Damage control orthopaedics

Author: Bari Mofakhkharul, Islam Shahidul, Shetu Nazmul Huda, Rahman Mahfuzer
Journal: Гений ортопедии @geniy-ortopedii
Section: Случай из практики
Article in issue: 3, 2017.
Free access
Emergency procedures aimed at rapid reduction and fixation and spanning of periarticular fractures has been termed “damage control orthopaedics”. In severely injured patients, early definitive fixation of fractures may not be appropriate. Recent studies showed that in multiple trauma, DCO is the best option for management of patients who are unstable and in extremis. The paper presents a case of such a control in a 34-year-old patient who sustained polytrauma on 20.10.2016. Primary medical care was conducted at a local hospital. Ten hours after the injury, the patient was transported to the Bari-Ilizarov orthopaedic centre for further management. On admission, he was in a traumatic shock. Radiographic study showed a comminuted fracture of the left femur, medial condylar fracture of the ipsilateral femur, comminuted fractures of both bones of the shin, left wrist sprain, and contusion of the head. Osteosynthesis of the left femoral shaft was performed with a Kuntscher nail and additionally with the Ilizarov fixator. When patient’s condition stabilized on the next day, osteosynthesis of the tibia was performed with the Ilizarov apparatus and the wrist was fixed with a plaster cast.
Polytrauma, femur, shaft, tibia, fibula, wrist, fracture, kuntscher nail, ilizarov apparatus
Short address: https://sciup.org/142121980
IDR: 142121980 | UDC: 617-089.844-611.728.2-616.71-001.59 | DOI: 10.18019/1028-4427-2017-23-3-351-353
Ортопедический контроль повреждений при политравме
Неотложные мероприятия с целью быстрого репонирования и фиксации переломов при политравме получили название «ортопедический контроль повреждений». При тяжелой травме окончательное репонирование и фиксацию нецелесообразно проводить сразу. Исследования показали, что ортопедический контроль повреждений является необходимым при лечении пациентов с политравмой, находящихся в нестабильном или тяжелом состоянии. В работе представлен клинический случай применения такого подхода у пациента 34 лет, получившего политравму 20.10 2016 года. Первая помощь была оказана по месту жительства. Через 10 часов после травмы пострадавший был доставлен в ортопедический центр Bari-Ilizarov для дальнейшего лечения. При поступлении пациент находился в состоянии шока, на рентгенограммах определялся оскольчатый перелом левой бедренной кости, перелом медиального мыщелка правой бедренной кости, оскольчатые переломы обеих костей левой голени, перелом левого запястья и ушиб головы. Остеосинтез перелома диафиза бедра выполнен гвоздем Кюнчера с дополнительной фиксацией аппаратом Илизарова. Когда состояние пациента стабилизировалось, остеосинтез костей голени осуществлен аппаратом Илизарова, а перелом запястья зафиксирован гипсовой повязкой.
Text of the scientific article Damage control orthopaedics
Emergency procedures aimed at rapid reduction and fixation and spanning of periarticular fractures has been termed “damage control orthopaedics”.
There was always a debate between early total care (ETC) and damage control orthopaedics (DCO). Early fixation of femoral fractures was shown to have better outcomes and less pulmonary complications. The arguments for early fixation of femoral fractures is to minimize hemorrhage from the fracture site, prevent an ongoing soft tissue damage and minimize a systemic inflammatory activation which reduces secondary lung complications.
Bone et al. (1989) showed in prospective clinical trial that the patients who underwent definitive femoral fracture stabilization within 24 hours of admission to the hospital showed a significant reduction in lung complications when compared to the patients which were delayed [1].
In severely injured patients, early definitive fixation of fractures may not be appropriate.
Pape et al. (2002) showed that in the multiple trauma patients, with chest injury, ETC resulted in more pulmonary complications [2].
The argument for DCO is to minimize the second hit to the systemic inflammatory system which is due to a surgical intervention and is caused by the surgical stabilization of fractures. The majority of authors categorize the multiple injured patients into 4 groups which are:
Recent studies showed that for management of multiple trauma patients, ETC is appropriate in stable and borderline multiple injured patients and DCO is the best option for management of patients in the unstable and in extremis [3, 4].
So, the debate should not be which management is better but which patients would be better treated with either ETC or DCO.
A practical approach is to quantify the physiological response to resuscitation in the multiple trauma patients.
Vallier et al. (2013) applied the term “early appropriate care” [4]. They studied 1442 patients with pelvic, spinal and femoral fractures. The patients underwent comprehensive resuscitation prior to a definitive surgical intervention and fixation. Patients with lactate level < 4.0 mm/l, pH > 7.25 base excess > 5.5 mm/l post resuscitation were safe to proceed with definitive fixation.
Patients, who were not responsive to resuscitation, where the lactate, PH and base excess were worsening, were treated with DCO.
Ш Bari M.M., Islam S., Shetu N.H, Rahman M. Ортопедический контроль повреждений при политравме // Гений ортопедии.
CONCLUSION
ETC and DCO have their place in the management of multiple trauma patients. Comprehensive resuscitation is mandatory for improving end-organ hypoperfusion.
Case presentation
Patient M. H., 34 years old male, sustained an injury on 20.10.2016 at 11:00 am in Bogra district, 205 km from Dhaka. He was taken to Bogra Medical College Hospital where he got primary management by plaster and antibiotics and 2 units of blood (900 ml). Then, he was referred to Dhaka for better management. I received the patient at my BARI-ILIZAROV ORTHOPAEDIC CENTRE, Dhanmondi, Dhaka at 09:00 pm. After the proper anamnesis had been taken, I did all investigations accordingly. Then, the patient was taken to OT for further management. X-rays showed:
-
1. Comminuted shaft fracture of the left femur;
-
2. Medial condylar fracture of the ipsilateral femur (was found by fluoroscopy in OR);
-
3. Comminuted fracture of the left tibia with comminuted fracture of the left fibula G IIIA;
-
4. Left wrist sprain;
-
5. Contusion of the head.
The patient was in a shock. BP was: 70/60 mm of Hg. Pulse was 140/minutes. 2 units (900 ml) of blood was transfused per operatively and 2 units (2 liters) of Hartmann’s Solution (Sodium Chloride: BP 0.6 % w/v, Potassium Chloride: BP 0.04 % w/v, Calcium Chloride: BP 0.027 % w/v, Sodium Lactate: USP 0.32 % w/v) intravenously infused.
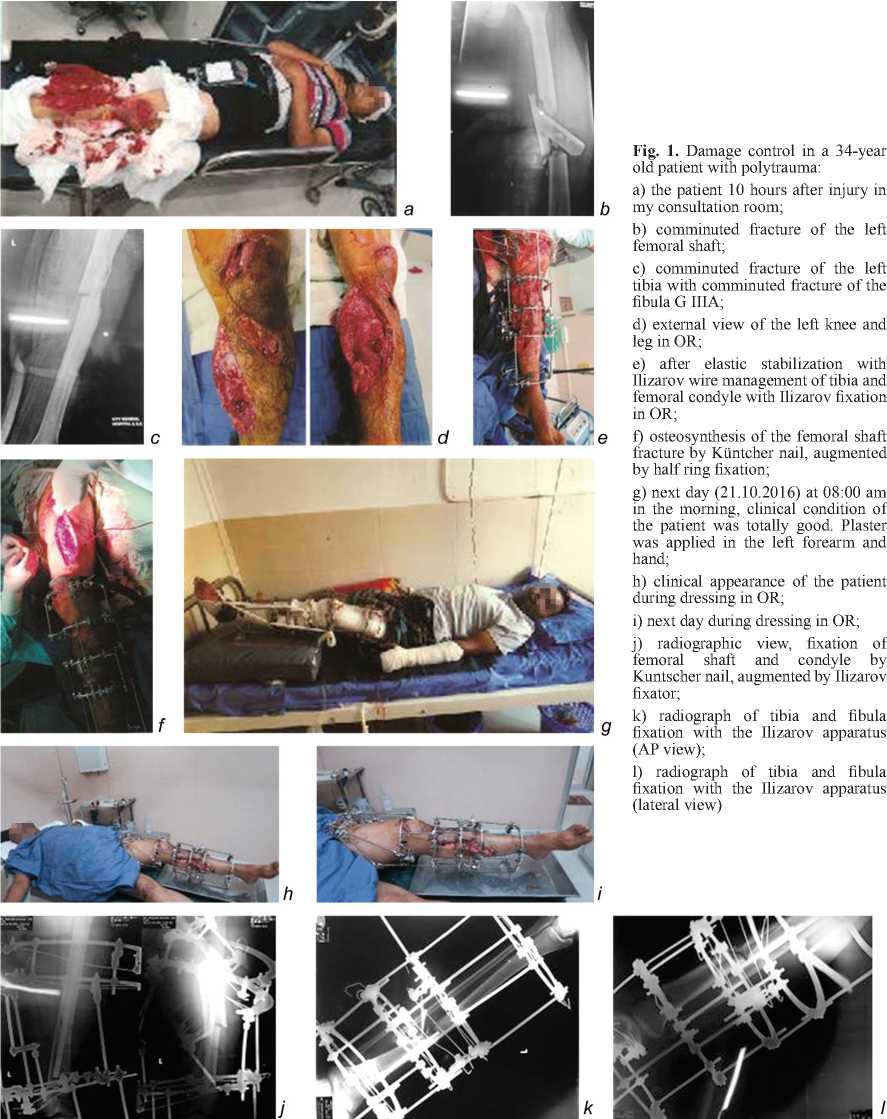
Fig. 1. Damage control in a 34-year old patient with polytrauma:
a) the patient 10 hours after injury in my consultation room;
b) comminuted fracture of the left femoral shaft;
c) comminuted fracture of the left tibia with comminuted fracture of the fibula G IIIA;
h) clinical appearance of the patient during dressing in OR;
i) next day during dressing in OR;
j) radiographic view, fixation of femoral shaft and condyle by Kuntscher nail, augmented by Ilizarov fixator;
k) radiograph of tibia and fibula fixation with the Ilizarov apparatus (AP view);
l) radiograph of tibia and fibula fixation with the Ilizarov apparatus (lateral view)
d) external view of the left knee and leg in OR;
e) after elastic stabilization with Ilizarov wire management of tibia and femoral condyle with Ilizarov fixation in OR;
f) osteosynthesis of the femoral shaft fracture by Küntcher nail, augmented by half ring fixation;
g) next day (21.10.2016) at 08:00 am in the morning, clinical condition of the patient was totally good. Plaster was applied in the left forearm and hand;
ь
е
References Damage control orthopaedics
- Early versus delayed stabilization of femoral fractures. A prospective randomized study/L.B. Bone, K.D. Johnson, J. Weigelt, R. Scheinberg//J. Bone Joint Surg. Am. 1989. Vol. 71, No 3. P. 336-340.
- Changes in the management of femoral shaft fractures in polytrauma patients: from early total care to damage control orthopedic surgery/H.C. Pape, F. Hildebrand, S. Pertschy, B. Zelle, R. Garapati, K. Grimme, C. Krettek, R.L. Reed 2nd//J. Trauma. 2002. Vol. 53, No 3. P. 452-461.
- Borderline femur fracture patients: early total care or damage control orthopaedics?/B. Nicholas, L. Toth, K. van Wessem, J. Evans, N. Enninghorst, Z.L. Balogh//ANZ J. Surg. 2011. Vol. 81, No 3. P. 148-153 DOI: 10.1111/j.1445-2197.2010.05582.x
- Timing of orthopaedic surgery in multiple trauma patients: development of a protocol for early appropriate care/H.A. Vallier, X. Wang, T.A. Moore, J.H. Wilber, J.J. Como//J. Orthop. Trauma. 2013. Vol. 27, No 10. P. 543-551 DOI: 10.1097/BOT.0b013e31829efda1
