Новая методика чрескожной кортикотомии при удлинении конечностей и коррекции деформаций

Автор: Ариаманеш A., Гарехдахи M., Алхаосави M., Омидикашани Ф.
Журнал: Гений ортопедии @geniy-ortopedii
Рубрика: Оригинальные статьи
Статья в выпуске: 3, 2011 года.
Бесплатный доступ
Предпосылки: Правильное проведение кортикотомии очень существенно при удлинении конечностей и коррекции дефор- мации методом дистракционного остеогенеза. В настоящее время используются разнообразные методики кортикотомии/ остеотомии, но они не внушают достаточной уверенности относительно сохранения эндостального кровообращения и избежания повреждения надкостницы. В этой статье мы представляем новый простой и эффективный метод кортикото- мии. Методы: Это исследование проводилось в Медицинском Университете Мешхеда (Иран) в период с июня 1995 года по сентябрь 2009 года. У 22 пациентов (24 конечности), являвшихся кандидатами на проведение удлинения конечностей с коррекцией деформации или без нее, одновременная кортикотомия проводилась новым методом, который мы наглядно представляем в этой статье. Результаты: Случаев преждевременной консолидации не было. В 19 конечностях рентгено- логическое образование мозоли отмечалось в конце третьей недели, у всех наших пациентов - в конце четвертой недели. Оценки функции у пациентов и оценки удовлетворенности были лучше при посттравматических укорочениях и деформа- циях конечности по сравнению с врожденными нарушениями. Заключение: Кортикотомия при применении нового метода является простой в исполнении, более уверенной и предсказуемой, способной предупредить нежелательные повреждения кости и сохранить как периост, так и эндост.
Кортикотомия, остеотомия, надкостница (периост), эндост, илизаров
Короткий адрес: https://sciup.org/142121463
IDR: 142121463 | УДК: 616.717/718-007.24-001.5-089.85
A novel technique of percutaneous corticotomy for limb lengthening and deformity correction
Background: correct corticotomy is essential in limb lengthening and deformity correction by distraction osteogenesis. Currently a variety of corticotomy /osteotomy techniques are used but do not make enough confidence about preserving endosteal circulation and avoidance of periosteal damage. We introduce a new simple and efficient corticotomy method in this paper. Methods: This study was undertaken in Mashhad Medical University-Iran from June 1995 till September 2009. In 22 patients (24 limbs) who was candidate for limb lengthening with or without correction of deformity, simultaneous corticotomy was performed by a new method which we explain it descriptively in this paper. Results: There was not any premature consolidation. 19 limbs had radiologic callus formation at the end of 3rd week and in all of our patients at the End of 4th week. Patient functional scores and analogue satisfaction scores were better in post traumatic limb shortening and deformities in comparison to congenital disorders. Conclusion: Corticotomy with this new method is a simple, more confident and predictable one which can prevent undesirable bone cracks and preserve both periosteum and endosteum.
Текст научной статьи Новая методика чрескожной кортикотомии при удлинении конечностей и коррекции деформаций
Ilizarov developed the technique of distraction osteogenesis to regenerate large deficiencies in bone. Distraction osteogenesis is induced locally by a special corticotomy and controlled externally by a ring fixator. One of the factors that affect the process of callus distraction in limb lengthening is the type of osteotomy [1–4].
A finely performed corticotomy is so important to the success of distraction osteogenesis, so many open osteotomies have evolved but they gradually abandoned as was proved to be traumatic to osteogenic elements of bone [5, 6]. Although a variety of percutaneous osteot omy and corticotomy methods [8, 11-13], or a combination of an open partial subperiosteal cortical osteotomy followed by manual osteoclasis of the remainder of the bone cortex [1], have been introduced in the literature but all of them look to be time consuming and difficult to control.
A corticotomy can be complicated which these complications include incomplete corticotomy, damage to osteogenic elements through rough surgical technique (lead to delay in callus formation) and displacement of the fragments after corticotomy [10].
We have lengthened 24 limbs in 22 patients with congenital or post traumatic limb shortening or bone deformities (11 post traumatic limb shortening, 3 proximal femoral focal deficiencies, 4 fibula hemimelia, 5 limb shortening secondary to physeal arrest and one bone tumor for reconstruction after tumoral resection) [fig. 1, 2].
-
14 patients were male and 8 were female subjects, with mean age of 26. 3 years (8–42). The shortened or deformed limb were 13 right-sided, 9 left-sided, and two bilateral. The
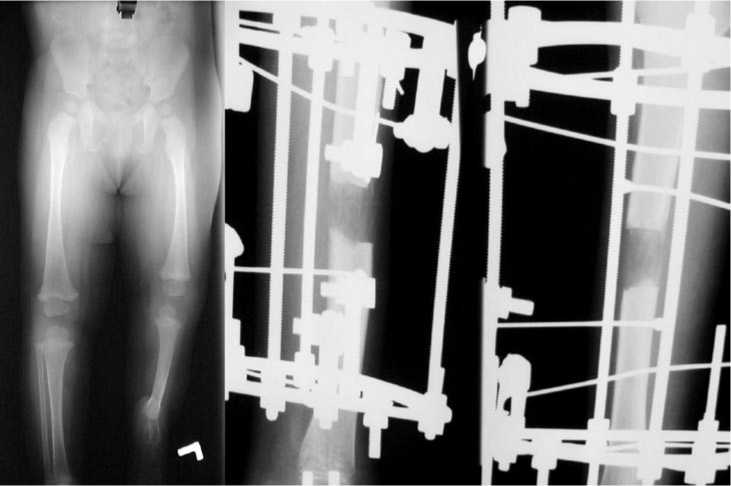
Fig. 1. case 1. A 9 years old girl with left terminal paraxial fibula hemimelia with 78 mm shortening on scanogram, one level and one stage bone lengthening was performed, with our novel technique, fantastic call formation at the end of 5th week
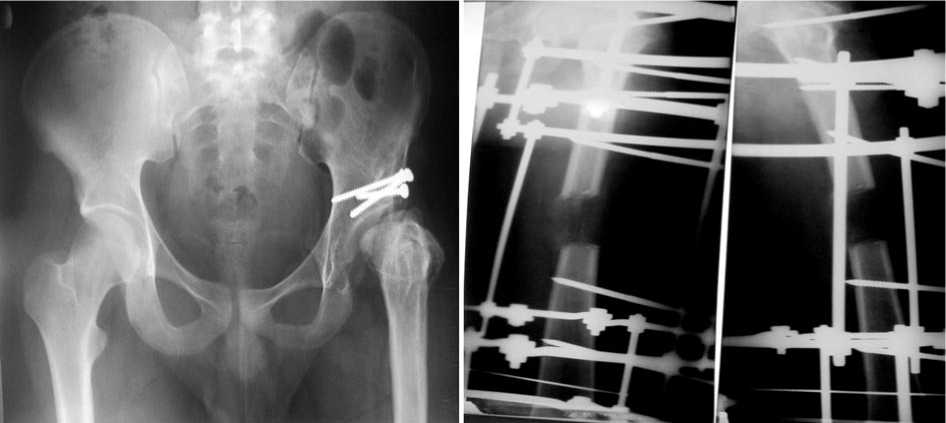
Fig. 2. Case 2. A 22 years old man with history of left hip septic arthritis at age 5, and secondary proximal femoral physeal arrest with 5. 67 cm shortening in scanogram. One stage and one level true corticotomy (with our novel method) was performed, the hip subluxation was managed after device removal by periacetabuar osteotomy
-
2. Through the osteotomy the extended lateral column of osteotome places out side of bone and prevents slipping
-
3. Obliquity of the osteotome edge itself prevent slipping of the osteotome to the outside of bone and prevents periosteal damage too.
average of limb length discrepancy was 5. 32 cm (4. 1–8. 3), the site and exact amount of discrepancy was determined in all patients with CT-Scanogram. 18 patients underwent proposed lengthening and / or correction of the bone deformities through a single treatment procedure and in 4 patients through 2–3 procedures. In 20 patients (21 limbs) a single level corticotomy was performed and in 2 patients (3 limbs), double level corticotomy was established.
In all 24 limbs corticotomy was performed by our new technique which is explained descriptively in surgical method section.
Surgical Method:
After inserting the lengthening / corrective device (Ilizarov, orthofix), the corticotomy site is approached with regard to preoperative planning for lengthening. We prefer corticotomy at the site of angular deformity or as close as possible to the apex of deformity (usually meta- physo-diaphyseal or diaphyseal), but for pure shortening we prefer to do corticotomy on the metaphyseal region. The periosteum is incised in a «H-shape manner». For better exposures we use routinely from a head lamp and mini fragment set retractors. We create very gently a hole by a pneumatic drill on the exposed bone and we use a specific step wise osteotome, the commercial kinds of these osteotomes can be find in rhinoplasty sets [fig. 3]. Cement removal osteotomes can be used but they are high profile and their usage should be restricted for large limbs with wider cortex.
The rhinoplasty osteotomes are so fine, they have a lateral column and the osteotome end edge is oblique itself. The advantages of these osteotomes for corticotomy are: 1. They are fine and can be used by small incisions.
of the osteotome to the medullary canal and damaging of the endosteum (especially if the size of the osteotome edge be the same as the cortical diameter).
After creating the hole, this hole is used as a starting point for insertion of the osteotome and the corticotomy is completed circumferentially (for each 180 degree cor-ticotomy, curved left and curved right osteotomes can be used — fig. 3).
After 7 days of latency period we initiate distraction with a controlled rate and rhythms of distraction 0. 25 mm, four times a day.
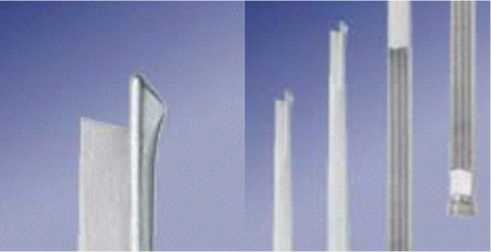
Fig. 3. Rhinoplasty osteotomes in 3 different sizes, straight, curved left and right
RESULTS
There was radiologic callus formation in 19 limbs at the end of 3rd. week and in all of our patients at the end of 4 weeks. There was not any premature consolidation in none of 22 patients. 4 patients needed second and third procedure for managing pin track infection, iliotibial band release and correcting the lengthening device. One patient experienced radicular pain in the limb which was managed by decreasing the rate of daily distraction.
Patient functional scores and analogue satisfaction scores were better in post traumatic limb shortening and deformity in comparison to congenital disorders (87 % and 90 % versus 72 % and 81 %). The average final limb length discrepancy was 1. 83 cm. None of our procedures was complicated by delayed union or non-union.
DISCUSSION
Respecting the soft tissue and bone marrow circulation is one of the main principals In orthopedic surgery [7, 14] and this will be more important in managing some complex cases with the Ilizarov technique [9] which they have specific complexity and unpredictable results themselves and the addition of some complications like nonunion, delayed union, premature consolidation of osteotomy / corticotomy site can make the treatment plan more complex.
The importance of correct corticotomy with the Ilizarov technique has been emphasized in so many studies [1, 2]. In a study by Frierson M, et al. on 15 dogs, the authors demonstrated that there was a significant difference in union times between corticotomy, multiple drill hole osteotomy, osteotomy with oscillating saw. In the latter group they reported delayed radiological callus formation till 10 Week after surgery [3].
The factors that correlate with callus formation during limb lengthening by the Ilizarov method were investigated by Yasui N, et. al. They concluded that the most important factor is correct corticotomy following by starting to distraction after a safe latency period [4].
Kajimoto H, et. al. on an animal model (27 rats) emphasized the importance of periosteal and endosteal preserving during corticotomy for leg lengthening by callus distraction method [5].
In an experimental study the effect of different osteotomy methods on bone regeneration was evaluated. Five methods of subcutaneous corticotomy, open corticotomy, Cattaneo corticotomy, open osteotomy and osteoclasis on 35 sheeps in 7 groups — each contained 5 sheeps — were compared according to roentgenogram, morphological examination (bone sections, histological evaluation, superficial X-ray). In all of the cases the gaps were filled with regenerated bone but in bone section analysis and histological slides the most advanced osteogenesis process was on osteoclasis group. On SEM examination and X-ray microanalysis the mineralization of new bone on osteoclasis group had more similarity with healthy bone than other groups [6].
Usage of unreliable methods of corticotomy in the Ilizarov method, condemned of keeping more latency period for minding about union of the site in future [7, 14], on the other hand prolonged latency period can lead to premature consolidation which may need returning the patient to hospital and operating teater to revising the procedure.
We emphasize that for achieving satisfactory results for most of orthopedic procedures paying sufficient attention to details, respecting soft tissues and preserving of bone circulation are really important and it will be more important during corticotomy / osteotomy in handling complex disorders with the Ilizarov technique. We believe that usage of this technique for corticotomy is a real and fantastic method on considering all of this details and preserving both endosteum and periosteum during procedure, on the other hand because of high reliability it does not need a prolonged latency period and capable the surgeons to starting bone distraction after 7 days. At the end we introduce this method as the gold standard for bone corticotomy in orthopedics.
REF
-
1. Schwatsman V., Schwartsman R. Corticotomy // Clin. Orthop. Relat. Res. 1992. Vol. 280. P. 37–47.
-
2. The role of corticotomy and osteotomy in the treatment of bone defects using the Ilizarov technique / R. Brutscher [et al. ] // J. Orthop. Trauma.
1993. Vol. 7, No 3. P. 261–269.
-
3. Frierson M., Ibrahim K., Boles M. Distraction osteogenesis. A comparison of corticotomy techniques // Clin. Orthop. 1994. Vol. 301. P. 19–24.
-
4. Factors affecting callus distraction in limb lengthening / N Yasui [et al. ] // Clin. Orthop. 1993. Vol. 293. P. 55–60.
-
5. Bone lengthening in rabbits by callus distraction. The role of periosteum and endosteum / H. Kojimoto [et al. ] // J. Bone Jt. Surg. 1988. Vol. 70-B, No 4. P. 543–549.
-
6. Experimental studies on the effect of osteotomy technique on the bone regeneration in distraction osteogenesis / A. Krawczyk [et al. ] // Bone. 2007. Vol. 40, No 3. P. 781–791.
-
7. Alonso J. E., Regazzoni P. Bridging bone gaps with the Ilizarov technique. Biologic principles / Clin. Plast. Surg. 1991. Vol. 18, No 3. P. 497– 504.
-
8. A technique of percutaneous multidrilling osteotomy for limb lengthening and deformity correction / N. Yasui [et al. ] // J. Orthop. Sci. 2000. Vol. 5, No 2. P. 104–107.
-
9. Ilizarov G. A. The tension–stress effect on the genesis and growth of tissues. Part I. The influence of stability fixation and soft tissue preservation // Clin. Orthp. Relat. Res. 1989. Vol. 238. P. 249–281.
-
10. Radiological imaging of the formation of regenerated bone in distraction osteogenesis: an experimental study / A. Krawczyk [et al. ] // Orthop. Traumatol. Rehabil. 2002. Vol. 4, No 3. P. 290–298.
-
11. A comparison of two osteotomy techniques for tibial lengthening / L. Eralp [et al. ] // Arch. Orthop. Trauma Surg. 2007. Vol. 124, No 5. P. 298– 300.
-
12. The influence of osteotomy technique on distraction osteogenesis / A. Krawczyk [et al. ] // Clir. Narzadow Ruchu. Orthop. Pol. 2001. Vol. 66, No 6. P. 535–543.
-
13. Monticelli G., Spinelli R. Leg lengthening by closed metaphyseal corticotomy // Ital. Orthop. Traumatol. 1983. Vol. 9, No 2. P. 139–150.
-
14. Pan S. C. Application of Ilizarov's external fixator on the basis of biology // Zhonghua Wai Ke Za Zhi. 1991. Vol. 29, No 5. P. 296–297.
Рукопись поступила 06. 06. 11.
