Nature and structure of thoracoabdominal injuries

Author: Khodzhimatov G. M., Yakhyoev S.M.
Journal: Cardiometry @cardiometry
Section: Original research
Article in issue: 22, 2022.
Free access
This article presents the incidence, nature and structure of thoracoabdominal injuries in two major districts of the Andijan region. The results of diagnostics, tactics of treatment, and also an estimation of severity of a condition of patients with thoracoabdominal traumas are resulted. An analysis of mortality is presented.
Thoracoabdominal injuries, mortality, iss scale
Short address: https://sciup.org/148324586
IDR: 148324586 | DOI: 10.18137/cardiometry.2022.22.128132
Text of the scientific article Nature and structure of thoracoabdominal injuries
Gulomidin M. Khodzhimatov*, Sardorbek M. Yakhyoev. Nature and structure of thoracoabdominal injuries. Cardiome-try; Issue 22; May 2022; p. 128-132; DOI: 10.18137/cardiome-try.2022.22.128132; Available from: issues/no22-may-2022/nature-and-structure
Despite the large number of studies devoted to the problem of thoracoabdominal injuries, there are still many unresolved questions. Mortality in thoracoabdominal injuries varies from 3.13 to 20% [1,3,4]. The main causes of death in thoracoabdominal trauma are acute blood loss, shock, peritonitis, and respiratory distress syndrome [3,9]. Postoperative complications in thoracoabdominal injuries occur in 14.9-53% of patients [8]. Difficulties in timely diagnosis of this pathology are due to the polysymptomatic clinical picture, the severity of the injured, the lack of specific symptoms of diaphragm injury, and the presence of concomitant injuries of the thoracic and abdominal cavities [5,9]. Chest and abdominal injuries cause severe disorders of basic vital functions of the body immediately at the time of injury and within minutes after 128 | Cardiometry | Issue 22. May 2022
it. The presence in the thoracoabdominal region of the human body of the main vital organs, major vessels, the specificity of anatomical structure, the proximity of intestinal contents and enzymes in injuries leads to massive internal bleeding, shock, cardiorespiratory disorders and purulent-septic complications [2,5,11]. More than in any other injury thoracoabdominal trauma requires accurate and prompt diagnosis, thought-out and adequate surgical tactics, the ability to predict the dynamics of pathological changes occurring in parenchymatous organs and gastrointestinal tract, operations are complicated and labor-intensive, the outcomes depend on the terms of surgical intervention, the need for careful management of the patient in the postoperative period. The peculiarities of modern traumatism are an increasing proportion of severe combined injuries, a combination of injuries to several anatomical areas, aggravating the course of traumatic disease, which often leads to fatal outcome [7,10]. And also, monitoring the prevalence of thoracoabdominal injury in the population with an assessment in dynamics of risk factors, causes of development, survival rate, diagnosis and approaches to surgical treatment is a topical problem of modern medicine, which allows to study the epidemiological situation regarding thoracoabdominal injuries and requires continued search for optimal diagnostic measures and choice of correct surgical tactics at all stages of treatment.
Purpose of work: To study the incidence, nature and structure of thoracoabdominal injuries in the adult population of two major districts of the Andijan region in the period from 2017 to 2021.
Material and methods We studied case histories and medical records of 188 victims with concomitant injuries delivered to the sub-branches of the Emergency Department of the RRCEMP (EMS) of Balykchi and Shahrikhan districts of Andijan region in the period from 2017 to 2021. Of the total number of victims - 44 persons with thoracoabdominal injuries. Of them 19 (43,2 %) were hospitalized in Balykchy 25 (56,8 %) and Shakhrikhan EMP.
All patients admitted with thoracoabdominal injuries were assessed for the severity of injuries using the ISS scale. To diagnose the patients, clinical-laboratory and instrumental studies (ultrasound, radiography, and multispiral computed tomography) were performed.
The nature of instrumental examination and the sequence of their performance were determined based on the specific clinical situation. Instrumental examinations were used both to confirm and document the nature of chest and abdominal injuries and to diagnose other complications of trauma, concomitant diseases, and the degree of compensation for the functions of various organs and systems (Table 1).
Table 1
Volume of instrumental examinations
|
Type of examination |
In the Shakhrikhan CEMP |
In Balykchy CEMP |
|
Chest X-ray |
25 |
19 |
|
Abdominal X-ray |
25 |
19 |
|
Thoracic ultrasound |
20 |
10 |
|
Abdominal ultrasound |
25 |
19 |
|
Thoracoscopy |
- |
- |
|
Laparoscopy |
- |
- |
|
Computed tomography |
13 |
9 |
|
Total |
108 |
76 |
The magnitude of acute blood loss confirming the diagnosis of traumatic shock was judged by systolic blood pressure (SBP), pulse rate, number of erythrocytes per mm3 of blood, hemoglobin, and hematocrit. In the absence of arterial hypotension (BP over 90 mm Hg), traumatic shock was not included in the formulation of the diagnosis. These data were taken from the medical histories of the victims and the accompanying vouchers filled out by the ambulance doctors.
The database on the victims was created in Microsoft Office Excel 2010 (Microsoft, USA). Based on the database created, statistical analysis was performed using the BioStat 2009 application software package (AnalystSoft Inc., USA). All victims were included in the study by the continuous method.
Study Results. The data and analysis show that in 2017-2021 in Shakhrikhan district 96 patients with various concomitant injuries were hospitalized, including 25 (26,04%) with thoracoabdominal injuries, in Balykchi district 92 patients with concomitant injuries were under observation, including 19( 20,65%) patients with thoracoabdominal injuries. Initially, we studied the prevalence of thoracoabdominal injuries over a 5-year period. In 2017-2018, 5 patients were hospitalized in Shahrikhan district, 4 patients in 20192020, and 7 patients in 2021. In Balykchy district 2 patients were hospitalized in 2017-2018, 4 and 1 in 2019 and 2020 respectively, and 10 patients in 2021 with. This shows that both districts had the highest number of hospitalized patients in 2021 (Fig.1).
The vast majority of patients in Shakhrikhan Emergency Department (SHEMP) received chest and abdominal injuries as a result of traffic accidents, which amounted to -14 (56%) of observations. The second place was occupied by criminogenic injuries - 7 (28 %) of observations, and the third place, fall from height -4 (16 %) of observations. The difference between the causes of pathology in patients in Balykchy EMP is not large, i.e. traffic accidents - in 7(36.8%) patients, falls from height in second place - in 6 (31.6%), criminogenic injuries (stabbing and beating) - in 5 (26.3%) and 1 (5.3%) case of thoracoabdominal injury associated with work activities (Fig. 2).
There were 34 (77.2%) male and 10 (22.8%) female victims. Most of the victims, 37 (84.1%), were between the ages of 22 and 60, i.e., of working age (Table 2).
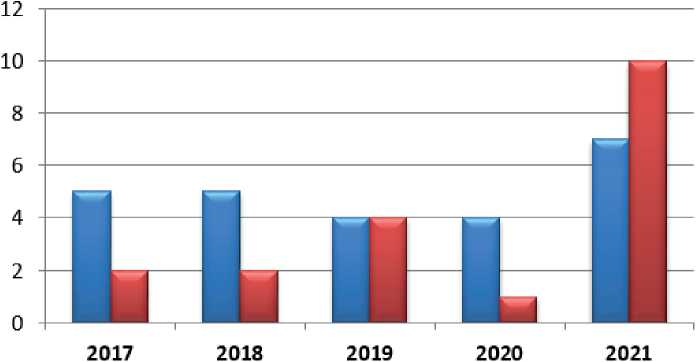
И Shakhrikhan district
и Balykchy District
Figure 1. Frequency of patients with thoracoabdominal trauma.
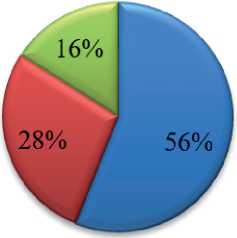
и traffic accident
ы criminogenic injuries
J drop from height
5,30%
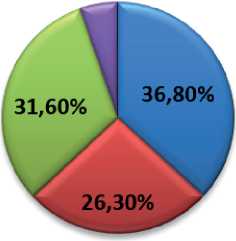
b) in Balykchi EMP
a traffic accident m criminogenic injuries a drop from height
M related to production
a) in Shakhrikhan EMP
-
Figure 2. Distribution by causes of thoracoabdominal trauma
Table 2
Distribution of patients with thoracoabdominal trauma by sex and age, n (%)
|
Indicator |
In the Shakhrikhan CEMP |
In Balykchy CEMP |
|
Men |
21(84%) |
13(68,5%) |
|
Women |
4(16%) |
6(31,5%) |
|
Age, years |
||
|
16-21 |
- |
1(5,2%) |
|
22-35 |
7 (28%) |
7(36,9%) |
|
36-60 |
14 (56%) |
9(47,5%) |
|
61-75 |
3(12%) |
1(5,2%) |
|
Over 75 |
1(4%) |
1(5,2%) |
Upon admission to the emergency department, all the victims (n = 44) were evaluated for the severity of injury according to the ISS scale; the total number of ISS scores was distributed as follows: less than 17 - 9 (20.5%), 17-25 - 15 (34.1%), 26-40 - 14 (31.8%), over 40 - 6 (13.6%), i.e. in most cases thoracoabdominal injuries were of severe form.
Posttraumatic shock was observed in 40.9% (18) cases. Of these, 7 (15.9%) patients had I-II degree of shock, and 7 (15.9%) had III degree and 4 (9.1%) victims had terminal shock. The development of traumatic shock of II-III degree was noted in the majority of the victims.
Among the major complications, the following were most frequently observed: hemorrhage - 34.1%, embolism (fat and air) - 20.75%, and associated infection - 15.24% . Of 44 victims, 18 (40.9%) were operated on. On admission, the condition of the victims was severe or extremely severe due to massive blood loss and shock. In all cases, there were emergency indications for surgery.
Depending on localization of injury and extent of injury, the following combinations of accesses were performed: thoracotomy first and then laparotomy in 3 (6.81%) cases, respectively; laparotomy and draining of pleural cavity simultaneously in 8 (18.18%) cases; laparotomy first, thoracotomy second in 5 (11.36%); thoracotomy and laparotomy simultaneously in 2 (4.54%) patients. Thoracotomy was indicated in suspected cardiac injury and hemothorax up to the fifth rib as well as translocation of greater omentum into pleural cavity. In 8 cases (18.18%) pleural cavity drainage was performed after surgery. Laparotomy was performed on all patients admitted for diagnostic and therapeutic purposes. The most frequent indication for laparotomy was abdominal bleeding.
The severity of the condition dictated strict requirements for the choice of accesses, their sequence and the volume of interventions. The results of surgical treatment of patients with thoracoabdominal injuries depended on the sequence of interventions in order to perform hemostasis as quickly as possible. Staging and sequence of interventions was based on the determination of bleeding priority according to chest X-ray and ultrasound of abdominal, pleural and pericardial cavities, which does not contradict the literature data [2]. Thoracotomy was performed initially with obvious signs of ongoing intrapleural bleeding and absence of gross symptoms of abdominal organ damage. It was indicated by large (more than 1000 ml) and progressive (more than 300 ml per hour) hemothorax with positive Rouvillois-Gregard test. In the clinical picture of abdominal injuries laparotomy was performed first. As a rule, pleural cavity drainage according to Bühlau was performed simultaneously with the control of blood release through drains. Tho- racotomy was performed as the second stage in case of continuous bleeding and massive air drainage - it was anterior-lateral thoracotomy at - 6 and 7 intercostal space.
The most severe group consisted of patients with concomitant, equal in complexity abdominal and thoracic injuries - 10 (22.7%). Laparotomy and thoracotomy by two teams were performed simultaneously in 2 (4.54%) patients; in 8 (18.18%) patients thoracotomy and laparotomy were performed stepwise or vice versa. During postoperative period the patients received intensive care in intensive care unit: artificial lung ventilation, blood components and blood substitutes transfusion, prevention of purulent-septic complications. As the condition stabilized, patients were transferred to the surgery department for further treatment and discharge from the hospital. The average duration of a bed-day was 12.
Complications in the postoperative period were observed in 12 (27,27%) patients: suppuration of the postoperative wound - 6 (13,63%), postoperative bleeding - 1 (2,27%), most frequently there were pulmonary complications in the form of hypostatic pneumonia (5 cases - 11,36%). Especially it was noted in elderly people. Four (9.09%) patients died in the postoperative period. The main causes of death were shock, severe blood loss, various purulent-septic complications. All intrapleural purulent complications developed in patients who underwent only pleural cavity drainage.
In fact, the deceased patients with thoracoabdominal injuries were young and of working age, which confirms numerous literature data on the social significance of thoracoabdominal trauma problem.
Thus, analysis of the results of a retrospective study of patients with thoracoabdominal injuries shows that most of the injuries were the result of transport trauma, and men predominated. The ISS score was 25.
Conclusions
-
1. Thoracoabdominal injuries accounted for 23.4% with various co-injuries, and these types of injuries tend to increase.
-
2. In the structure of thoracoabdominal traumatism in the adult population of two large districts of the Andijan region, 21 (47,7%) were victims with thoracoabdominal injuries as a result of transport trauma. Most of the patients were men (77.2%) of working age.
-
3. surgical treatment for thoracoabdominal injuries should be started from the area of the greatest
-
4. severity of trauma over 25 points according to the ISS scale was diagnosed in half of the victims. Shock of various degrees in 40,9% of cases. Bleeding was noted in 34,1% of cases and embolism (fat and air) in 20,75% of cases. Postoperative mortality in thoracoabdominal injuries was 9.1% of hospitalized patients.
injury, i.e. thoracotomy or laparotomy. Laparotomy is performed with simultaneous drainage of the pleural cavity according to Bulau.
Statement on ethical issues
Research involving people and/or animals is in full compliance with current national and international ethical standards.
Conflict of interest
None declared.
Author contributions
The authors read the ICMJE criteria for authorship and approved the final manuscript.
References Nature and structure of thoracoabdominal injuries
- Abakumov MM. Surgery of combined chest and abdominal wounds: 30-year experience. Tuberculosis and pulmonary diseases. 2010;87(11):17-23. [in Russian]
- Bagdasarova YA, et al. Peculiarities of surgical tactics in left-sided stabbing-cutting-thoracic-abdominal wounds. Thoracic and cardiovascular surgery. 2006(4): 63-6. [in Russian]
- Bagnenko SF, et al. Combined lesions of the chest, accompanied by shock (diagnostics, surgical tactics and treatment). St. Petersburg: I.I. Janelidze Research Institute of Emergency Medicine. I.I. Janelidze, 2006. 160 p. [in Russian]
- Ermolov AS, et al. Diagnostics and treatment of posttraumatic coagulated hemothorax. Surgery. 2006;1:22-8. [in Russian]
- Zhestkov KG. Thoracoscopic surgery. The modern state of the issue: successes, problems, prospects. Review of materials presented at the VII congress of ROEC. Мoscow, 2005. 19 p. [in Russian]
- Kukushkin AV. Thoracoabdominal Wounds. Bulletin of Ivanovo Medical Academy. 2011;16(1):39-45. [in Russian]
- Maksin AA, et al. Principles of diagnostics and surgical treatment of victims with thoracoabdominal trauma. [in Russian]
- Styazhkina SN, et al. Main methods of treatment and prevention of complications in thoracoabdominal traumas. Causes of lethality in thoracoabdominal traumas. Modern innovations. 2018;6(28). [in Russian]
- Topchiev MA, Plekhanov VI, Kolegova AS, Alibekov RS. Treatment of thoracoabdominal injuries. Acta Biomedicacientifica. 2011;42:194-96.
- Gao JM, et al. Traumatic diaphragmatic rupture with combined thoracoabdominal injuries: difference between penetrating and blunt injuries. Traumatol. 2015; 18(1): 21-6.
- Kones O, et al. Is nonoperative approach applicable for penetrating injuries of the left thoracoabdominal region. Turk. J. Emerg. Med. 2016; 16:22-5.
