологический журнал @siboncoj
Section: Случай из клинической практики
Article in issue: 5 т.22, 2023.
Free access
Background. Bone metastasis is very common in the advanced stage of numerous carcinomas. In penile carcinoma, lymph nodes metastasis is somehow common but it is very rare reported to be secondary from penile cancer. Till the date, there are only few cases of penis carcinoma reported bone metastasis in literature worldwide. Case Presentation. Herein, We presented a 51-year-old Nepalese male with squamous cell carcinoma of penis. Computed Tomography (CT) scan of the patient revealed that there was carcinoma involving glans penis and precure with bilateral external & internal inguinal Lymphadenopathies. After then, the patient was under gone for partial penectomy and bilateral inguinal lymphadenectomy and complete 6-cycle chemotherapy. After one year of treatment, patient developed thigh pain and headache and he advised to have Magnetic Resonance Imaging (MRI) of brain, 99mTc-MDP whole body bone scan and CT scan of Pelvis and Thigh. The examination report reveals that there was a sclerotic change in vertex of skull bone and moderate 99mTc-MDP uptake in right proximal shaft of femur just below the neck D/D metastasis. The histopathological examination of the true cut biopsy taken from the lesion of the femur showed metastatic keratinizing squamous cell carcinoma which is rare case of femoral shaft bone metastasis secondary from penile carcinoma. Then patient was sent for surgical reconstruction of femur. Based on the case studies review femur shaft bone metastasis from penile cancer is extremely rare.
Skeletal metastasis, penis cancer, femoral shaft, comprehensive management
Short address: https://sciup.org/140302490
IDR: 140302490 | UDC: 616.66-006.6-033.2:611.718.4 | DOI: 10.21294/1814-4861-2023-22-5-173-179
Случай раннего выявления метастазов в бедренной кости у больного раком полового члена
Метастазы в кости часто встречаются на поздних стадиях разных злокачественных новообразований. Для рака полового члена характерно лимфогенное метастазирование, костные метастазы встречаются очень редко. На данный момент в мировой литературе зарегистрировано лишь несколько случаев рака полового члена с метастазами в кости. Описание клинического случая. Мы представляем описание клинического случая плоскоклеточного рака полового члена у 51-летнего мужчины из Непала. Компьютерная томография (КТ) выявила рак полового члена, локализованный на головке и крайней плоти с двусторонней паховой лимфаденопатией. Пациенту выполнена частичная пенэктомия, двусторонняя паховая лимфаденэктомия, проведено 6 курсов адъювантной химиотерапии. Через один год после завершения лечения у пациента появились боли в бедре и головная боль, рекомендована МРТ головного мозга, сканирование костей скелета с 99mTc-MDP и КТ таза и бедра. Обследование показало наличие склеротических изменений в теменной кости черепа и умеренное накопление 99mTc-MDP в проксимальном отделе правом бедренной кости ниже шейки. Гистологическое исследование биоптата, взятого из очага в бедренной кости, выявило метастаз ороговевающего плоскоклеточного рака, что является редким случаем метастазирования рака полового члена в диафиз бедренной кости. Пациент был направлен на хирургическую реконструкцию бедренной кости. Согласно обзору клинических исследований, метастазы в диафизе бедренной кости при раке полового члена встречаются крайне редко.
Text of the scientific article A case report of early detection of rare femoral shaft bone metastasis in a penis cancer patient
Background
Bone metastasis might be secondary from numerous sorts of cancers. On the opposite hand, penis cancer could be a fairly uncommon and localized malignancy. It always spreads via lymphatic routes, and hematogenous dissemination seldom occurs even within the advanced stage because of the natural barrier functions of Buck’s fascia [1]. Metastatic bone disease secondary from penile carcinoma is extremely rare, with only few cases reported in literature worldwide thus far. Based on the case study and more importantly, the literature review, both skull vertex and femur shaft bone metastasis from penile cancer is extremely rare, to the best of our knowledge; this is the first report of a patient with penile cancer spread to the femur as well as skull bone from primary squamous cell carcinoma of the penis.
Case Presentation
Penile cancer usually occurs in the sixth decades of life, with SCC representing the most common pathological type. Penile cancer usually occurs in the sixth decades of life, with SCC representing the most common pathological type. For the diagnosis of metastatic bone disease, serological examinations are usually of low efficiency. Although hyper-calcemia is often presumed to be associated with bone metastasis because of osteolysis, it may be a hallmark of paraneoplastic syndrome but not of skeletal metastasis in penile cancer [2]. In most of these cases, the diagnosis was made through imaging and histopathological examinations. Of the 10 cases, histological biopsy of the metastatic foci was performed in 5 cases, including the present case. The results of biopsy are mostly well-differentiated SCC, and consistent with final pathological results.
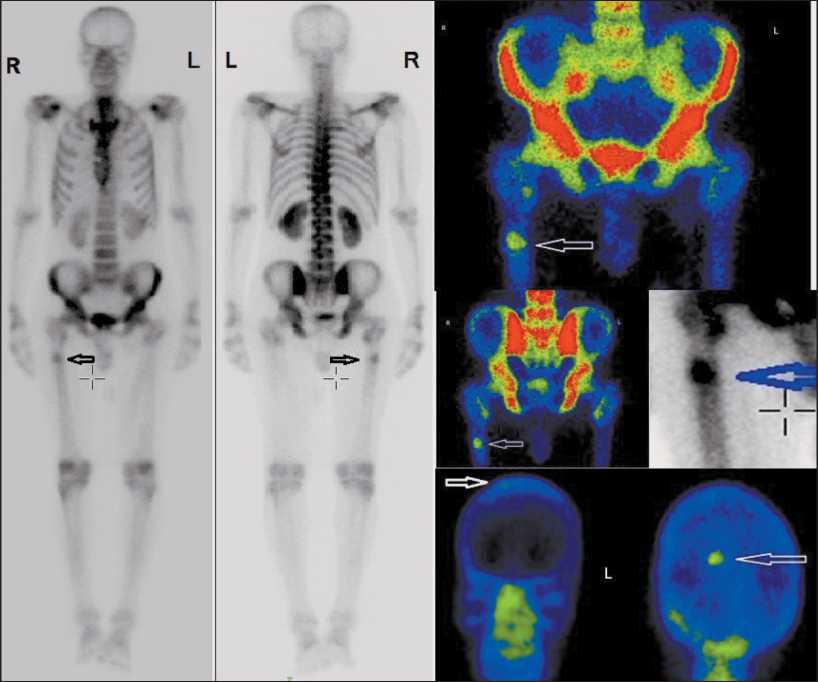
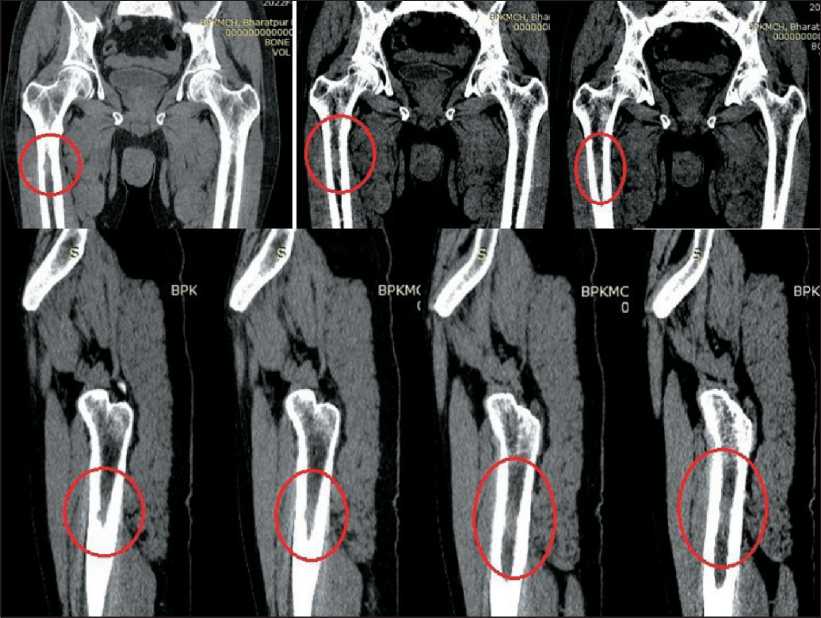
Fig. 1. There is moderate 99mTc-MDP uptake in right proximal shaft of femur just below the neck and vertex of skull in 99mTc-MDP whole body scan and static images of their respective. Note: created by the authors
Рис. 1. При сканировании всего тела с 99mTc-MDP наблюдается умеренное накопление радиофармпрепарата в проксимальной части правой бедренной кости ниже шейки, а также в теменной области черепа. Примечание: снимок выполнен авторами
Рис. 2. КТ таза и бедра. Метастатическое поражение проксимального отдела правой бедренной кости ниже шейки, двусторонние метастазы в паховых лимфатических узлах. Примечание: снимок выполнен авторами
Plain and Gadolinium contrast media enhanced MRI brain scan was performed. T1-TSE-Tra, T2-TSE-
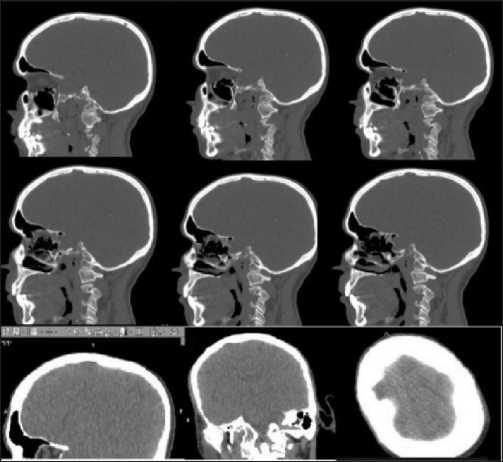
Fig. 3. There is sclerotic changes like lesion on vertex of skull bone of CT scan of brain. Note: created by the authors Рис. 3. КТ головного мозга и костей черепа. Склеротические изменения в теменной кости. Примечание: снимок выполнен авторами
Tra, T2-FLAIR-Tra, T1-TSE-Cor, T2-TSE-Sag, DWI-epi3trace-Tra, Contrast Enhanced T1-TSE-Tra and Contrast Enhanced T1-TSE-Cor series were performed. MRI scan concluded there was a sclerotic change like lesion on the vertex of skull bone (Fig. 4).
After that a histopathological examination of the true cut biopsy taken from the lesion of the femur showed metastatic keratinizing squamous cell carcinoma and patient sent for orthopedic surgery department for further treatment and follow up.
After that, the patient was undergone for surgery. Normally, in long bone shaft metastasis, an intramedullary rod has been placed down the center of the femur. The goals of bone stabilization in the lower extremity include preventing a pathologic fracture, relieving pain, and improving mobility and quality of life. But in our case, total proximal femur replaced to prevent the chance of new metastases in head and neck of femur and to decrease the chance of any other fracture. After 6 month of surgery, the patient felt better in walking and had a radiograph which is shown in Fig. 5.

Fig. 4. There is sclerotic changes like lesion on vertex of skull bone of MRI scan of brain. Note: created by the authors
Рис. 4. МРТ головного мозга и костей черепа. Склеротические изменения в теменной кости.
Примечание: снимок выполнен авторами
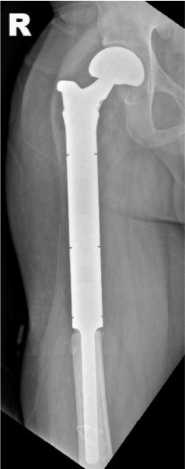
Fig. 5. Radiograph of post right proximal femur replacement of patient.
Note: created by the authors
Рис. 5. Рентгенограмма проксимального отдела правой бедренной кости после протезирования.
Примечание: снимок выполнен авторами
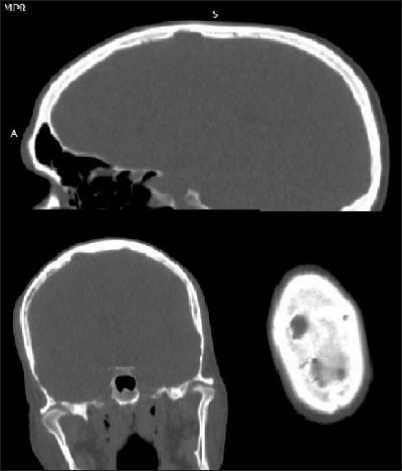
Fig. 6. There is sclerotic changes like lesion on vertex of skull bone of CT scan of brain. Note: created by the authors Рис. 6. Контрольная КТ головного мозга и костей черепа. Склеротические изменения в теменной кости.
Примечание: снимок выполнен авторами
The patient was also undergone for CT scan of brain to evaluate the sclerotic changes in brain bone which was seen 6 months before. There was nothing changes in sclerotic lesion of skull bone after 6 month follow up (Fig. 6). Patient still felt dizziness and headache.
Discussion
Patients with penile cancer are a common in developing countries as well as in Nepal. In Nepal, the majority of the penile cancer patients reach to referral hospital very late. Early detection and timely treatment management are required to get better the overall result [3].
Bilateral inguinal lymph nodes metastasis is very common in patients with penile carcinoma but bone metastasis is very rare. The beginning of bone metastasis in patients with penile carcinoma mostly occurs after 18 months after conformal diagnosis of carcinoma. Radiological examinations and histopathological confirmation are important tools for the diagnosis of this rare individual. With aims of palliative treatment of patients with penile carcinoma, surgery is the preferred alternative of the treatments, particularly for metastatic foci in the long skeletons [4].
Patients with primary penis carcinoma with positive histological findings and no lymph nodes involvement have little risk for tumor metastasis. These types of patients are also most excellent well-matched for organ-sparing or glans-sparing treatment. Distant metastasis of patients with penile carcinoma is rare, and metastasis to the bones is even rarer.
This patient had developed femur as well as asymptomatic lung metastasis. Distant metastasis to the lung, liver, bone, or brain is uncommon [1] in the range of 1 to 10 %. A series of 380 patients with penile carcinoma analyzed by Prem Raj Sigdel [3], were included in the study. In that study, 78.5 % had clinically node-positive
References A case report of early detection of rare femoral shaft bone metastasis in a penis cancer patient
- Diorio G.J., Leone A.R., Spiess P.E. Management of Penile Cancer. Urology. 2016; 96: 15-21. DOI: 10.1016/j.urology.2015.12.041
- Dorfinger K., Maier U., Base W. Parathyroid hormone related protein and carcinoma of the penis: paraneoplastic hypercalcemia. J Urol. 1999; 161(5): 1570.
- Sigdel P.R., Mahaseth N., Pokharel B.M., Thapa J., Jalan A., Gharti B.B., Pokharel G.P., Pandey G., Nepal U., Lamichhane N. Clinicopathological characteristics of carcinoma penis over 10 years in a tertiary-level oncology center in Nepal: a retrospective study of 380 cases.Int Urol Nephrol. 2023; 55(3): 589-96. DOI: 10.1007/s11255-022-03427-7 EDN: WSMPKV
- Sun J., Chen X., Xu Z., Tian J., Jin B. A rare case report of femoral neck metastasis secondary from penile carcinoma and literature review. Urol Case Rep. 2021; 38. DOI: 10.1016/j.eucr.2021.101692
