Clinical and radiographic outcomes of medial open wedge high tibial osteotomy (MOWHTO) with Ilizarov technique in OA knee
 with Ilizarov technique in OA knee")
Author: Bari Mofakhkharul Bari, Islam Shahidul, Shetu Nazmul Huda, Rahman Mahfuzer
Journal: Гений ортопедии @geniy-ortopedii
Article in issue: 3, 2018.
Free access
High tibial osteotomy, medial open wedge osteotomy, knee osteoarthrosis, varus deformity, ilizarov''s apparatus
Short address: https://sciup.org/142213651
IDR: 142213651 | UDC: 616.718.5-001.5-089.227.85-073.7 | DOI: 10.18019/1028-4427-2018-24-3-307-311
Text of the article Clinical and radiographic outcomes of medial open wedge high tibial osteotomy (MOWHTO) with Ilizarov technique in OA knee
The surgical options available to treat surgical compartment osteoarthritis (OA) of the knee include osteotomies and unicompartmental replacement (UKR) and total knee replacement (TKR). Medial open wedge high tibial osteotomy (MOWHTO) has proved to be safe and effective and is a well-established surgical technique for the treatment of this disorder [1–3].
Initially overcorrection was recommended for this procedure [2], transferring the load from the damaged to the intact compartment of the knee and leading to a potential reduction of subchondral sclerosis [4] and regeneration of cartilage [5–7].
MOWHTO-Medial open wedge high tibial osteotomy is a widely accepted treatment option in young and active patients with medial compartment osteoarthritis in a varus knee [8]. The continuous nature of the opening of medial aspects of the proximal tibial metaphysis improves fine-tuning of alignment by Ilizarov technique [5]. MOWHTO fails when correction is not adequately produced in the postoperative period. Ilizarov fixation device should be carefully placed to optimize the clinical and radiographic outcomes of MOWHTO [9. 10]. The Ilizarov device allows the valgus tibia osteotomy to be adjusted in millimeter increments that is required for each patient [11].
The purpose of the present study was to evaluate the clinical and radiographic outcomes after MOWHTO with Ilizarov apparatus with minimum follow up of 5 years.
MATERIALS AND METHODS
This study included 26 knees of 25 consecutive patients with medial unicompartmental osteoarthritis of the knee that was treated with valgus-producing MOWHTO by Ilizarov apparatus between December 2005
and December 2011. Knee osteoarthrosis was clinically diagnosed using the American College of Rheumatology criteria and radiologically derived Kellgren-Lawrence grade was assigned [12, 13].
The inclusion criteria were:
-
a) varus malalignment with medial unicompartmental osteoarthritis of the knee;
-
b) a local chondral lesion of the medial femoral condyle and
-
c) the knee stability.
The exclusion criteria were:
-
a) severe articular damage to the medial compartment with attritional bone loss;
-
b) cartilage lesions of the lateral compartment;
-
c) extensive osteoarthritis (Kellgren-Lawrence 3 or 4) of the patellofemoral joint [13];
-
d) absence or extensive loss of lateral meniscus;
-
e) active knee flexion, < 120º or an extension deficiency exceeding 20º;
-
f) high grade ligamentous instability;
-
g) active local or systemic infection;
-
h) inflammatory arthropathy.
The extent of angular correction was preoperatively measured; we sought to active 6-8º of anatomical valgus on an anteroposterior postoperative weight-bearing radiograph [13]. All patients were preoperatively evaluated both clinically and radiologically, evaluated again at three, six and 12 months postoperatively and annually till 5 years.
Surgical procedure: After spinal anaesthesia under all aseptic precautions one ring was applied at the level of fibular head with three 1.8 biocompatible wires. Out of three wires, two are olive wires. Then the second ring was applied 8–10 cm from the 1st ring with three 1.8 (two olives + one Ilizarov) wires. The 3rd ring was mounted 4 cm from the second ring with 1.8 Ilizarov wires (one olive and two smooth wires).
Then hinges were applied in between the 1st and 2nd ring at the level of osteotomy site, i.e CORA. Under fluoroscopy from the medial side, a small 2 cm stab incision was made and a 5 mm osteotom was placed through the incision in the direction of the fibular head. The medial side of tibia was osteotomized by gradual hammering up to the lateral cortex that must be kept intact. Gradual hinged distraction was applied at the medial side using a diapason graded in millimeters, until the preoperatively calculated distance was attained. The hinge was placed at the level of CORA (Centre of rotation of angulation) at the medial and lateral sides.
Postoperative period : The postoperative rehabilitation period featured isometric quadriceps and range of movement exercises commencing the day after surgery. Patient could partially maintain weight-bearing with the aid of crutches or a walker next day after the surgery and gradually progressed to full weight-bearing.
Clinical assessment : Clinical evaluation of the knee pain was measured using 100-mm visual analogue scale (VAS) (0 mm, no pain, 100 mm worst pain). Pain was evaluated upon walking.
X-ray assessment : Radiographic assessment was done by anteroposterior weight-bearing radiography of the knee, with alignment expressed as the femorotibial angle (FTA) as described previously. Lateral X-ray was taken using a standard technique with the knee in 30º of flexion.
The posterior tibial slope (PTS) angle was calculated using the method of Brazier et al. The Insall-Salvati Index (ISI) was used to measure patellar height.
RESULTS
25 knees of 24 patients were evaluated clinically and radiographically in all the patients. Detailed patient demographics are shown in Table I.
The average follow up period was 5 years.
MOWHTO that breaks the proximal tibia is an extra-articular correction. Hence MOWHTO cannot correct the intra-articular deformity of the knee in patients with severe medial OA.
Table I
Patients characteristics
|
Age |
Mean = 55 (45–62) (range) |
|
Male |
05 |
|
Female |
20 |
|
BMI |
23–32 |
|
Knees (left/right) |
10/15 |
|
Mean osteotomy gap |
8.1 ± 2.0 (range 4–15 mm) |
Case 1:
CASE ILLUSTRATION
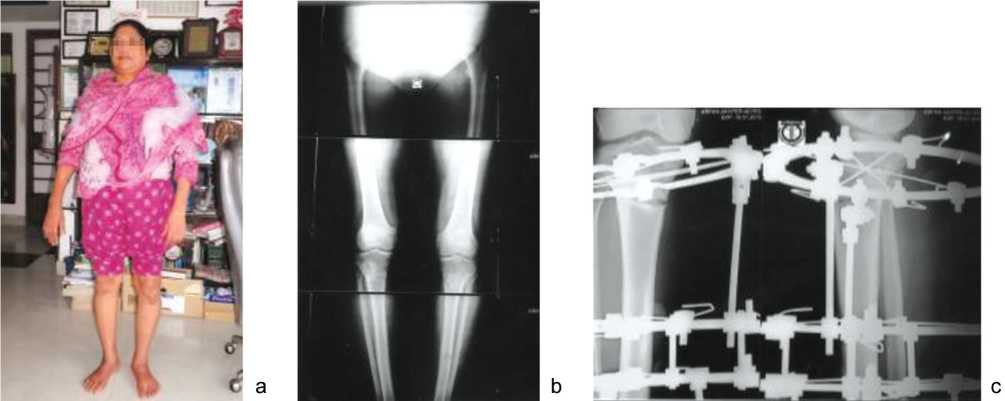
Fig. 1 .: a – bilateral knee OA, Kellgren-Lawrence type III (Ahlback type-III), before surgery; 55 yrs old female with bilateral tibia vara; b – preoperative radiograph of both knees (stress view); c – radiograph of Right knee after surgery with Ilizarov in situ
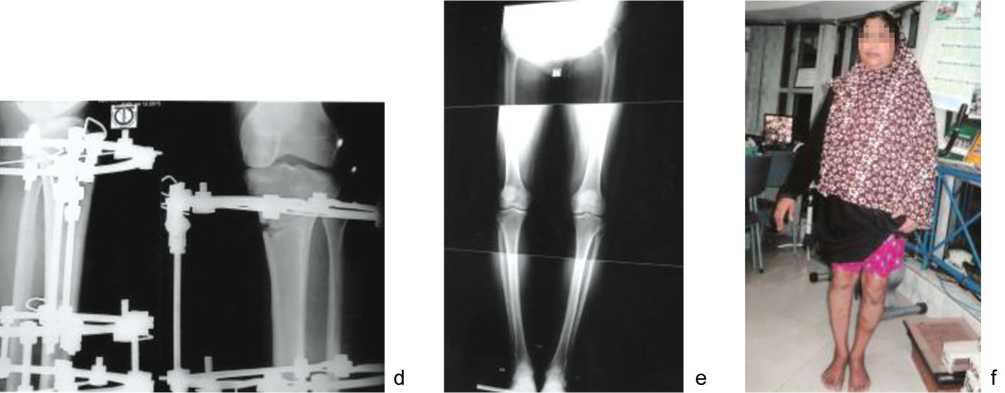
Continuation of Fig. 1 .: d – radiograph of Left knee after surgery with Ilizarov in situ; e – clinical result, radiograph after surgery with good regenerate bone at the osteotomy site; f – clinical appearance of the patient with corrected bilateral tibia vara
Case 2:
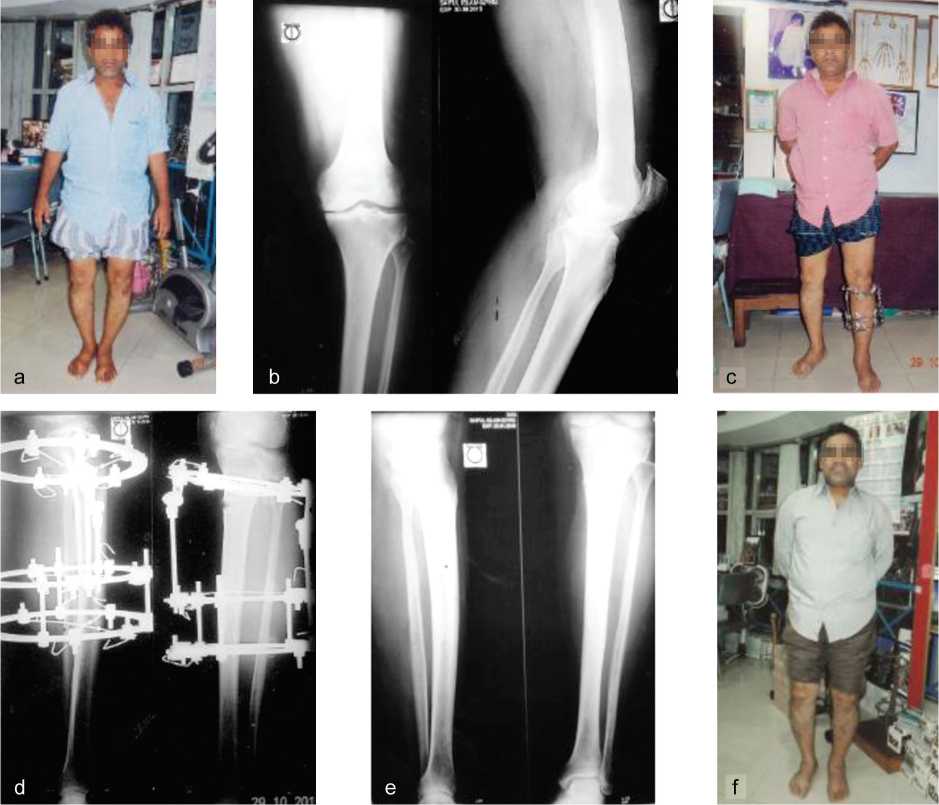
Fig. 2 .: a – bilateral knee OA Kellgren-Lawrence, Ahlback type III; the left knee has greater varus than the right knee; b – AP and lateral views of both knees; c – the patient with Ilizarov fixator in situ in the left knee after correction of knee varus; d – radiograph of left knee after MOWHTO with Ilizarov apparatus on; e – good regenerate is seen at the osteotomy site with correction of varus deformity; f – clinical appearance of the patient after varus correction of the left knee
DISCUSSION
Evaluation of deformities of the lower limbs and principles of deformity correction.
There are two kinds of deformities in the lower limbs: One is intra-articular and the other is extra- articular. We are representing the correction methods used by the principles of Centre of Rotation of angulation (CORA). The corrective osteotomy based on CORA is an entirely extra-articular osteotomy and not an intra-articular one. CORA is usually located at the upper metaphysis of the tibia, and the deformity is usually an extra-articular angular varus deformity. Extra-articular deformities can be corrected acutely by osteotomy or by gradual correction with Ilizarov external fixator based on CORA. Intra-articular deformities cannot be corrected by an extra-articular osteotomy; the intra-articular deformity can only be corrected by an intraarticular osteotomy. The knee of the majority of patients with severe medial OA has intra-articular deformity and some patients have both intra-articular and extra-articular deformities. Intra-articular deformities of the medial OA knee are characterized by cartilage wear, medial subluxation of the medial femoral condyle and the detachment of the lateral articular surface of the proximal tibia. MOWHTO cannot correct these intra-articular deformities because MOWHTO offers only extra-articular correction. So, our conclusion is that when there are intra-articular deformities and extra-articular deformities of the lower limb, these two deformities must be evaluated and corrected individually. In the case of progressed medial compartment OA, the aim of MOWHTO is to transfer the weight bearing axis to the unaffected lateral compartment, in order to reduce pain and to delay the need for knee replacement [14].
The role of MOWHTO in patients undergoing cartilage repair is to provide an optimal biomechanical environment for healing by decreasing the load on the operative site [15, 16].
Unloading of the medial compartment is beneficial in patients with varus malalignment undergoing cartilage repair of the medial compartment [17].
Overload due to malalignment may damage the graft over time, leading to failure [18].
Problems of MOWHTO:
There are no intra-articular deformities at early stage of medial OA; both condyles cause into contact with the articular surface of the proximal tibia simultaneously. MOWHTO is the extra- articular osteotomy chosen to correct this. It is highly recommended for the treatment of mild and moderate OA. Severe medial OA lead to intraarticular deformities. MOWHTO cannot correct this.
CONCLUSION
There are both intra-articular deformities and extra-articular deformities of the lower limb, and these two deformities must be evaluated and corrected individually.
The deformities of severe medial OA are mainly intraarticular deformities and the intra-articular deformity must be corrected first.
References Clinical and radiographic outcomes of medial open wedge high tibial osteotomy (MOWHTO) with Ilizarov technique in OA knee
- Insall J., Salvati E. Patella position in the normal knee joint//Radiology. 1971. Vol. 101, No 1. P. 101-104. DOI: 10.1148/101.1.101.
- Coventry M.B., Ilstrup D.M., Wallrichs S.L. Proximal tibial osteotomy. A critical long-term study of eighty-seven cases//J. Bone Joint Surg. Am. 1993. Vol. 75, No 2. P. 196-201.
- High tibial valgus osteotomy in unicompartmental medial osteoarthritis of the knee; a retrospective follow-up study over 13-21 years/A. Schallberger, M. Jacobi, P. Wahl, G. Maestretti, R.P. Jakob//Knee Surg. Sports Traumatol. Arthrosc. 2011. Vol. 19, No 1. P. 122-127. DOI: 10.1007/s00167-010-1256-4.
- Changes in osteosclerosis of the osteoarthritic knee after high tibial osteotomy/Y. Akamatsu, T. Koshino, T. Saito, J. Wada//Clin. Orthop. Relat. Res. 1997. No 334. P. 207-214.
- Takahashi S., Tomihisa K., Saito T. Decrease of osteosclerosis in subchondral bone of medial compartmental osteoarthritic knee seven to nineteen years after high tibial valgus osteotomy//Bull. Hosp. Jt. Dis. 2002-2003. Vol. 61, No 1-2. P. 58-62.
- Cartilage regeneration after proximal tibial osteotomy for medial gonarthrosis. An arthroscopic, roentgenographic, and histologic study/S. Odenbring, N. Egund, A. Lindstrand, L.S. Lohmander, H. Willén//Clin. Orthop. Relat. Res. 1992. No 277. P. 210-216.
- Fujisawa Y., Masuhara K., Shiomi S. The effect of high tibial osteotomy on osteoarthritis of the knee. An arthroscopic study of 54 knee joints//Orthop. Clin. North Am. 1979. Vol. 10, No 3. P. 585-608.
- Return to sports after valgus osteotomy of the knee joint in patients with medial unicompartmental osteoarthritis // D. Saragaglia, R.C. Rouchy, A. Krayan, R. Refaie // Int. Orthop. 2014. Vol. 38, No 10. P. 2109-2114. DOI: 10.1007/s00264-014-2435-6.
- Opening wedge high tibial osteotomy: plate position and biomechanics of the medial tibial plateau/P. Martinez de Albornoz, M. Leyes, F. Forriol, A. del Buono, N. Maffulli//Knee Surg. Sports Traumatol. Arthrosc. 2014. Vol. 22, No 11. P. 2641-2647. DOI: 10.1007/s00167-013-2517-9.
- Staged medial opening wedge high tibial osteotomy for bilateral varus gonarthrosis: biomechanical and clinical outcomes/E.L. Sischek, T.B. Birmingham, K.M. Leitch, R. Martin, K. Willits, J.R. Giffin//Knee Surg. Sports Traumatol. Arthrosc. 2014. Vol. 22, No 11. P. 2672-2681. DOI: 10.1007/s00167-013-2559-z.
- A new fixation material for open-wedge tibial osteotomy for genu varum/C.H. Ribeiro, N.R. Severino, P. Cury Rde, V.M. de Oliveira, R. Avakian, T. Ayhara, O.P. de Camargo//Knee. 2009. Vol. 16, No 5. P. 366-370 DOI: 10.1016/j.knee.2009.01.007
- The body composition of patients with knee osteoarthritis relationship with clinical parameters and radiographic severity/C. Ertürk, M.A. Altay, C. Sert, A. Levent, M. Yapti, K. Yüce//Aging Clin. Exp. Res. 2015. Vol. 27, No 5. P. 673-679 DOI: 10.1007/s40520-015-0325-4
- Kellgren J.H., Lawrence J.S. Radiological assessment of osteo-arthrosis//Ann. Rheum. Dis. 1957. Vol. 16, No 4. P. 494-502.
- High tibial valgus osteotomy for medial gonarthrosis: a 10-to 21-year study/P. Aglietti, R. Buzzi, L.M. Vena, A. Baldini, A. Mondaini//J. Knee Surg. 2003. Vol. 16, No 1. P. 21-26.
- Minas T., Peterson L. Advanced techniques in autologous chondrocyte transplantation//Clin. Sports Med. 1999. Vol. 18, No 1. P. 13-44, v-vi.
- Parker D.A., Viskontas D.G. Osteotomy for the early varus arthritic knee//Sports Med. Arthrosc. 2007. Vol. 15, No 1. P. 3-14 DOI: 10.1097/JSA.0b013e3180303592
- High tibial osteotomy for unloading osteochondral defects in the medial compartment of the knee/C. Mina, W.E. Garrett Jr., R. Pietrobon, R. Glisson, L. Higgins//Am. J. Sports Med. 2008. Vol. 36, No 5. P. 949-955 DOI: 10.1177/0363546508315471
- Amendola A. Knee osteotomy and meniscal transplantation: indications, technical considerations, and results//Sports Med. Arthrosc. 2007. Vol. 15, No 1. P. 32-38 DOI: 10.1097/JSA.0b013e31802f997b
