Cardiometric criteria for diagnostics, therapy, and prediction of COVID-19 virus infection development under hospital conditions

Author: Rudenko M.Y., Dvorina O.G., Zernov V.A., Voronova O.K.
Journal: Cardiometry @cardiometry
Article in issue: 18, 2021.
Free access
The topicality of the understanding and knowledge of the impact of the COVID-19 virus infection on the human organism is obvious. In this connection, all aspects are important: diagnostics, making decision on therapy, monitoring of the effectiveness of the administered therapy and prediction of the patient condition development. In the spring of 2020, the authors hereof obtained evidence data covering a group of patients diagnosed with the COVID-19 infection who were in the Red Zone of the inpatient treatment in one of the Moscow clinical institutions
Cardiometric criteria, covid-19 virus infection, hospital conditions
Short address: https://sciup.org/148321529
IDR: 148321529 | DOI: 10.18137/cardiometry.2021.18.1117
Text of the scientific article Cardiometric criteria for diagnostics, therapy, and prediction of COVID-19 virus infection development under hospital conditions
Mikhail Y. Rudenko, Olga G. Dvorina, Vladomir A. Zernov, Olga K. Voronova. Cardiometric criteria for diagnostics, therapy, and prediction of COVID-19 virus infection development under hospital conditions. Cardiometry; Issue 18; May 2021; p.11-17; DOI: 10.18137/ cardiometry.2021.18.1117; Available from: http://www.cardiometry. net/issues/no18-may-2021/prediction-of-covid-19
The topicality of the understanding and knowledge of the impact of the COVID-19 virus infection on the human organism is obvious. In this connection, all aspects are important: diagnostics, making decision on therapy, monitoring of the effectiveness of the administered therapy and prediction of the patient condition development. In the spring of 2020, the authors hereof obtained evidence data covering a group of patients diagnosed with the COVID-19 infection who were in the Red Zone of the inpatient treatment in one of the Moscow clinical institutions.
Materials and methods
For the purpose of the cardiometric diagnostics of the above mentioned group of the patients, we have employed cardiological PC-assisted device Cardiocode. The device has been designed to record an ECG and Rheogram in parallel in a patient that takes 30 seconds only. Then, in the automatic mode, the following data sets are calculated and displayed on the Cardiocode screen:
-
1. Hemodynamic parameters: - SV – stroke volume of blood (ml),
-
- MV – minute volume (l / min),
-
- PV1 – the volume of blood entering the ventricle during the early diastole (ml),
-
- PV2 – the volume of blood entering the ventricle during the atrial systole (ml),
-
- PV3 – the volume of blood ejected by the ventricle during the rapid ejection phase (ml),
-
- PV4 – the volume of blood ejected by the ventricle during the slow ejection phase (ml),
-
- PV5 – the volume of blood pumped by the ascending aorta in the systole (ml).
-
2. The above parameters are utilized to calculate the ejection fraction ratio RV1= PV1/SV (%). It is expressed as a percentage representing the ratio of the incoming volume of blood in the left ventricle in the early diastole to the blood volume ejected into the aorta. This parameter shows the capability of the heart to cover the actual blood demand by a human organism. Normally, this value is about 62%; higher values thereof are the indicators of hypertrophy of the heart, and the values below this limit value are markers of the heart hypofunction.
-
3. Another complete set of important indicators is formed by the metabolic characteristics in the heart muscle fiber cells, which are as follows:
-
- the concentration of oxygen in the myocardial muscle fiber cells (O 2 ),
-
- the concentration of lactate,
-
- the concentration of phosphocreatine (PC).
-
4. The system parameters of the regulation are as listed below:
-
- the indicator of heart rate variability, stress index SI, - the degree of mental concentration of attention, - the actual type of actual adaptation reactions.
The therapy was carried out with the use of noninvasive therapeutic device “EZh-2"designed to generate low-intensity electromagnetic field frequencies. The specific EMF parameters of the device are aimed at controlling the desired adaptation reactions in a human body. The produced EMF frequencies due to the bioresonance induce the genome expression. This brings the immune system performance to its optimal level that makes possible to achieve a pronounced therapeutic effect: the T-cell immunity is stimulated, and cell metabolism is activated. Also, the operation of enzymes is intensified.
Table 1
Results of the cardiometric diagnostics and therapy of patients with COVID-19
|
Patient No.3 |
CT diagnosis |
CRP, mg/l |
Diagnosis & Disease History |
Cardiometric diagnosis when being in the COVID-19 Red Zone |
Ejection fraction RV1, % (norm 62%) |
Use of the EZh-2 device |
О 2 (0.85… 0.5 arb.u.) |
SI (250 arb.u.) |
|
1 |
3 |
317.54 /3.86 |
Pneumonia |
The slow ejection phase indicates Weak respiration. The blood volume supplied to the coronary arteries is sufficient |
47 |
+ at the beginning |
0.6..0.4 |
80… 200 |
|
2 |
1 |
Pneumonia |
Cardiosclerosis |
49 |
+ after resuscitation |
0.7..0.6 |
60… 80 |
|
|
3 |
2/3 |
CHD, spinal surgery. Pneumonia |
Decreased blood flow in the coronary arteries |
62 |
+ |
0.8..0.9 |
300… 1000 |
|
|
4 |
3 |
Atherosclerosis, Stenosis of the left internal carotid artery 76%. Pneumonia |
The slow ejection phase does not provide blood volumes for the coronary arteries. Weak respiration |
39 |
+ |
0.2..0.2 |
100… 100 |
|
|
5 |
4 |
Pneumonia |
The slow ejection phase does not provide blood volumes for the coronary arteries. Weak respiration |
38 |
+ |
0.3..0.2 |
2200... 3000 |
|
|
6 |
- |
Pneumonia |
The slow ejection phase does not provide blood volumes for the coronary arteries. Weak respiration |
50 |
+ |
0.8..0.8 |
2000… 3000 |
|
|
7 |
3 |
Breast cancer. Radiation therapy. Pneumonia |
The slow ejection phase does not provide blood volumes for the coronary arteries. Weak respiration. AVV prolapse. Atherosclerosis |
49 |
+ |
0.5..0.5 |
4000... 1500 |
|
|
8 |
3 |
Skin cancer. Polychemotherapy. Pneumonia |
The slow ejection phase does not provide blood volumes for the coronary arteries. Weak respiration |
20 |
+ |
0.6..1.4 |
500… 80 |
|
|
9 |
3 |
Skin cancer. Radiation therapy |
The slow ejection phase does not provide blood volumes for the coronary arteries. Weak respiration |
52 |
+ |
0.4..0.6 |
150… 250 |
|
|
10 |
1 |
Pneumonia |
“The adrenaline heart” |
30 |
- |
0.8…0.5 |
90… 400 |
|
|
11 |
3 |
Pneumonia |
Problem of coronary blood flow. Signs of SCD |
36 |
- |
0.5 |
112 |
|
|
12 |
¾ |
Pneumonia |
Problem of coronary blood flow |
49 |
- |
1.0 |
3400 |
|
|
13 |
4 |
Pneumonia |
- |
- |
+ from the 4th day |
- |
||
|
14 |
Pneumonia |
- |
- |
- |
- |
- |
As a rule, in the circumstances many patients demonstrate poor immunity and have a number of chronic diseases. Therefore, preventive diagnostics is important in the COVID-19 treatment.
For the purpose of the cardiometric diagnostics, the ECG and Rheogram recording technology has been used that is fundamental for cardiometry. Figure 1 herein shows an example of the recorded ECG and Rheogram curves corresponding to the norm.
Results
Under the clinical conditions, using the Cardiocode device, 14 patients have been examined. The obtained examination results are presented in Table 1 herein. The most typical ECG recordings of patients cardiometric data are shown in Figure 2, 3 and 4 herein. For 5 of the 14 patients the lethal outcome was reported. Of concern to us were the background indicators, when the above patients were admitted to the hospital. Upon a detailed examination from the point of view
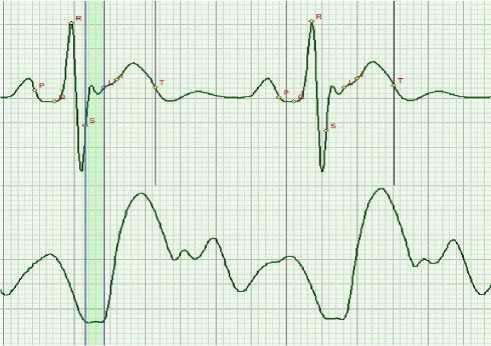
Figure 1. Typical normal ECG and Rheogram
Table 2. Blood biochemistry (CA-180)
|
Data |
29.04.2020 12:57 |
04.05.2020 07:30 |
|
Total protein [g/l] |
65.0 |
|
|
Glucose [mmol / L] |
4.78 |
4.46 |
|
Urea [mmol/L] |
7.10 |
|
|
Alpha-amylase [units / l] |
11 |
|
|
ALT [units/l] |
81 |
|
|
AST [units/l] |
90 |
|
|
ALKP [units/l] |
127 |
|
|
LDH [units/l] |
1273 |
|
|
Albumin [g/l] |
40.7 |
|
|
CRP, mg/l |
317.54 |
3.86 |
|
Creatinine [mmol / L] |
32.40 |
50.20 |

$у(мл) - Ударный объем
4909 000
223 (08 05 20 10 44 37)
% отношения систолического объё
Объемы крови % от ударного объема
Результат % отклонения Индикаторы результатов
1змерения измерений
05.05.20
05.05.20
Объем изгоняемый левым; tbasv медленного изгнания
Объём притекающим в систолу поедсеодия
Индекс Баевского
о

08.05
Объем, поступающий в желудочек в фазу
Объем изгоняемый левым (базу быстоого изгнания
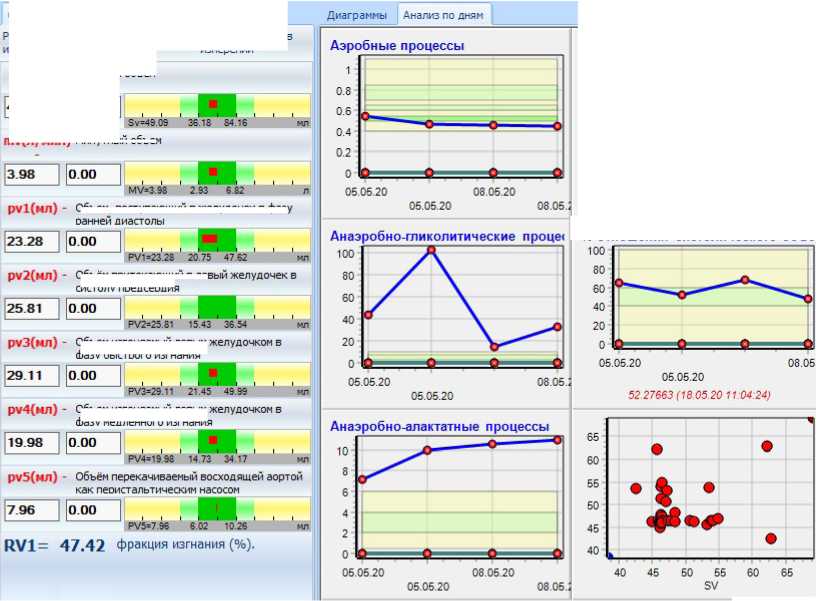
Figure 2. Patient 1 was treated with EZh-2. CT diagnosis: lung damage degree CT3. Ejection fraction RV1=47 %. Almost without any
medication. A typical example of an under-development of the slow ejection phase that is identifiable according to the Rheogram.
This patient has been cured.

Объемы крови % отударного объема
Аэробные процессы
$л/(мл) - Ударный объем
[206.08 | |з7.00 ]
14.05.:
Диаграммы Анализ по
12:15 33)
Результат % отклонения Индикаторы резу; измерения измерений
80 84 |о 00
1125.24 | |Э 6 О7 |
|83 69 |37.13
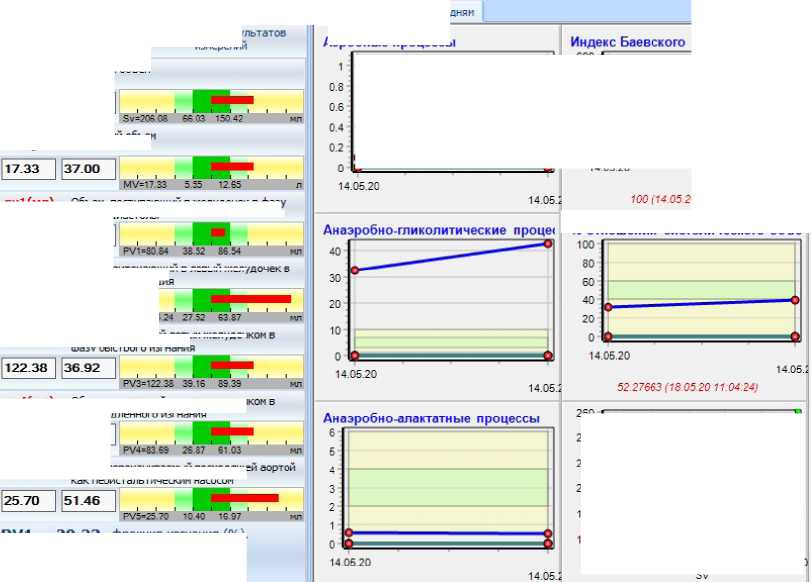
RV1= 39.23 фракция изгнания (%).
Figure 3. Patient 4. CT diagnosis: lung damage degree CT3. Ejection fraction RV1=39 %. A typical example of an under-development of the slow ejection phase that is identifiable according to the Rheogram. This patient has been cured. Significant deviations from the hemodynamic parameters are found.
% отношения систолического объё
of Cardiometry, we revealed a decline in the respiratory function during the phase of slow ejection. This phase of the cardiac cycle is responsible for the systolic blood pressure and the volume of blood required for normal blood filling of the coronary arteries [1]. As you can see, the actual blood filling conditions are not sufficient under COVID-19. Figure 2 and 3 present the cardiometric data of the cured patients, and Figure 4 exhibits the data recorded in a patient with the lethal outcome. In all the Figures, the slow ejection phase and an inclination of the Rheogram peak are marked with arrows.
In the given Table, the patients, who used the low-intensity EMF physiotherapy device EZh-2 in the course of treatment, are marked with the + sign. The device is commercially produced and widely used in practice as a therapy device for individual use.
For one female patient, the results of the CRP tests both before and after treatment are presented.
Discussions
Considering the presented data, it is important to highlight the main characteristic features which may


Figure 4. Patient 11. CT diagnosis: lung damage degree CT3. Ejection fraction RV1=36 %. Improper development of the slow ejection phase that is identifiable according to the Rheogram. Signs of possible SCD. The patient’s lethal outcome recorded.
be decisive for the COVID-19 complications, if any, we should note the following:
