Breast cancer awareness package on knowledge, attitude and practice towards breast self examination to prevent breast cancer among women in adopted communities - a pilot analysis

Author: Priyadarshini P., Sarath S., Hemavathy V.
Journal: Cardiometry @cardiometry
Section: Original research
Article in issue: 22, 2022.
Free access
Breast health is extremely important for all women. However, the breast is another region of the human body that is susceptible to cancer. Breast cancer is becoming increasingly common these days, and it is now one of the leading causes of mortality globally. According to the World Health Organization, breast cancer is the most common disease among women worldwide, claiming the lives of hundreds of thousands of women each year and impacting nations at all stages of development. In fact, it is the most common cancer in women, with a significant incidence observed among those aged 30 to 50. The goal of the World Health Organization’s Worldwide Breast Cancer Initiative (GBCI) is to reduce global breast cancer mortality by 2.5 percent each year; As a result, 2.5 million breast cancer deaths will be avoided globally between 2020 and 2040. To achieve these goals, three pillars must be in place: health endorsement for early detection, suitable identification at the right time, and comprehensive breast cancer management. Because of advances in early detection and care, the incidence of women dying of breast cancer has decreased by 41% from 1989 to 2018. During that time, more than 403,000 breast cancer deaths were prevented.
Breast cancer, breast self examination, prevention, awareness package, malignant tumor
Short address: https://sciup.org/148324631
IDR: 148324631 | DOI: 10.18137/cardiometry.2022.22.471483
Text of the scientific article Breast cancer awareness package on knowledge, attitude and practice towards breast self examination to prevent breast cancer among women in adopted communities - a pilot analysis
P. Priyadarshini, Sathiyalatha Sarath, Hemavathy V. Breast cancer awareness package on knowledge, attitude and practice towards breast self examination to prevent breast cancer among women in adopted communities – a pilot analysis. Cardiom-etry; Issue 22; May 2022; p. 471-483; DOI: 10.18137/cardiom-etry.2022.22.471483; Available from: http://www.cardiometry. net/issues/no22-may-2022/breast_cancer_awareness_package
Because the breast plays such an important part in female sexuality, breast cancer has a deep and long-lasting influence on people. Fear, anxiety, and despair are common responses to real or suspected breast cancer [1]. In addition to any other disease that is prevalent in society, breast cancer is diagnosed in more women than various other types of cancer [2]. In the United States, 281,550 women are expected to be diagnosed with persistent breast cancer this year, with 49,290 women being diagnosed with non-inva-sive (in situ) breast cancer. Invasive breast cancer in women increased by half a percent every year from 2008 to 2017.This year, 2,650 males in the United States are likely to be diagnosed with invasive breast cancer. Fear of deformity, loss of sexual attractiveness, rejection by a spouse, and mourning are all common responses (Babington 2000). Breast cancer is a disease in which malignant (cancer) cells develop in the breast tissues. The term “breast cancer” refers to an abnormal development that originates in the breast cells. Breast cancer usually starts in the cells of the milk-producing glands, the lobules, or the ducts, the passageways that drain milk from the lobules to the nipple. When researching your family tree, don’t forget to dig into your father’s side of the family. In determining your personal risk of having breast cancer, your father’s side is just as essential as your mother’s side. Breast cancer can also start in the stromal tissues of the breast, which comprise the fatty and fibrous connective tissues.
1.1. Need for the Study
The 5-year survival rate indicates the percentage of persons who live for at least 5 years after being diagnosed with cancer. Percentage refers to how many out of 100 something is. Women with non-metastatic invasive breast cancer had a 90 percent 5-year survival rate [3].Women with non-metastatic invasive breast cancer had an 84 percent 10-year survival rate. After lung cancer, breast cancer is the second most common cause of death among women in the United States. Because of advances in early detection and care, the incidence of women dying of breast cancer has decreased by 41% from 1989 to 2018. As a result, about 403,000 breast cancer deaths were prevented over that time.
2 Literature Review
Effect of screening by clinical breast examination on and transience after 20 years: prospective, cluster randomized controlled trial in Mumbai by Indra-neel Mittra., Gauravi A Mishra et al. , (2021). The study’s conclusion is that clinical breast examinations performed every two years by primary health care providers significantly reduce breast cancer stage at diagnosis and result in a non-significant 15% reduction in overall breast cancer mortality (but a significant reduction of nearly 30% in mortality in women over 50) [4]. There was no reduction in the death rate among women under the age of 50. For the evaluation of breast cancer in lower and middle-income nations, there should be a thorough clinical breast examination.
Among female students at King Saud University in Riyadh, Saudi Arabia, Abdullah Nasser Alomair, Dania Ghazi Felemban,., et.,al (2020) conducted a research study on breast self-examination and its Knowledge, attitude, and practice, the majority of the feminine students in the sample, despite having ample knowledge about BSE and a positive attitude, did not perform BSE [5]. This might be a problem for breast cancer screening programmes and early detection. As a result, more intensive awareness initiatives for female students are required to take in mind their present status of breast cancer and BSE knowledge [6]. In addition, more research is needed to determine the reasons behind the poor usage of BSE . More use of the media as a significant source of knowledge is necessary for community progress and awareness.
Sherin Ishaaque, Nandini Gopalamenon et al. (2019) conducted a research on breast self-examination in a rural region of North Kerala and knowledge, attitude, and practice on it [7]. In this study, it was shown that of the women with a positive family history of breast cancer were unaware of BSE [8]. The importance of BSE in early identification and treatment of breast cancer was not communicated to family by doctors, which was rather disturbing [9]. Similar re- 472 | Cardiometry | Issue 22. May 2022
search and chances for teaching women while the studies are being conducted on a wide scale assist to uncover further gaps in BSE knowledge, attitude, and practice, as well as give [10].
In [5] Osei Owusu-Afriyie, Linda Ahenkorah Fondjo, et al (2017) performed a study on Breast Self-Examination Practice and Comparative Assessment of Knowledge and Attitudes [11]. In Ghanaian female secondary and tertiary school students BSE practice was found to be exceedingly rare in both secondary and postsecondary students, according to the survey [12]. Furthermore, secondary school pupils have a lower level of BSE knowledge. BSE training should be introduced into second-cycle schooling, and BSE should be practiced once a month, as advised [13]. With a greater focus on the teenager, campaigning and instruction must be enhanced, beginning at the elementary level and stressing practical knowledge.
3 Method and Materials
A pilot research was carried out [14]. To see if the study was relevant and practical, 40 women from the adopted communities of Sree Balaji Medical College and Hospital were studied in the same way as the original study [15]. Data was evaluated to determine the statistics’ appropriateness [16].
3.1. The Purpose of this Research
The goal of this study was to assess the impact of a Breast Cancer Awareness Package on knowledge, attitudes, and behaviours related to breast self-examination in order to prevent breast cancer in women in adopted communities Title of the study:
“A Study To Assess The Effectiveness Of Breast Cancer Awareness Package On Knowledge, Attitude And Practice Towards Breast Self-Examination To Prevent Breast Cancer Among Women In Adopted Communities Of Sree Balaji Medical College And Hospital” [17].
3.2. Objectives of the Study 3.2.1. To assess the existing knowledge, attitude, practice score regarding prevention of breast cancer 3.2.2. To assess the knowledge, attitude, and practice score after the influence of the breast awareness package regarding prevention of breast cancer. 3.2.3. To assess association between the knowledge, attitude and practice and selected demographic variables
4 Research Methodology 4.1. Methodology: 4.1.1. Study Design (Type of Study)
Cross sectional design was adopted in their study.
-
4.1.2. Study Area
-
4.1.3. Study Population:
-
4.1.4. Sampling Methods:
-
4.1.5. Inclusion Criteria
This study was conducted in selected communities of Sree Balaji Medical College and Hospital, Community Medicine, Padappai
In this study, sample refines those women between the age group 30 - 60 years, residing in adopted communities of Sree Balaji Medical College and Hospital, Community Medicine, Padappai.
The patients who are the age period grouping between 30 to 60 years in Sree Balaji Medical College and Hospital, Community Medicine, Padappai.
-
• Women between the ages of 30 and 60 years old
-
• Willing to join
-
• Able to communicate in Tamil and English
-
4.1.6. Exclusion Criteria
• Women who have been diagnosed with breast cancer and are now undergoing treatment.
4.2. Data Collection Instruments (Data Questionnaire, Tools, Equipments)
4.2.1. Tools Used for Data Collection:
4.2.1.1. Tool 1: Demographic Variables of Women
4.2.1.2. Tool 2: Structured Interview Schedule on Knowledge on Prevention Package4.2.1.3. Tool 3: Attitude Related to Self-Breast Examination Practice
4.2.1.4. Tool 4: Practice Related to Self-Breast Examination Practice
4.2.1.5. Tool 5: Breast Cancer Awareness Package
4.3. Ethical Considerations
Table 1
Demographic Variables
Data analysis methods: Descriptive and inferential statistics will be used to analyze the data in accordance with the study’s goals.
The proposed study was carried out with the agreement of the Institution’s Research and Ethical Committee. Permission was received from the Institution’s Head [18]. The Dean of Sree Balaji Medical College and Hospital and the head of the community medicine department gave their assent for the pilot project [19]. Before beginning the data collection, each subject gave their informed permission and was assured that their identity would be protected.
Table 1. Shows the Demographic Information of Women who participated in the Following Study. A study to assess the effectiveness of a breast cancer awareness package on knowledge, attitude, and practice toward breast self-examination to prevent breast cancer among women in Sree Balaji Medical College and Hospital’s adopted communities.
Table 2 represents the life style variables of women those who are take part in this study.
Table 3 lists the clinical characteristics of the women who took part in this investigation.
|
Demographic variables |
Number of women |
Percentage(%) |
|
|
Age |
30 to 40 years |
10 |
25.00 |
|
40 to 50 years |
18 |
45.00 |
|
|
50 to 60 years |
12 |
[1]30.00 |
|
|
Religions |
Hindus |
30 |
75.00 |
|
Christians |
6 |
15.00 |
|
|
Muslims |
4 |
10.00 |
|
|
Weight |
Below 50 kg |
5 |
12.50 |
|
50 to 70 kg |
28 |
70.00 |
|
|
70 to 80 kg |
7 |
17.50 |
|
|
Greater than80 kg |
0 |
0.00 |
|
|
Age of menarche |
Below 12 years |
30 |
75.00 |
|
13 years |
5 |
12.50 |
|
|
14 years |
5 |
12.50 |
|
|
Above 14 yrd |
0 |
0.00 |
|
|
Demographic variables |
Number of women |
Percentage(%) |
|
|
literacy |
Primary |
12 |
30.00 |
|
Middle |
7 |
17.50 |
|
|
Higher secondary |
14 |
35.00 |
|
|
Graduate |
7 |
17.50 |
|
|
Occupation |
Daily wages |
16 |
40.00 |
|
Private company |
8 |
20.00 |
|
|
Government |
2 |
5.00 |
|
|
House wife |
14 |
35.00 |
|
|
Socio economic status |
Upper class |
3 |
7.50 |
|
Upper middle class |
11 |
27.50 |
|
|
Middle class |
6 |
15.00 |
|
|
Lower middle class |
10 |
25.00 |
|
|
Lower class |
10 |
25.00 |
|
|
Marital status |
Married |
35 |
87.50 |
|
Unmarried |
0 |
0.00 |
|
|
Divorced |
0 |
0.00 |
|
|
Widow |
5 |
12.50 |
|
|
Age of marriage |
Below 20 |
15 |
37.50 |
|
20 to 30 |
15 |
37.50 |
|
|
30 to 40 |
5 |
12.50 |
|
|
Above 40 |
5 |
12.50 |
|
|
Type of marriage |
Consanguineous |
29 |
72.50 |
|
Non consanguineous |
11 |
27.50 |
|
|
Sexual history |
Daily |
3 |
7.50 |
|
Once in a week |
7 |
17.50 |
|
|
2 weeks once |
5 |
12.50 |
|
|
Once in a month |
20 |
50.00 |
|
|
Not in sexual relation |
5 |
12.50 |
|
|
Number of children |
Nil |
9 |
22.50 |
|
One |
8 |
20.00 |
|
|
Two |
14 |
35.00 |
|
|
Greater than Two |
9 |
22.50 |
|
|
History of breast-feeding |
[15]6 months Maximum |
19 |
47.50 |
|
1 year Maximum |
13 |
32.50 |
|
|
2 years Maximum |
3 |
7.50 |
|
|
Not a breast fed |
5 |
12.50 |
|
|
History of abortion |
Yes |
17 |
42.50 |
|
No |
23 |
57.50 |
|
|
if yes |
1 |
12 |
70.59 |
|
2 |
5 |
29.41 |
|
|
3 |
0 |
0.00 |
|
|
Greater than3 |
0 |
0.00 |
|
|
Use of contraceptives |
Copper T |
12 |
30.00 |
|
Oral contraceptive pills |
7 |
17.50 |
|
|
Not used |
21 |
52.50 |
|
Table 2
Life Style Variables
|
Number of women |
Percentage (%) |
||
|
Dietary habit |
Vegetarian |
12 |
30.00 |
|
Non Vegetarian |
28 |
70.00 |
|
|
Intake of fatty and grilled foods |
Yes |
16 |
40.00 |
|
No |
24 |
60.00 |
|
|
light exposure at night / Night shift employees |
Yes |
16 |
40.00 |
|
No |
24 |
60.00 |
|
|
History of exercise |
Yes |
14 |
35.00 |
|
No |
26 |
65.00 |
|
Table 3
Clinical Variables
Table 6
Pretest Level of Practice Score
|
Level of achievement |
Women’s number |
Percentage (%) |
|
Deficient |
25 |
65.00 |
|
Average |
15 |
35.00 |
|
Satisfactory |
0 |
0.00 |
|
Total |
40 |
100.00% |
Table 8
Pretest and Posttest Level of Knowledge Score Comparison
|
score level |
[1]Pre-test |
Post-test |
Extended Mc-Nemar’s test |
||
|
n |
% |
n |
% |
||
|
Deficient |
27 |
67.50% |
0 |
0.00% |
χ 2=47.50 P=0.001***(S) |
|
Average |
13 |
32.50% |
9 |
22.50% |
|
|
Satisfactory |
0 |
0.00% |
31 |
77.50% |
|
|
Total |
40 |
100.00% |
40 |
100.00% |
|
Pretest and Posttest Level of Knowledge Score Comparison ***p 0.001 indicates a very high level of significance.
Objective 2: Assess the knowledge, attitude, and practice score after the influence of the breast awareness package regarding prevention of breast cancer.
Table 7 tells us the percentage level of post-test knowledge score among women. In general, none of the women have deficient knowledge level score, 22.50% of them having average knowledge level score and 77.50% of them have satisfactory knowledge level score.
Table 7
Score for the Posttest Level of Knowledge
|
Level of achievement |
Women’s number |
Percentage (%) |
|
Deficient |
0 |
0.00 |
|
Average |
9 |
22.50 |
|
Satisfactory |
31 |
77.50 |
|
Total |
40 |
100.00% |
Table 8 shows the pre-test and post-test knowledge level score among women. According to the breast awareness package, 67.50 percent of women have an inadequate degree of knowledge, 32.50 percent have a moderate level of knowledge, and none have an acceptable level of knowledge. Following the breast awareness package, the posttest revealed that none of the women had an insufficient level of knowledge, 22.50 percent had a moderate level of knowledge, and 77.50 percent had an appropriate level of knowledge. By using Extended McNemar’s chi square test the amount of score difference between the pretest and posttest is significant. The difference in level of knowledge acquired between the pretest and posttest was determined.
Table 9 Compare the total knowledge score before and after the breast awareness package was admin-
Table 9
Pretest and Posttest Mean Knowledge Score Comparison
On average, women raised their knowledge score from 14.73 to 23.53 after receiving a breast awareness package; in details that can be referred in Figure 1. Or, to put it another way, before intervention, they could only answer 15 out of 30 questions correctly; after intervention, they can only answer 24 out of 30 questions correctly, implying that intervention improved their ability to answer 9 questions correctly.
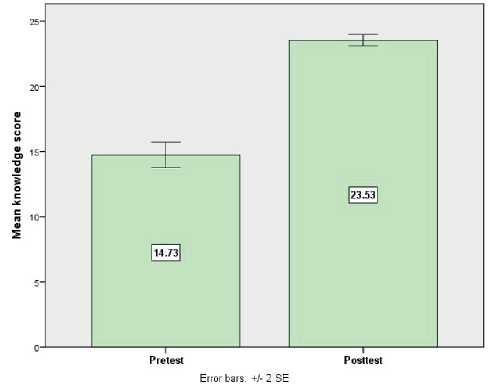
Figure 1. The Pretest and Posttest Knowledge Scores are compared using a Simple Bar Diagram with Two Standard Error Bars.
Table 10 demonstrates the impact of a breast cancer awareness package on knowledge.
Table 10
Breast Awareness Package Effectiveness and Knowledge Generalization Gain Score
|
Maximum score |
Average score |
Percentage of Knowledge score |
With a 95% confidence interval, the mean difference in knowledge gain score |
With a 95% confidence interval, the percentage of knowledge gained is calculated. |
|
|
Pretest |
30 |
14.73 |
49.10% |
8.80 (7.70 – 9.90) |
29.33% (25.67% – 33.00%) |
|
Posttest |
30 |
23.53 |
78.43% |
Women obtained 29.33 percent more knowledge in the posttest after receiving the breast awareness package than in the pretest. The mean difference with 95 percent confidence intervals and the proportion with 95 percent confidence intervals were used to determine generalization and differences in knowledge score gain score between pretest and posttest.
Table 11 illustrates the percentage level of women’s post-test attitude score. In general, none of the women have an insufficiently bad attitude score, 25.00 percent have a moderate level of attitude score, and 75.00 percent have a good level of attitude score.
Table 11
Score for the Post Test Level of Attitude
The amount of score difference between the pretest and posttest is significant. The Extended Mc Nemar’s chi square test was used to calculate the level of attitude gain between the pretest and posttest.
Table 13 compares the overall attitude score before and after the breast awareness package was administered. Women had a 48.35 attitude score on the pretest and a 73.33 attitude score on the posttest, resulting in a mean difference of 24.98 attitude score, which is a big and statistically significant attitude gain score for Statistical significance was assessed using the student’s paired’t’ test. Following the delivery of the breast awareness package, women’s attitudes increased on average from 48.35 to 73.33 which details are shown in Figure 2.
Table 12 display the level of attitude score of pretest and post-test core among women
Table 12
Comparison of Pretest and Posttest Level of Attitude Score
|
Level of [1]score |
Pretest |
Posttest |
Extended McNemar’s test |
||
|
n |
% |
n |
% |
||
|
Deficient |
28 |
70.00% |
0 |
0.00% |
χ2=36.20 |
|
Average |
12 |
30.00% |
10 |
25.00% |
P=0.001***(S) |
|
Satisfactory |
0 |
0.00% |
30 |
75.00% |
|
|
Total |
40 |
100.00% |
40 |
100.00% |
|
***p 0.001 indicates a very high level of significance
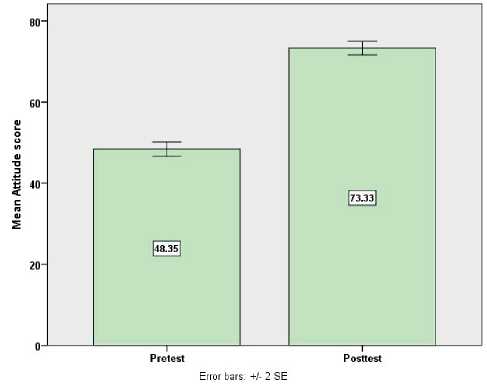
Figure 2. Diagram of a simple bar with two standard error bars compares the attitude score before and after the exam.
Table 14 enhances the effectiveness of a breast awareness package on attitude.
Prior to receiving the breast awareness package, 70.00 percent of women had an insufficient level of attitude, 30.00 percent had a moderate level of attitude,
Table 13
Pretest and Posttest Mean Attitude Score Comparison
|
Number of Women |
Pre-test |
Post-test |
Average |
Student’s paired t-test |
||
|
Average |
Standard Deviation |
Average |
Standard Deviation |
|||
|
40 |
48.35 |
5.66 |
73.33 |
5.25 |
24.98 |
t=20.33 [1]p=0.001 *** df= 39 , Significance |
Table 14
Generalization of Attitude Gain Score and Effectiveness of Breast Awareness Package
|
Maximum score |
The average score |
Percentage of Attitude score |
With a 95% confidence interval, the mean difference in attitude gain score |
Score of Attitude Gain in Percentage with a 95% Confidence Interval |
|
|
Pretest |
100 |
48.35 |
48.35% |
24.97 (22.49 – 27.45) |
24.97% (22.49% – 27.45%) |
|
Posttest |
100 |
73.33 |
73.33% |
On an average, after having breast awareness package, in posttest women are gained 24.97% attitude score is higher than the pre-test score. The mean difference with 95 percent confidence intervals and the proportion with 95 percent confidence intervals were used to determine differences and generalization of attitude score gain score between pretest and posttest.
The percentage level of post-test practice score among women is shown in Table 15. In general, none of the women have a low level of practice, 22.50 percent have a moderate level of practice, and 77.50 percent have a high degree of practice.
Table 15
Posttest Level of Practice Score
|
Level of score |
No. of Women |
Percentage (%) |
|
Deficient |
0 |
0.00% |
|
Average |
9 |
22.50% |
|
Satisfactory |
31 |
77.50% |
|
Total |
40 |
100.00% |
The pretest and post-test level of practice score among women is shown in Table 16.
Table 16
Pretest and Posttest Levels of Practice Score Comparison
|
[1]Score Level |
Pre-test |
Post-test |
Extended McNemar’s Test |
||
|
n |
% |
n |
% |
||
|
Deficient |
25 |
70 |
0 |
0 |
χ2=33.07 p=.001***(S) |
|
Average |
15 |
30 |
9 |
22.50 |
|
|
Satisfactory |
0 |
0 |
31 |
77.50 |
|
|
Total |
40 |
100% |
40 |
100% |
|
*** p 0.001 indicates a very high level of significance.
Prior to receiving the breast awareness package, 70.00 percent of women had an inadequate level of practice, 30.00 percent had a moderate level of practice, and none of them had an appropriate level of practice. In the posttest after receiving the breast
478 | Cardiometry | Issue 22. May 2022
awareness package, none of the women had an insufficient bad level of practice score, 22.50 percent had a moderate level of practice score, and 77.50 percent had an excellent level of practice score. The amount of score difference between the pretest and posttest is significant. The Extended McNemar’s chi square test was used to calculate the level of practice gain score between the pretest and posttest.
Table 17 compares the overall practice score before and after the breast awareness package was administered. Women had a pretest practice score of 30.00 and a posttest practice score of 47.10, resulting in a mean difference of 17.10 practice score. This difference is big and statistically significant practice gain score, as determined by the student’s paired’t ‘test. Women’s practice scores improved on average from 30.00 to 47.10 after being directed to a breast awareness package.
Table 17
Comparison of Pre-Test and Post-Test Mean Practice Score
|
Number of Women |
Pre-test |
Post-test |
Average |
Student’s paired t-test |
||
|
Average |
Standard Deviation |
Average |
Standard Deviation |
|||
|
40 |
30 |
2.8 |
47.1 |
3.11 |
17.1 |
t=30.32[1] P=0.001 *** DF= 39 , Significant |
Table 18 displays the effectiveness of a breast awareness package on practice. Women obtained 29.17 percent more practice on the posttest after receiving the breast awareness package than in the pretest. Differences in practice score gain score between pretest and posttest were estimated using a mean difference with 95 percent confidence interval and a proportion with 95 percent confidence interval. Figure 3 discusses about bar diagram with two standard error bars with the practice score before and after the pretest.
Table 18
Effectiveness of Breast Awareness Package and Score Gained From Generalization Of Practice
|
Maximum score |
Average score |
Percentage of Practice score |
With a 95% confidence interval, the mean difference in practice gain score |
Practice increase score as a percentage with a 95% confidence interval |
|
|
Pretest |
60 |
30.00 |
50.00% |
17.50 (15.75 – 18.44) |
29.17% (26.25% – 30.73%) |
|
Posttest |
60 |
47.10 |
78.50% |
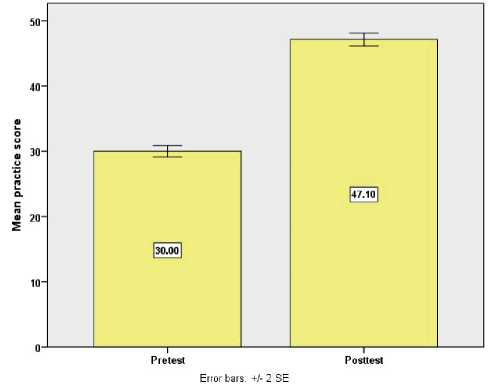
Figure 3. Simple bar diagram with two standard error bars Compares the practice score before and after the pretest.
The Table 19 above demonstrates the relationship between women’s demographic factors and their post-test level of knowledge score. Women who are older and more educated have a higher knowledge score than others. It was confirmed using chi-square test and Yates corrected chi-square test.
Table 20 above demonstrates the relationship between women’s demographic factors and their posttest level of attitude score. Women who are older and more educated have a higher knowledge score than others. It was confirmed using chi-square test and yates corrected chi-square test.
Table 21 demonstrates the relationship between women’s demographic factors and their post-test level of practice score. Women who are older and more educated have a higher knowledge score than others. It was confirmed using chi-square test and Yates corrected chi-square test.
Table 19
Demographic Variables and Posttest Level of Knowledge Score Association
|
Variables in demographics |
Knowledge level after the test |
n |
Chi Square test/ Yates corrected chi square-test |
||||
|
Average |
Satisfactory |
||||||
|
n |
% |
n |
% |
||||
|
Age |
30-40 years |
5 |
50.00% |
5 |
50.00% |
10 |
Х 2=3.87 [1] p=.05*(s) |
|
40-60 years |
4 |
13.33% |
26 |
86.67% |
30 |
||
|
Religions |
Hindus |
7 |
23.33% |
23 |
76.67% |
30 |
χ2=1.57 P=0.45(NS) |
|
Christians |
2 |
33.33% |
4 |
66.67% |
6 |
||
|
Muslims |
0 |
0.00% |
4 |
100.00% |
4 |
||
|
Weight |
Below 50 kg |
8 |
24.24% |
25 |
75.76% |
33 |
χ2=0.32 P=0.56(NS) |
|
70 -80 kg |
1 |
14.29% |
6 |
85.71% |
7 |
||
|
Age of menarche |
Below 12 years |
6 |
20.00% |
24 |
80.00% |
30 |
χ2=0.43 P=0.51(NS) |
|
13-14years |
3 |
60.00% |
7 |
40.00% |
10 |
||
|
literacy |
School |
9 |
41.67% |
24 |
58.33% |
33 |
x 2=4.03 P=0.05*(S) |
|
Graduate |
0 |
0.00% |
7 |
100.00% |
7 |
||
|
Occupation |
Employed |
5 |
31.25% |
11 |
68.75% |
16 |
χ2=0.02 P=0.87(NS) |
|
House wife |
4 |
28.57% |
10 |
71.43% |
14 |
||
|
Socio economic status |
Upper class |
2 |
14.28% |
12 |
85.72% |
14 |
χ2=0.83 P=0.36(NS) |
|
Middle class |
7 |
26.92% |
19 |
73.08% |
26 |
||
|
Marital status |
Married |
7 |
20.00% |
28 |
80.00% |
35 |
χ2=1.00 P=0.32(NS) |
|
Widow |
2 |
40.00% |
3 |
60.00% |
5 |
||
|
Age of marriage |
Below 40 |
9 |
25.71% |
26 |
74.29% |
35 |
χ2=2.78 P=0.10(NS) |
|
Above 40 |
0 |
0.00% |
5 |
100.00% |
5 |
||
|
Type of marriage |
Consanguineous |
7 |
24.14% |
22 |
75.86% |
29 |
χ2=0.16 P=0.68(NS) |
|
Non consanguineous |
2 |
18.18% |
9 |
81.82% |
11 |
||
|
Sexual history |
With sexual relation |
8 |
0.00% |
27 |
100.00% |
35 |
χ2=0.02 P=0.88(NS) |
|
Not in sexual relation |
1 |
20.00% |
4 |
80.00% |
5 |
||
|
Variables in demographics |
Knowledge level after the test |
n |
Chi Square test/ Yates corrected chi square-test |
||||
|
Average |
Satisfactory |
||||||
|
n |
% |
n |
% |
||||
|
Number of children |
Nil |
1 |
11.11% |
8 |
88.89% |
9 |
χ2=0.22 P=0.63(NS) |
|
Having children |
8 |
25.81% |
23 |
74.19% |
31 |
||
|
Breast feeding history |
Breast feed |
9 |
25.71% |
26 |
74.29% |
35 |
χ2=2.78 P=0.09(NS) |
|
Not breast fed |
0 |
0.00% |
5 |
100.00% |
5 |
||
|
History of abortion |
Yes |
3 |
17.65% |
14 |
82.35% |
17 |
χ2=0.39 P=0.53(NS) |
|
No |
6 |
26.09% |
17 |
73.91% |
23 |
||
|
Use of contraceptives |
User |
3 |
14.29% |
16 |
85.71% |
21 |
χ2=0.93 P=0.33(NS) |
|
Not used |
6 |
28.57% |
15 |
71.43% |
21 |
||
Table 20
Association of Demographic Variables with the Posttest Level of Attitude Score
|
Variables in demographics |
Knowledge level after the test |
n |
Chi Square test/yates corrected chi square-test |
||||
|
Average |
Satisfactory |
||||||
|
n |
% |
n |
% |
||||
|
Age |
30-40 years |
5 |
50.00% |
5 |
50.00% |
10 |
X 2=4.44 [1]p=0.05*(S) |
|
40-60 years |
5 |
16.67% |
25 |
83.37% |
30 |
||
|
Religions |
Hindus |
6 |
20.00% |
24 |
80.00% |
30 |
χ2=1.60 p=0.20 (NS) |
|
Christians/ Muslims |
4 |
40.00% |
6 |
60.00% |
10 |
||
|
Weight |
Below 70 kg |
8 |
24.24% |
25 |
76.76% |
33 |
χ2=0.05 p=0.81 (NS) |
|
70 -80 kg |
2 |
28.57% |
5 |
71.43% |
7 |
||
|
Age of menarche |
Below 12 years |
6 |
20.00% |
24 |
80.00% |
30 |
χ2=1.60 p=0.20 (NS) |
|
13 -14years |
4 |
40.00% |
6 |
60.00% |
10 |
||
|
literacy |
School |
9 |
27.27% |
24 |
62.73% |
33 |
χ2=0.06 p=0.81 (NS) |
|
Graduate |
1 |
14.29% |
6 |
85.71% |
7 |
||
|
Occupation |
Employed |
3 |
11.53% |
23 |
88.47% |
26 |
x 2=5.27p=0.03* (S) |
|
House wife |
7 |
50.00% |
7 |
50.00% |
14 |
||
|
Socio economic status |
Middle to Upper class |
4 |
0.00% |
16 |
100.00% |
20 |
χ2=0.53 p=0.46 (NS) |
|
Lower class |
6 |
30.00% |
14 |
70.00% |
20 |
||
|
Marital status |
Married |
10 |
28.57% |
25 |
71.43% |
35 |
χ2=3.15 p=0.08 (NS) |
|
Widow |
0 |
0.00% |
5 |
100.00% |
5 |
||
|
Age of marriage |
Below 20 |
6 |
40.00% |
9 |
60.00% |
15 |
χ2=2.88 p=0.09 (NS) |
|
Above 20 |
4 |
13.33% |
21 |
86.67% |
25 |
||
|
Type of marriage |
Consanguineous |
7 |
24.14% |
22 |
75.86% |
29 |
χ2=0.04 p=0.83 (NS) |
|
Non consanguineous |
3 |
27.27% |
8 |
72.73% |
11 |
||
|
Sexual history |
In sexual relation |
7 |
20.00% |
28 |
80.00% |
35 |
χ2=3.73 p=0.06 (NS) |
|
Not in sexual relation |
3 |
60.00% |
2 |
40.00% |
5 |
||
|
Number of children |
Nil |
3 |
27.27% |
6 |
72.73% |
9 |
χ2=0.43p=0.51 (NS) |
|
Having children |
7 |
33.33% |
24 |
66.67% |
31 |
||
|
Breast feeding history |
Breast feed |
10 |
28.57% |
15 |
71.43% |
35 |
χ2=3.15 p=0.08 (NS) |
|
Not breast fed |
0 |
0.00% |
5 |
100.00% |
5 |
||
|
History of abortion |
Yes |
5 |
29.41% |
12 |
70.59% |
17 |
χ2=0.30 p=0.58 (NS) |
|
No |
5 |
21.74% |
18 |
78.26% |
23 |
||
|
Use of contraceptives |
User |
7 |
25.00% |
12 |
75.00% |
19 |
χ2=2.70 p=0.10 (NS) |
|
Not used |
3 |
14.29% |
18 |
85.71% |
21 |
||
Table 21
Association between Posttest Level of Practice Score and Demographic Variables
|
Variables in demographics |
Knowledge level after the test |
n |
Chi-square test |
||||
|
Average |
Satisfactory |
||||||
|
n |
% |
n |
N% |
||||
|
Age |
30-40 years |
5 |
50.00% |
5 |
50.00% |
10 |
χ 2=5.78 p=0.02* (S) |
|
40-60 years |
4 |
13.33% |
26 |
87.67% |
30 |
||
|
Religions |
Hindus |
7 |
23.33% |
23 |
76.67% |
30 |
χ2=0.04 p=0.86 (NS) |
|
Christians/muslims |
2 |
20.00% |
8 |
80.00% |
10 |
||
|
Weight |
Below 70 kg |
7 |
21.21% |
26 |
78.79% |
33 |
χ2=0.06 p=0.81 (NS) |
|
Greater than70 kg |
2 |
28.57% |
5 |
71.43% |
7 |
||
|
Age of menarche |
Below 12 years |
7 |
23.33% |
23 |
76.67% |
30 |
χ2=0.05 p=0.82 (NS) |
|
13 -14years |
2 |
20.00% |
8 |
80.00% |
10 |
||
|
literacy |
School |
7 |
8.33% |
26 |
91.67% |
33 |
χ2=0.17 p=0.67 (NS) |
|
Graduate |
2 |
28.57% |
5 |
71.43% |
7 |
||
|
Occupation |
Employed |
3 |
11.54% |
23 |
88.46% |
26 |
χ 2=5.11p=0.02* (S) |
|
House wife |
6 |
42.86% |
8 |
57.14% |
14 |
||
|
Socio economic status |
Middle to Upper class |
6 |
30.00% |
14 |
70.00% |
20 |
χ2=1.29 p=0.25 (NS) |
|
Lower class |
3 |
15.00% |
17 |
85.00% |
20 |
||
|
Marital status |
Married |
7 |
20.00% |
28 |
80.00% |
35 |
χ2=1.00 p=0.31 (NS) |
|
Widow |
2 |
40.00% |
3 |
60.00% |
5 |
||
|
Age of marriage |
Below 20 |
8 |
22.86% |
27 |
77.14% |
35 |
χ2=0.02 p=0.88 (NS) |
|
Above 20 |
1 |
20.00% |
4 |
80.00% |
5 |
||
|
Type of marriage |
Consanguineous |
5 |
17.24% |
24 |
82.76% |
29 |
χ2=1.67 p=0.19 (NS) |
|
Non consanguineous |
4 |
36.36% |
7 |
63.64% |
11 |
||
|
Sexual history |
in sexual relation |
7 |
15.00% |
28 |
85.00% |
35 |
χ2=2.09 p=0.15 (NS) |
|
Not in sexual relation |
0 |
0.00% |
5 |
100.00% |
5 |
||
|
Number of children |
Nil |
2 |
18.18% |
9 |
81.82% |
11 |
χ2=0.16 p=0.68 (NS) |
|
One |
7 |
24.13% |
22 |
75.87% |
29 |
||
|
Breast feeding history |
BREST FEEDING |
8 |
22.86% |
27 |
77.14% |
35 |
χ2=0.02 p=0.88 (NS) |
|
Not breast fed |
1 |
20.00% |
4 |
80.00% |
5 |
||
|
History of abortion |
Yes |
2 |
11.76% |
15 |
88.24% |
17 |
χ2=1.95 p=0.16 (NS) |
|
No |
7 |
30.43% |
16 |
69.57% |
23 |
||
|
Use of contraceptives |
Copper T |
4 |
25.00% |
15 |
75.00% |
19 |
χ2=0.04 p=0.83 (NS) |
|
Not used |
5 |
23.81% |
16 |
76.19% |
21 |
||
-
5 Validity and Reliability
The content validity of the instrument was used to determine its validity [20]. Experts from a variety of nursing and medical backgrounds assessed the content validity. They proposed various changes and improvements to the tool [21]. After all of the corrections and modifications, the experts agreed on this tool for evaluating the effectiveness of a breast cancer awareness package on knowledge, attitude, and practice toward breast self-examination to prevent breast cancer among women in Sree Balaji Medical College and Hospital’s adopted communities.
-
6 Conclusion
The tool’s reliability was tested after a pilot study utilizing the Test retest technique and the Cronbach Alpha method. The reliability correlation coefficient value of the knowledge score is 0.85, the reliability correlation coefficient value of the attitude score is 0.82, and the reliability correlation coefficient value of the practice score is 0.88. These correlation coefficients are very high, and the tool is useful for evaluating the effectiveness of a breast cancer awareness package on knowledge, attitude, and practice toward breast self-examination in breast cancer prevention among women in Sree Balaji Medical College and Hospital’s adopted communities. The chance of developing breast cancer is influenced by a number of variables. When contemplating the risk of breast cancer, keep in mind that the vast majority of women who get breast cancer have no obvious risk factors and no family history of breast cancer. This emphasizes the importance of every woman being aware of changes in her breasts. By providing public health education to raise awareness and understanding of the warning signs and symptoms of breast cancer among women and their families, as well as the importance of early detection and management, women who are first suspected of having breast cancer will seek medical advice before the cancer stage progresses.
Statement on ethical issues
Research involving people and/or animals is in full compliance with current national and international ethical standards.
Conflict of interest
None declared.
Author contributions
The authors read the ICMJE criteria for authorship and approved the final manuscript.
References Breast cancer awareness package on knowledge, attitude and practice towards breast self examination to prevent breast cancer among women in adopted communities - a pilot analysis
- WHO Breast cancer., 26 March 2021 - https://www.who.int/news-room/fact-sheets/detail/breast-cancer
- Harrison AP, Srinivasan K, Binu VS, Vidyasagar MS, Nair S (2010) Risk factors for breast cancer among women attending a tertiary care hospital in southern India. International Journal of Collaborative Research on Internal Medicine & Public Health 2: 109 -116.
- BMJ 2021; 372 doi: https://doi.org/10.1136/bmj. n256 (Published 24 February 2021)Cite this as: BMJ 2021;372:n256
- Hindawi International Journal of Breast Cancer Volume 2018, Article ID 7502047, 10 pageshttps://doi.org/10.1155/2018/7502047, Received 6 September 2017; Revised 1 March 2018; Accepted 2 July 2018; Published 30 July 2018
- Abdullah Nasser Alomair et al, 2020;4(2):429– 434.https://doi.org/10.24911/IJMDC.51-1576668182, Abdullah Nasser Alomair et al, 2020;4(2):429–434. https://doi.org/10.24911/IJMDC.51-1576668182
- Aich RK, Mondal NK, Chhatui B, Sepai HM, Aich R, et al. (2016) Relevance of risk factors of breast cancer in women: An Eastern Indian scenario. J Cancer Res Ther 12: 302-308.
- Pan SY, Zhou J, Gibbons L, Morrison H, Wen SW (2011) Antioxidants and breast cancer risk- a population- based case-control study in Canada. BMC Cancer 11: 372-384.
- Singh,A;Settleman,J(2010).”EMT,cancer stem cells and drug resistance”. Oncogene. 29:4741–4751.
- Jump upto: a b WangYP, LeiQY(2017). Perspectives of Reprogramming Breast Cancer Metabolism. Adv Exp Med Biol. Advances in Experimental Medicine and Biology.
- Velasco-Velazquez, MA; Popov, VM; Lisanti, MP (2011). “The role of breast cancer stem cells in meta stasis and therapeutic implications”. American Journal of Pathology
- Ahmed, Shaymaa J., Nawfal K. Yas, and Hatem A. Hatem. “DNA polymorphism of interleukin IL-4of nasal mucosal stem cells innasalpolyps of Iraqi patients.” International Journa of Bio-Technology and Research (IJBTR) 7.3 (2017):11-16.
- Bhadoria AS, Kapil U, Sareen N, Singh P (2013) Reproductive factors and breast cancer: a case-control study in tertiary care hospital of North India. Indian J Cancer 50: 316-321.
- Xu YL, Sun Q, Shan GL, Zhang J, Liao HB, et al. (2012) A case-control study on risk factors of breast cancer in China. Arch Med Sci 8: 303-309.
- Pijpe A, Andrieu N, Easton DF, Kesminiene A, Cardis E, et al. (2012) Exposure to diagnostic radiation and risk of breast cancer among carriers of BRCA1/2 mutations: retrospective cohort study (GENE-RADRISK). BMJ 345: 5660.
- Rollison DE, Brownson RC, Hathcock HL, Newschaffer CJ (2008) Case-control study of tobacco smoke exposure and breast cancer risk in Delaware. BMC Cancer 8: 157-166.
- Cui Y, Miller AB, Rohan TE (2006) Cigarette smoking and breast cancer risk: update of a prospective cohort study. Breast Cancer Res Treat 100: 293-299.
- Augustine P, Jose R, Peter A, Lal AA, Prabhakar J, et al. (2014) Risk factors of breast cancer in Kerala, India - A case control study. Academic Medical Journal of India 2: 7-13.
- Steindorf K, Schmidt M, Kropp S, Chang-Claude J (2003) Case-control study of physical activity and breast cancer risk among premenopausal women in Germany. Am J Epidemiol 157: 121-130.
- Tessaro S, Béria JU, Tomasi E, Victora CG (2003) Breastfeeding and breast cancer: a case-control study in Southern Brazil. Cad SaudePublica 19: 1593-1601.
- Sezer H, Yilmaz M, Gurler H, Koyuncu A (2011) Breast Cancer Risk Factors in Turkey: a Hospital-based Case-control Study. Asian Pac J Cancer Prev 12: 2317-2322.
- International Journal of Community Medicine and Public Health Ishaaque Setal. Int J Community Med Public Health.2019May;6(5):2069-2073, http://www.ijcmph.comp ISSN2394-6032|eISSN 2394-6040
