Modern features of diagnosis and treatment of thoraco-abdominal injuries

Author: Khodzhimatov Gulomidin M., Yakhyoev Sardorbek M.
Journal: Cardiometry @cardiometry
Section: Original research
Article in issue: 26, 2023.
Free access
The improved algorithm of the diagnosing and treatment tactic of thoracoabdominal injuries can allows for timely diagnosis and the choice of adequate treatment tactics. The important role and opportunities of the endovideosurgical technologies are revealed in the diagnosis and surgical management of patients with thoracic and abdominal trauma. The results of diagnostics and treatment of patients with thoracoabdominal injuries using the diagnostic and treatment tactic algorithm improved by the authors were analyzed. The use of the offered diagnostic and treatment algorithm has improved the results of treatment of this severe category of patients. The clinical effectiveness of minimally invasive methods of the treatment and diagnosing of the thoracoabdominal injury is average 1.1 times higher than traditional surgical approaches
Traumatic injuries of the chest and abdominal cavity, laparoscopy, thoracoscopy
Short address: https://sciup.org/148326602
IDR: 148326602 | DOI: 10.18137/cardiometry.2023.26.98104
Text of the scientific article Modern features of diagnosis and treatment of thoraco-abdominal injuries
Gulomidin M. Khodzhimatov, Sardorbek M. Yakhyoev. Modern Features of Diagnosis and Treatment of Thoraco-abdom-inal Injuries. Cardiometry; Issue No. 26; February 2023; p. 98104; DOI: 10.18137/cardiometry.2023.26.98104; Available from:
Early diagnosis and treatment of patients suffer with thoracoabdominal injuries is one of the most difficult problems of emergancy surgery. In the condition of modern technological progress, the prevalence of chest and abdominal trauma, including thoracoabdominal trauma, reaches up to 40% of all injuries. At the same time, most difficulties of diagnosing and surgical management of this type of trauma characterized by ambiguous results in treatment due to the severity of the patients. [1].
Mortality from traumas ranks second in the general structure of mortality of Commonwealth of Independent States (CIS) and it is one of the main factors in its depopulation [4]. According the authors, the number of deaths in the group of combined injuries of the thoracic and abdomen exceeds mortality in isolated injuries by 7-8 times [9].
In recent years, thoracoabdominal injuries increased due to the criminal situation, the growth of traffic accidents, natural disasters, terrorist attacks, riots and military conflicts and this is the main cause of death of group of working-age people. There is still a high level of diagnostic and tactical errors in the treatment of this category of patients because of severity of the patient’s condition which majority of damage to various organs accompanied by large blood loss and shock, masking the symptoms of damage to the organs of the thoracic and abdominal cavities, drug or alcohol intoxication, often observed in these patients [5, 6].
The results of surgical treatment of patients with thoracoabdominal injuries are determined by a number of objective indicators. Among them, the most important are the number of postoperative complications and their structures [12, 14]. As well as, the volume of intraoperative blood loss affect the improvement of the patient’s condition. This circumstance indicates the need for revision of emergency surgical approaches and diagnostic procedures of the injuries of thoracic and abdominal cavity organs, as well as using minimally invasive surgery, in parallel with anti-shock measures.
The choice of rational surgical tactics is still controversial and the issues of using endoscopic methods of diagnosis and treatment of this category of victims are insufficiently covered [3, 7, 11]. Due to the lack of unified tactical guidelines for conducting diagnostic and treatment tactics, optimal methods of diagnosis and treatment are always chosen, which leads to both belated surgical interventions and an unjustified expansion of the scope of operations [2, 3, 13]. A large number of postoperative complications – up to 50% and high mortality – 15.9-49.5% [8, 10] dictate the need to generalize the accumulated experience, tactical and technical additions to the classification and surgical measures of suffered from thoracoabdominal injuries.
For this reason, the aim of study is improving the quality of medical care for patients with thoracoabdominal injuries at the hospital stage through the evolution and implementation of a treatment and diagnostic algorithm, as well as widely using of endovid-eosurgical methods of diagnosis and treatment into clinical practice.
Patients and methods
Over a 6-year period, between January 2017 and December 2022, the records of all patients aged 18 years and above, managed for thoracic and abdominal injury at the Andizhan branch of the Republican Scientific Center for Emergency Medical Care, were reviewed. Recordings of 122 (64.86%) patients (in the control group were treated from 2017 to 2020) with thoracoabdominal injuries were retrospectively analyzed, in which the diagnostic and therapeutic stages were carried out according to the generally accepted scheme. The main group included 65 (35.14%) patients managed from 2021 to 2022 using by the improved diagnostic and surgical tactical algorithm applying minimally invasive technologies (fig. 1.).
The age of the patients ranged from 18 to 88 years. The largest group of patients consisted of patients aged 19 to 30 years – 73 people (38.4%). There were 3.2 times more male patients than female patients – 76.3% versus 23.7% (tab. 1.).
Hospitalized patients with thoracoabdominal injuries (n=190)
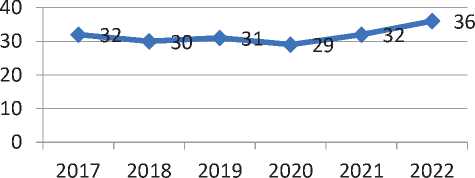
Hospitalized patients with thoracoabdominal injuries (n=190)
Figure 1.Distribution of hospitalized patients with thoracoabdominal injuries by years.
According to the time of admission, 48 (25.26%) victims were delivered in the first hour from the moment of injury, 93 (48.94%) patients were delivered from 1 to 3 hours, 16 (8.42%) patients were delivered from 3 to 6 hours, later 6 hours – 31 (16.3%), the time was not set for 2 (1.05%) admitted.
In the structure of the mechanism of injury, stab wounds prevailed – in 97 (51%) patients; ruptures with bruises in road traffic accidents – in 49 (26%) patients, wounds with fragments of ribs in case of a closed injury – in 44 (23%) (fig. 2.).
Depending on the predominance of one or another symptomatology, three groups of patients with different damage characteristics were clearly distinguished: 1) the first group – these are patients with a predominance of symptoms of damage to the thoracic organs – 66 (34.7%); 2) the second group – patients with a predominance of symptoms of damage to the abdominal organs – 91 (47.9%); 3) the third group – patients with the same complexity, injuries of the organs of the thoracic and abdominal cavities – 33 (17.4%) (fig. 3.).
Table 1
Age and gender distribution of patients
|
Group |
Gender |
Age of patients |
Total: |
|||||||
|
19-30 |
31-40 |
41-50 |
51-60 |
61 и ст. |
||||||
|
Control group |
m |
N |
38 |
20 |
18 |
11 |
9 |
96 |
122 |
64,2% |
|
% |
20 |
10,5 |
9,5 |
5,7 |
4,7 |
50,5 |
||||
|
f |
N |
8 |
6 |
6 |
2 |
4 |
26 |
|||
|
% |
4,2 |
3,1 |
3,1 |
1,0 |
2,1 |
13,7 |
||||
|
Main group |
m |
N |
19 |
13 |
8 |
5 |
4 |
49 |
68 |
35,8% |
|
% |
10 |
6,84 |
4,2 |
2,66 |
2,1 |
25,8 |
||||
|
f |
N |
8 |
4 |
2 |
2 |
3 |
19 |
|||
|
% |
4,2 |
2,1 |
1,0 |
1,0 |
1,7 |
10 |
||||
injury mechanism
23%
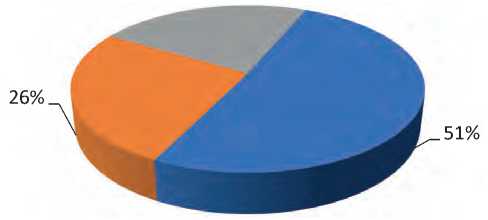
■ stab wounds
■ ruptures with bruises in an accident
■ wounds by fragments of ribs in blunt trauma
Figure 2.Structural distribution of victims with thoracoabdominal wounds according to the types of injury.
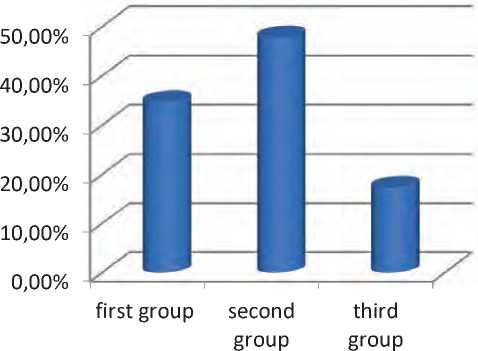
Figure 3.Characteristics of the symptoms of patients with thoracoabdominal injuries.
Thoracic and abdominal X-ray examination was performed in the X-ray room of the admission department, or in the operating room using X-ray. This afforded to identify to severity of damage, exception of extremely serious patients. In parallel, diagnostic medical sonography of the organs of the abdominal and pleural cavities, and the pericardium was performed to accurate diagnose the dominant damage. The results of the clinical characteristics, radiography of the chest and abdominal organs, primary surgical treatment and revision of the wound channel, sonography of the chest and abdominal organs, allowed us to determine the surgical tactics and surgical access in 90% of cases.
Endoscopic study included diagnostic and treatment laparoscopy, thoracoscopy and fibrogastrodu-odenoscopy. Laparoscopy and thoracoscopy made it possible, on the basis of direct and indirect signs, to confirm with great certainty not only the presence of 100 | Cardiometry | Issue 26. February 2023
blood in the abdominal cavity, and also to establish the source of bleeding, thereby determining the indications for surgery on the abdominal organs and surgical interventions. One of the leading diagnostic methods was emergency thoracoscopy, which performed in 12 (6.3%) patients on admission and in 2 (1.1%) patients in the postoperative period for the diagnosis and treatment of emerging complications.
Injuries of the gastrointestinal tract were detected and diagnosed by fibrogastroduodenoscopy (FGDS) in 13 (6.8%) patients. Basically, FGDS was performed for suspected injuries and ruptures of the hollow organs of the gastroduodenal zone, both in the preoperative period and in the intraoperative period.
Magnetic spiral computed tomography was also used to clarify the diagnosis in cases that were in stable patients and could not be diagnosed by traditional diagnostic methods.
All patients underwent general blood and urine tests upon admission to the hospital. The remaining laboratory tests (electrolytes, prothrombin time, coagulogram, blood clotting time, blood enzymes, control of the general analysis of blood and urine) were carried out individually during the patient’s hospitalization.
At admission 59 (31%) patients were in a state of shock of the first degree, 21 (11%) – of the second degree, 31 (16.3%) – of the third degree. The severity of the concomitant injury was assessed by the injury severity scale Injury Severity Score (ISS), in the control group it was 17.8±4.9 points, in the main group 18.2±4.2.
RESULTS AND DISCUSSION
Clinical experience has shown that in order to choose the most rational treatment with the consistent use of surgical and conservative measures, a classification and a specific treatment and diagnostic algorithm of actions are necessary, which serve as a guide to the action of practitioners. According to the algorithm, patients with thoracoabdominal injuries in all cases undergo a revision of the wound channel, followed by primary surgical debridement (PSD). It should be noted that the revision of the wound channel was carried out in the conditions of the emergency department in order to determine the penetration of the wound into the cavity. With a penetrating nature, PSD was performed in the operating room. It was carried out in parallel with resuscitation, during anesthesia. To diagnose the dominant damage to the organs of the abdominal and pleural cavity, ultrasound, X-ray of the organs of the chest and abdominal cavity were performed, endoscopic research methods were used, which made it possible to determine the surgical and operative approach in 90% of cases.
Injuries to the internal organs revealed in the patients were also of a different nature. As can be seen from Table 2, the most frequent injuries were observed in the following organs: lungs, liver, spleen, omentum, stomach and large vessels. In our patients, injuries of the lung and stomach, liver, small and large intestines were more often combined with a multiple nature of the injury (tab. 2.).
Various surgical interventions were performed in all patients. Operational tactics depended on the nature and severity of the injury, the general condition of the victims. The volume of surgical interventions and approaches in patients with thoracoabdominal injuries and the amount of damage were performed by the following combinations of approaches: (tab. 3.)
From the data of the table it follows, first of all, thoracotomy, and then laparotomy – 13 (6.8%); thora-
Table 2
The nature of damage to internal organs
|
Nature of damage |
Кол-во |
% |
|
Without damage |
17 |
8, 9 |
|
Injury of the arteries of the chest wall |
27 |
14, 2 |
|
Pericardial/heart injury |
3 |
1, 6 |
|
Injury/injury to the lung |
42 |
22, 1 |
|
Diaphragm injury/trauma |
13 |
6, 8 |
|
Injury/injury to the liver (capsule rupture, superficial wound up to 3 cm long and up to 1.5 cm deep, massive damage – detachment of the lobe) |
31 |
16, 3 |
|
Injury/trauma of the spleen (rupture of the capsule, damage to the pole, damage to the hilum) |
23 |
12, 1 |
|
Injury/injury of the stomach (inertial rupture of the visceral peritoneum of the stomach) |
16 |
8, 4 |
|
Injury/trauma of the small intestine (non-tensioned hematoma of the mesentery, rupture of the visceral peritoneum of the intestine, separation of the intestine from the mesentery, direct wound) |
6 |
3, 2 |
|
Injury/injury of the colon (mesenteric hematoma, serosa rupture, mesenteric avulsion, direct injury) |
11 |
5, 8 |
|
Gallbladder injury |
2 |
1, 1 |
Table 3
The nature of surgical interventions and accesses
|
№ |
Type of access and scope of surgical intervention |
Control group |
Main group |
||
|
Number of injured |
Quantity patients in % |
Number of injured |
Quantity patients in % |
||
|
1 |
Thoracotomy followed by laparotomy |
9 |
4,7 |
4 |
2,1 |
|
2 |
Thoracophrenotomy |
2 |
1,1 |
3 |
1,6 |
|
3 |
Laparotomy and drainage of the pleural cavity without thoracotomy |
18 |
9,5 |
7 |
3,7 |
|
4 |
The first step is laparotomy, the second step is thoracotomy. |
9 |
4,7 |
2 |
1,1 |
|
5 |
Simultaneous thoracotomy and laparotomy |
2 |
1,1 |
1 |
0,5 |
|
6 |
Thoracophrenolaparotomy |
1 |
0,5 |
||
|
7 |
Laparotomy |
38 |
20 |
16 |
8,4 |
|
8 |
Thoracotomy |
10 |
5,2 |
3 |
1,6 |
|
9 |
Laparoscopy |
1 |
0,5 |
10 |
5,2 |
|
10 |
Thoracoscopy |
0 |
0 |
8 |
4,2 |
|
11 |
Drainage of the pleural cavity without thoracotomy |
18 |
9,5 |
12 |
6,3 |
|
12 |
PSD |
13 |
6,8 |
2 |
1,1 |
|
Total: |
122 |
64,2 |
68 |
35,8 |
|
cotomy and frenotomy – 5 (2.6%), respectively; laparotomy and drainage of the pleural cavity without thoracotomy – 25 (13.2%), the first stage was laparotomy, the second – thoracotomy – 11 (5.8%), thoracophre-nolaparotomy – 1 (0.5%). Simultaneous thoracotomy and laparotomy was performed in 3 (1.6%) patients. At the same time, in 19 (10%), the operation was completed using a minimally invasive approach, without thoraco- or laparotomy. At the same time, it was possible to take in defects of both various organs and the diaphragm. Before the applying of endovideosurgical methods of treatment, drainage of the pleural cavity was conducted at the thoracic stage of the operation in 8 (4.2%) patients. Indications for thoracotomy in this category of patients were established in cases of suspected injury to the heart or large vessels, or with continued bleeding.
It should be noted that in all cases, in the course of performing diagnostic thoracoscopy and laparoscopy, regardless of the detection or absence of damage to the internal organs of the abdominal and thoracic cavity, false-negative results were not obtained.
Thoracic organ pathologies were not detected, when performing of the diagnostic thoracoscopy 6 (3.2%) with thoracoabdominal trauma, which was confirmed during the observation patients and compiled a true negative result.
When massive intrapleural bleeding in case of a stab wound of the thorax and multiple lung injury, during the performance of 2 (1.1%) diagnostic thoracoscopies was indication for conversion of the open operative approaches. The described causes of massive bleeding were identified only during thoracotomy, and did not allow visualization of these injuries during endovideosurgical diagnostic surgery. As well as, emergency thoracoscopy performed in 12 (6.3%) patients on admission and in 2 (1.1%) patients in the postoperative period for the diagnosis and treatment of emerging complications.
Analyzing data of study in the use of endovideo-surgical technologies for the diagnosis and treatment of patients with thoracoabdominal injury (intraoperative, postoperative complications, mortality) and the results of operations using thoracotomy or laparotomy made it possible to reveal the degree of clinical effectiveness of endovideosurgical techniques. Consequently, 18 (9.5) % operations were recognized as effective out of 19 performed endovideosurgical diagnostic and treatment approaches, mortality is not noticed. In the 2nd group of patients operations performed through open surgical access, in 38 cases (31.2%) were recorded complications of the total number of operations of 2nd group patients (control group) there were recorded complications and in case 9 (7.4%) deaths observed. The clinical efficacy of en-dovideosurgical diagnostic and surgical managment is on average 1.1 times higher than that of interventions through open surgical access.
The data obtained indicate a high degree of effectiveness of the method of endovideosurgical diagnostics in thoracoabdominal trauma. The analysis of the obtained results made it possible to determine that endovideosurgical diagnostic methods for thoracoabdominal trauma provide, on average, 1.09 times higher level of sensitivity, 1.68 times higher level of specificity and 1.16 times higher level of accuracy. The frequency and structure of postoperative complications in comparison by groups is shown in Figure 4.
A good clinical effect was achieved as a result of the treatment of patients in the main group of patients with the use of endovideosurgical interventions. So in the postoperative period, the pain syndrome was less pronounced, there was no need for long-term observation and treatment in the intensive care unit and resuscitation. In addition, the rates of postoperative complications decreased by 32% (including early complications by 26.1% and late ones by 5.9%), a good cosmetic effect, the average hospital stay was reduced by 4.3 ± 0.34 bed-days, and decreased postoperative mortality by 11.7%. There was no cosmetic defect on the chest and abdominal wall.
One of the main indicators of the outcome of treatment is mortality, which amounted to 25.6%. 7 (6.4%) people died from shock, 13 (10.6%) from multiple organ failure, 5 (4.1%) from pulmonary embolism (tab. 4.).
Table 4
Causes of mortality in thoracoabdominal injuries
|
№ |
Causes of death |
Main group(n=) |
% |
Control group (n=) |
% |
|
1 |
Traumatic, hemorrhagic shock |
1 |
1,5 |
6 |
4,9 |
|
2 |
Multiple organ failure |
5 |
7,3 |
8 |
6,5 |
|
3 |
Pulmonary embolism |
2 |
2,9 |
3 |
2,5 |
|
TOTAL |
8 |
11,7 |
17 |
13,9 |
|
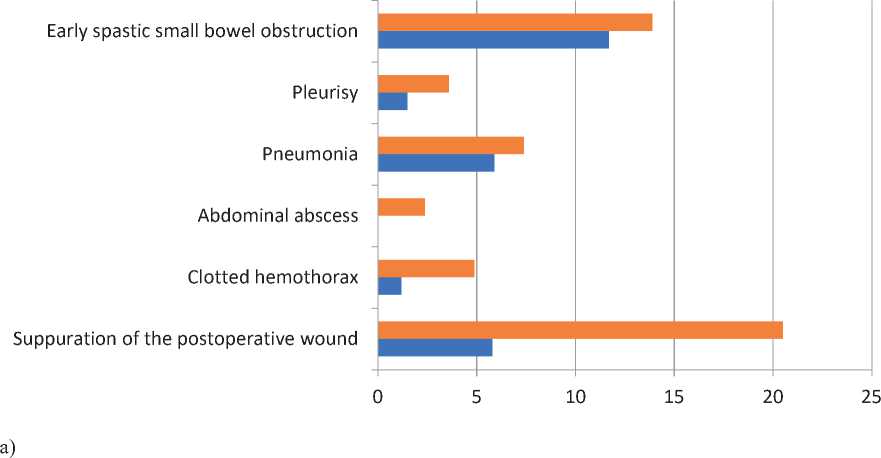
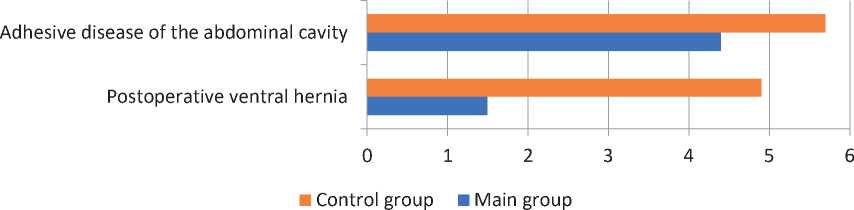
b)
Figure 4.Complications of surgical treatment of patients with thoracoabdominal injuries. a) early postoperative complications; b) late postoperative complications.
The success of any type of surgical treatment for thoracoabdominal injuries is determined by a number of indicators. The most important among them are: the volume of blood loss, the number of postoperative complications and their structure, the mortality rate, as well as the duration of inpatient treatment, which reflects the economic aspect of this problem. Therefore, the improved diagnostic and treatment algorithm can be used in the diagnosis and treatment of patients with thoracoabdominal injuries.
Conclusion
Applying in practice developed diagnostic and treatment algorithm using minimally invasive surgical methods allows to reducing the number of unreasonable laparotomies (5.2%) or complication and traumatism of result of open surgical operation. As well as, clinical effectiveness of endovideosurgery in diagnosing and surgical management of thoracoabdominal injury is average 1.1 times higher than the traditional diagnostic and treatment methods.
References Modern features of diagnosis and treatment of thoraco-abdominal injuries
- Alizhanov AA, Iskhakov BR, Iskhakov NB. The place of endovideosurgery in the diagnosis and treatment of patients with emergency pathology and injuries of the abdominal organs: 20 years of experience of the Namangan branch. Journal of Emergency Medicine 2021;14(6):31-35 https://doi.org/10.54185/TBEM/vol14_iss6/a5
- Alishikhov AM, Bogdanov DY, Matveev NL. Experience in the use of endovideosurgical technologies in the diagnosis and treatment of thoracoabdominal trauma. Endoscopic Surgery 2010;5:7.
- Amarantov DG, Zarivchatsky MF., Svetlakov AV. The role and place of intracavitary endoscopy in the treatment of thoracoabdominal wounds. Health of Tajikistan 2017; 4:5–10.
- Amarantov DG, Zarivchatsky MF, Kholodar AA, Gudkov OS, Kolyshova EV. Modern approaches to the surgical treatment of thoracoabdominal wounds. Bulletin of Surgery 2018;177(5):100-103. doi: https://10.24884/0042-4625-2018-177-5-100-104
- Degtyarev OL., Sitnikov VN., Turbin MV, Demin KA. Thoracoabdominal wounds in emergency surgery. Bull. St. Petersburg. university Ser.11: Medicine. 2010. App. : Pirogov. Surgical week: Materials of the All Russian 2010;669–670.
- Khadzhibaev AM, Shukurov BI, Altiev BK, Kuchkarov OO. Surgery of thoracoabdominal wounds: 15 years of experience in one clinic. Bulletin of Emergency Medicine 2019:12(4):9-16
- Khadzhibaev FA, Elmuradov GK, Mansurov TT, Shukurov BI, Elmuradov KS. Possibilities of ultrasound in assessing the nature and severity of closed abdominal trauma. Bulletin of Emergency Medicine 2021;14(6):14-19. http://doi.org/10.54185/TBEM/vol14_iss6/a2
- Cherkasov MF.Surgical tactics for combined injuries of the abdominal organs.Congress of Surgeons of the Southern Federal District, 2nd: Materials. Pyatigorsk; 2009;72–73.
- Cherkasov MF, Degtyarev OL, Sarkisyan VA. Urgent videothoracoscopy for injuries of the chest organs with multiple and combined trauma. Kuban Scientific Medical Bulletin 2012;3(132):195-199
- Amini A, Latifi R. Laparoscopic-assisted minithoracotomy for repair of diaphragmatic penetrating trauma.Surg. Laparosc. Endosc. percutan. Tech. 2013; 23:406-409.
- Matsevych OY, Koto MZ, Motilall SR, Kumar N. The roleof laparoscopy in management of stable patients with penetrating abdominal trauma and organ evisceration. J TraumaAcute Care Surg 2016;8:307–311.
- Moore EE, Knudson MM, Burlew CC, et al; WTA Study Group. Defining the limitsof resuscitative emergency department thoracotomy: a contemporary Western Trauma Association perspective. J Trauma. 2011;70(2):334-339.
- Trejo-Avila ME, Valenzuela-Salazar C, Betancourt- FerreyraJ, Fernandez-Enriquez E, Romero-Loera S, Moreno-PortilloM. Laparoscopic versus open surgery for abdominal trauma:A case-matched study. J Laparoendosc Adv Surg Tech A 2017;27:383–387
- Yahyoev SM., Khodzhimatov GM. Diagnostic methods and surgical treatment of patients with thoracoabdominal traumas (review of the literature).Kardiochirurgia i Toracochirurgia Polska 2022; 19(4):226-231. doi: https://doi.org/10.5114/kitp.2022.122093
