Acute cholecystitis as the first manifestation of primary pure squamous cell carcinoma of the gallbladder; a case report

Author: Bahadoram M., Barahman M., Davoodi M., Hassanzadeh S.
Journal: Сибирский онкологический журнал @siboncoj
Section: Случай из клинической практики
Article in issue: 4 т.21, 2022.
Free access
Background. scc of the gallbladder is characterized by more rapid and invasive growth with infiltration of the adjacent organs and less spread to the lymph nodes compared to adenocarcinoma of the gallbladder. it is a rare neoplasm that accounts for 1.4-12.7 % of gallbladder tumors. scc of the gallbladder has a poor prognosis. symptoms usually appear later when the disease has progressed and the malignancy has reached advanced stages. therefore, usually, the patients expire soon following the diagnosis. the etiology of the scc of the gallbladder is complex and is mostly associated with gallstones. Case description. We report a case of a 56-year-old man that had been suffering from colicky abdominal pain in the right upper quadrant for about two weeks before his admission. He did not have nausea, vomiting, shortness of breath, fever, lack of appetite, or weight loss. after evaluation, a diagnosis of acute cholecystitis was established and antibiotic therapy was initiated. However, he did not respond to medical therapy and underwent surgery. a tumor mass was detected during surgery. therefore, cholecystectomy and extended right hepatectomy were performed. the pathological evaluation of the biopsy specimen revealed squamous cell carcinoma. consequently, he underwent radiotherapy and chemotherapy and was followed up for two years. He acquired complete tumor remission. Conclusion. the present case highlights the requirement of considering further investigation on the histogenesis of scc of the gallbladder.
Primary squamous cell carcinoma of the gallbladder, periodic acid schiff reaction, extended right hepatectomy
Short address: https://sciup.org/140295747
IDR: 140295747 | UDC: 616.366-006.6+616.366-002 | DOI: 10.21294/1814-4861-2022-21-4-165-169
Острый холецистит как первое проявление первичного плоскоклеточного рака желчного пузыря: клинический случай
Актуальность. По сравнению с аденокарциномой плоскоклеточный рак желчного пузыря (ПРЖП) характеризуется более быстрым и инвазивным ростом с инфильтрацией соседних органов и более редким поражением лимфатических узлов. Это редкое новообразование, на долю которого приходится 1,4-12,7 % опухолей желчного пузыря. ПРЖП имеет плохой прогноз. Симптомы обычно появляются на поздних стадиях заболевания, в связи в чем пациенты часто умирают вскоре после постановки диагноза. Этиология ПРЖП сложная и в основном связана с наличием конкрементов в желчном пузыре. Описание случая. Пациент, 56 лет, поступил в стационар с жалобами на коликообразные боли в правом подреберье, которые возникли примерно за 2 нед до госпитализации; тошноты, рвоты, одышки, лихорадки, отсутствия аппетита или потери веса не отмечал. После обследования установлен диагноз острого холецистита и начата антибактериальная терапия, которая не дала положительных результатов, и пациенту была выполнена операция, при ревизии обнаружена опухоль желчного пузыря, что явилось показанием для холецистэктомии и расширенной правосторонней гемигепатэктомии. При гистологическом исследовании биопсийного материала выявлен плоскоклеточный рак. После операции назначена лучевая терапия и химиотерапия. При динамическом наблюдении в течение 2 лет отмечается полная ремиссия опухоли. Заключение. Представленный клинический случай подчеркивает необходимость дальнейшего изучения гистогенеза плоскоклеточного рака желчного пузыря.
Text of the scientific article Acute cholecystitis as the first manifestation of primary pure squamous cell carcinoma of the gallbladder; a case report
Carcinoma of the gallbladder is mostly seen in females and older ages and is the fifth most common cancer of the gastrointestinal (GI) system [1–5]. Primary carcinoma of the gallbladder has various histological subtypes. Adenocarcinoma is the most common subtype which accounts for 80–95 % of all primary carcinomas. Adenocarcinoma itself has different patterns including papillary, tubular, mucinous, or signetcell. In addition, squamous cell carcinoma (SCCs)/ adenosquamous cell carcinomas (ASCs) account for 2–10 % of all primary carcinomas. The other less common subtypes include undifferentiated carcinoma and small cell carcinoma/poorly differentiated endocrine carcinoma which account for 2–7 % and <4 % of primary carcinomas, respectively. Furthermore, some rare subtypes consist of tumors such as sarcomas or lymphomas [6, 7]. We report a case of a 56-year-old male that was diagnosed with acute cholecystitis but did not respond to medical therapy. Therefore, he underwent surgery and a mass of the gallbladder was detected. The pathological evaluation of the biopsy specimen revealed squamous cell carcinoma (SCC).
Case Presentation
A 56-year-old male visited our clinic with a two-week history of right upper quadrant (RUQ) pain. The pain would increase while laying down and had a colicky nature. The patients denied having nausea, vomiting, shortness of breath, fever, lack of appetite or, weight loss. His medical history included a history of rheumatology disorder since a year ago. On physical examination, there were RUQ tenderness and positive Murphy’s sign, and the gallbladder was palpable. The examination of the other parts of the abdomen was normal. The vital signs of the patient were normal; blood pressure – 110/80 cm Hg, heart rate – 82 beats/min, respiratory rate – 16/min, a body temperature of 37.5 °C.
Complete blood count revealed leukocytosis with a white blood cell count of around 12,000 ×103/uL.
Abdominal sonography was performed and revealed that the liver had normal size and echogenicity, and the gallbladder had increased wall thickness and contained some small stones (about 9–10 mm in size). Based on the clinical diagnosis of acute cholecystitis, treatment with ceftriaxone (1gr/intravenously (IV)/twice daily) and metronidazole (500 mg/IV/every eight hours TDS) was initiated. The patient underwent cholecystectomy since he showed no response to treatment after four days of medical therapy. On surgery, a mass in the fundus and body of the gallbladder with some extension to the fourth segment of the liver was detected. Therefore, cholecystectomy and an extended right hepatectomy were performed. Drainage was achieved with the closed suction method.
The biopsy specimens were sent for pathology evaluation. The microscopic examination of the gallbladder wall showed pathological changes caused by chronic cholecystitis along with a range of neoplastic alterations. The neoplastic tissue comprised of neoplastic cells with a squamous pattern containing polymorphism in the nuclei, greater nucleus to cytoplasm ratio, and hyperchromatosis which was accompanied by a proliferation of horny cells. The inflammatory reaction of huge multi-nuclei horny cells was remarkable. The extension of this tissue was observed to superficial muscular layers. Subsequently, the diagnosis of differentiated SCC was established (Fig. 1). In addition, periodic acid-Schiff (PAS) staining of the cancerous cells was negative.
The patient underwent a thorough evaluation to find the primary source of the tumor. The investigations were negative and the documents suggested that the gallbladder was the origin of the tumor. The patient was then referred to the oncology department to continue his treatment of advanced-stage SCC of
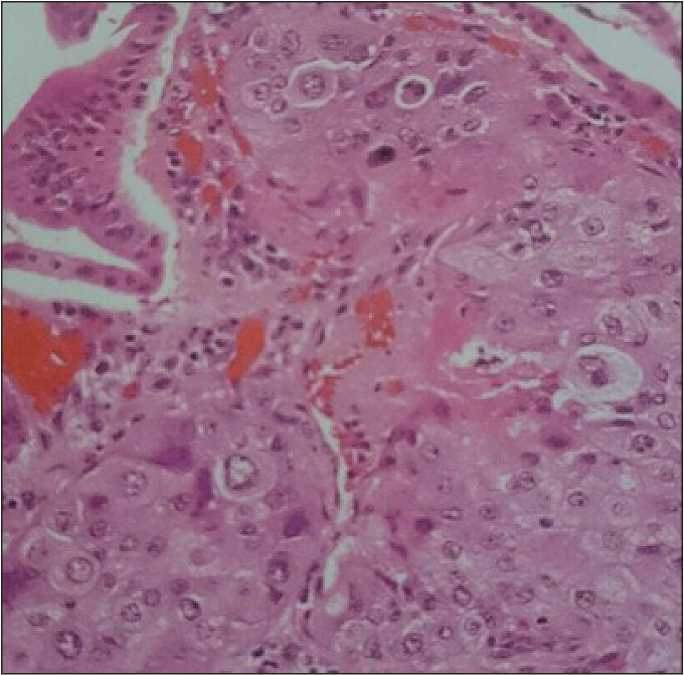
Fig. 1. Microphoto. Squamous cell carcinoma of the gallbladder, ×200
Рис. 1. Микрофото. Плоскоклеточный рак желчного пузыря, ×200
the gallbladder. He acquired complete tumor remission two months after the completion of conformal radiation therapy. He also underwent radiotherapy, chemotherapy, and follow-up for two years after his surgery.
Discussion
SCC of the gallbladder is characterized by more rapid and invasive growth with infiltration of the adjacent organs and less spread to the lymph nodes compared to adenocarcinoma of the gallbladder [2, 3]. Symptoms usually appear later when the disease has progressed and the malignancy has reached advanced stages, for example, when the liver or adjacent organs have been invaded and the lymph nodes are involved. Therefore, usually, the patients expire soon following the diagnosis. SCC of the gallbladder has a poor prognosis and is more prevalent in Chile, Japan, and northern India. The etiology of the SCC of the gallbladder is complex and is mostly associated with gallstones [1, 6, 8]. Secondary SCC of the gallbladder develops from the invasion of the neighboring structures or distant organs and is relatively more common than primary SCC of the gallbladder which originates from the gallbladder [8]. The lesion shows certain biological characteristics such as rapid growth, early metastatic dissemination, and diffuse local or regional infiltration. These tumors attach to the gallbladder along the fossa and grow to form large infiltrative masses. These masses invade the liver and adjacent organs (such as the abdomen, duodenum, and transverse colon) by direct expansion [8, 9]. This pattern was also observed and confirmed in our case. Despite its local and regional infiltration, SCC does not metastasis to the lymph nodes and seldom seeds in the peritoneum [10]. However, hepatic metastases, as seen in our case, are more commonly found in SCC than in adenocarcinoma of the gallbladder [8–10].
Most studies report that a pre-existing squamous epithelium that becomes metaplastic is usually from the origin of the squamous cells in the SCC of the gallbladder. However, other studies state that the squamous differentiation of the adenocarcinoma cells is the origin of SCC of the gallbladder through the expression of mixed phenotypes within a single tumor [8–10]. A characteristic of SCC is that its duplication time is half of that in adenocarcinoma; therefore, the expansion of the cells in SCC occurs more rapidly [7, 8].
The extent of SCC of the gallbladder at diagnosis is a determinate factor in the survival rate [8–10]. The majority of patients expire around six months after diagnosis when radical surgery is not performed [5]. This indicates the importance of early diagnosis of SCC of the gallbladder in the survival rate of patients. The surgical method depends on the amount of the local involvement and includes cholecystectomy with a wedge resection of a part of the liver tissue or liver resection with regional lymphadenectomy [2, 8]. In patients with localized lesions without any metastases or peritoneal involvement, radical surgery with resection of the involved organs may be performed. Hepato-pancreatic duodenectomy is the radical surgical method of choice radical operation of choice for SCC of the gallbladder because this is the main dissemination type seen in SCCs [2]. However, the long-term benefits of this treatment are not yet fully known. Postoperative radiotherapy and chemotherapy may be used as adjuvant therapies, but they have unpredictable results that may only be palliative. SCC is usually seen adjacent to adenocarcinoma on the submucosal membranes which gives an altered histological pattern between the adenocarcinoma and SCC surfaces. Therefore, squamous metaplasia of the adenocarcinoma should be considered as an involved factor in the pathogenesis of SCC [8, 9, 11]. Based on this hypothesis, SCC develops as a primary adenocarcinoma that undergoes squamous metaplasia and turns into adenosquamous cell carcinoma. Later, a metaplastic carcinoma proliferates and forms SCC in place of the adenocarcinoma.
Conclusion
The present study reports an invasive and metastatic squamous cell carcinoma of the gallbladder that was formed under the submucosa. Furthermore, PAS staining of cancerous cells was negative and there was no evidence of squamous metaplasia of the epithelium or displaced squamous epithelium. Additionally, no mucin production or rod-shaped structure was seen on the histologic serial sections. This case highlights the requirement of considering further investigation on the histogenesis of SCC of the gallbladder.
References Acute cholecystitis as the first manifestation of primary pure squamous cell carcinoma of the gallbladder; a case report
- Rustagi T., Dasanu C.A. Risk factors for gallbladder cancer and cholangiocarcinoma: similarities, differences and updates. J Gastrointest Cancer. 2012; 43(2): 137-47. doi: 10.1007/s12029-011-9284-y.
- Boutros C., Gary M., Baldwin K., Somasundar P. Gallbladder cancer: past, present and an uncertain future. Surg Oncol. 2012; 21(4): 183-91. doi: 10.1016/j.suronc.2012.08.002.
- Lai C.H., Lau W.Y. Gallbladder cancer--a comprehensive review. Surgeon. 2008; 6(2): 101-10. doi: 10.1016/s1479-666x(08)80073-x.
- Wernberg J.A., Lucarelli D.D. Gallbladder cancer. Surg Clin North Am. 2014; 94(2): 343-60. doi: 10.1016/j.suc.2014.01.009.
- Mastoraki A., Papanikolaou I.S., Konstandiadou I., Sakorafas G., Safioleas M. Facing the challenge of treating gallbladder carcinoma. Review of the literature. Hepatogastroenterology. 2010; 57(98): 215-9.
- Chakrabarti I., Giri A., Ghosh N. Cytohistopathological correlation of a case of squamous cell carcinoma of gallbladder with lymph node metastasis. Turk Patoloji Derg. 2014; 30(1): 81-4. doi: 10.5146/ tjpath.2013.01180.
- Kais H., Hershkovitz Y., Sandbank J., Halevy A. Port site metastases in squamous cell carcinoma of the gallbladder. Isr Med Assoc J. 2014; 16(3): 177-9.
- HosseinzadehM., ShokripurM., Salahi H. Primary pure squamous cell carcinoma of gallbladder presenting as acute cholecystitis. Iran J Med Sci. 2012; 37(4): 271-3.
- Al-Ramthan A., Ayash E., Asfar S. Squamous cell carcinoma of the gall bladder masquerading as a liver abscess. Kuwait Medical Journal. 2014; 46(1): 54-6.
- Rustagi T., Rai M., Menon M. Ruptured adenosquamous cell carcinoma of the gallbladder: case report and review of literature. Gastrointestinal cancer research: GCR. 2011; 4(1): 29-32.
- Zou Q., Yang Z.L., Yuan Y., Li J.H., LiangL.F., Zeng G.X., Chen S.L. Clinicopathological features and CCT2 and PDIA2 expression in gallbladder squamous/adenosquamous carcinoma and gallbladder adenocarcinoma. World J Surg Oncol. 2013; 11: 143. doi: 10.1186/1477-7819-11-143.
