On the patient’s influence on the postoperative healing process: an experimentum crucis

Author: Kofler W., Glazachev O. S.
Journal: Вестник Международной академии наук (Русская секция) @vestnik-rsias
Section: Медико-биологические науки
Article in issue: 1, 2025.
Free access
In a followup study conducted from 1950 onwards, significant and relevant differences in mortality were found among survivors of the atomic bombs in Hiroshima and Nagasaki who had been exposed to the same levels of radiation, with or without additional physical damage. This was unexpected, as it had been assumed that five years after surviving the somatic damage, both groups would be classified as part of the normal population and that both had been exposed to identical levels of radiation.W. Kofler assumed that each person has a limited ability to organize healing processes. The group with additional physical damage from the atomic bombs then differed from the group without these additional demands. Different results were therefore to be expected. It was inadmissible to draw conclusions about the generalizability of the data from the survivors of Hiroshima and Nagasaki. However, the chosen approach also corresponded to that of an «Experimentum crucis» (F. Bacon). In this case, the paradigm that took into account limited organizational capacity proved to be more effective than the one that did not. This should have had farreaching consequences. However, these could be avoided by relying on an argument based on the current state of knowledge. Since radiation exposure is based on quantum effects, predictions would only be possible for large numbers (populationbased approach). For individual cases, however, the uncertainty principle must be taken into account. It would therefore be worth discussing whether the epidemiologically proven assumption of the usefulness of only limited organizational capacity can be transferred to a capacity that every individual possesses. This objection can only be addressed in a case study. The present study demonstrates the greater significance of a view of the current state of knowledge that is expanded to include limited organizational effectiveness regarding biological and psychophysiological processes, e.g. in wound healing. It had been predicted that the healing process in individual lung cancer surgery would be faster if the patient was able to temporarily suspend competing processes that are not currently needed and that require the use of organizational capacity. The relevance of managing individual capacity to organize homeostatic functions is demonstrated in the described clinical case study.
Experimentum crucis, ability to organize, healing processes, individual
Short address: https://sciup.org/143184538
IDR: 143184538
О влиянии пациента на процесс послеоперационного заживления: решающий эксперимент
В ходе проспективного исследования, проводившегося с 1950 года, были обнаружены значительные и существенные различия в смертности среди людей, переживших атомные бомбардировки в Хиросиме и Нагасаки, которые подверглись одинаковому уровню радиации, с дополнительными физическими повреждениями или без них. Это было неожиданно, поскольку предполагалось, что через пять лет после пережитых соматических повреждений обе группы будут отнесены к относительно здоровому населению, поскольку все жертвы подверглись одинаковому уровню радиации. В. Кофлер в своей теории «расширенного взгляда на человека…» предположил, что каждый индивидуум обладает ограниченной способностью организовывать процессы заживления. Поэтому пострадавшие дополнительными физическими повреждениями от атомных бомбардировок отличалась от группы без этих дополнительных стрессоров и следовало ожидать иных результатов более тяжелых последствий катастрофы в этой группе. Очевидно, недопустимо делать выводы об обобщенности данных, полученных от выживших в Хиросиме и Нагасаки. Тем не менее, выбранный подход также соответствовал эксперименту «Experimentum Сrucis» (Ф.Бэкон). В данном случае парадигма, учитывающая ограниченные организационные возможности индивидуума, оказалась более эффективной, чем «классический» подход «доза - эффект». Это должно было иметь далеко идущие последствия. Однако их можно было избежать, опираясь на аргументы, основанные на современном уровне знаний. Поскольку радиационное воздействие основано на квантовых эффектах, предсказания возможны только для больших чисел (популяционный подход). Для отдельных случаев, однако, необходимо учитывать принцип неопределенности. Поэтому стоит обсудить, можно ли эпидемиологически доказанное предположение о пользе «управления» ограниченного потенциала организовывать гомеостаз перенести на потенциал, которым обладает каждый человек. Это положение может быть рассмотрено только в конкретном исследовании (критический эксперимент). Настоящее исследование демонстрирует бo´льшую значимость взгляда на актуальное состояние знаний, которые«расширяются» и должны включать в себя понятие об ограниченных индивидуальных возможностях организовывать биологические и психофизиологические процессы, например, при заживлении ран. Было предсказано, что процесс заживления при индивидуальной операции по удалению рака легкого пойдет быстрее, если пациент сможет временно приостановить не нужные в данный момент процессы, требующие использования индивидуальных организационных возможностей. Релевантность управления индивидуальными возможностями организации гомеостатических функций продемонстрирована в описанном клиническом случае.
Text of the scientific article On the patient’s influence on the postoperative healing process: an experimentum crucis
The importance of intellectual, emotional and cognitive effects on health, illness and the need for recreation is undisputed in modern medicine. However, it is particularly challenging that it is not only impossible to observe the abilities that cause intellectual, emotional and cognitive effects. We are used to this from energetic effects: we cannot observe ‘forces or energy fields’, but only their effects (such as changes in position in space) or the energy carriers from which forces can be drawn (such as petrol). However, our conception of the nature of natural objects, to which we therefore assign unobservable forces or fields, enabled us to formulate predictions for precisely characterizable empirical studies in order to test our inventions about the nature of objects. The success of the predictions confirmed the usefulness of our thought constructs. This shows how the theory about the nature of the objects under investigation and the methods used to examine and evaluate them are interdependent. This ‘philosophical’ foundation of natural science, which Einstein called ‘theory,’ is the prerequisite for developing empirical methods to test whether the assumptions are correct or not [3]. Thus, theory determines what we can observe (Einstein), but also what we cannot observe (Heisenberg). Theory also determines what conclusions we can draw from phenomena. What is true for energetic effects must also be true for non-energetic effects.
However, implementing this in research into intellectual, emotional and cognitive processes is particularly challenging for outsiders because the effects to be demonstrated are only observable and therefore accessible to natural science if they also lead to observable, i.e. energetic-material effects. As everyone knows from their own experience, it is possible to withhold one's own, far-reaching conclusions from others. Such determinations can, but do not necessarily, lead to behavioral changes or trigger classic stress reactions. They can only take place ‘internally’ and then lead to unexpected pathophysiological effects in cells or tissues, which are therefore not investigated. The latter group of effects in particular has hardly been researched in this regard. This is partly because doctors give their patients medication to trigger a specific observable effect. They therefore change the medication if the expected effect does not occur. We therefore assume that in practice it would be sufficient to assume a machine-like effect between stimulus and biological effect. But allergies should serve as a warning: cells are clearly capable of evaluating and autonomously changing their evaluation. And we know from placebos that unconscious evaluation processes can trigger a cascade of biochemical reactions in a person that correspond to the effects of drugs.
W. Kofler therefore assumes that biological systems, whether single cells or individuals, obviously have two ways of becoming effective, like Janus: ‘energetic-material’ and ‘non-energetic-meaning-related’. He assumes that both types are like the two sides of a coin, representing two characteristics of one and the same ability. Since one side enables energetic effectiveness (‘energy’) and the other side enables non-energetic, meaning-related effects, which in living beings corresponds to the ability to organize, the ability to organize, like energy, can only be available to a limited extent, just as the coin is limited. If we assume that every biological process must be organized properly and that the organizational capacity required for this is only available to a limited extent, then every process must also have a non-specific effect. It ties up organizational resources that would otherwise be available for other processes. This leads to health-related consequences: an additional requirement must therefore lead to a less favorable outcome, e.g. a worsening of existing symptoms/homeostatic disturbances, than without this additional requirement. If, on the other hand, it would be possible to artificially reduce the organizational requirement, this would have to lead to a more favorable outcome than without this intervention. The proposed consideration of organizational capacity thus represents a fundamental extension of the previous paradigm. However, its usefulness had to be proven empirically and logically [10].
Proving the paradigm. W. Kofler evaluated various studies of environmental disasters, which showed that all environmental disasters did not only lead to the specific effects of the environmental pollutants that occurred [9]: For example, the London smog of 1952 with extreme SO 2 and dust levels led to lung diseases, the dioxin disaster to soft tissue sarcoma, Chernobyl to cancer, heat and cold waves to death from heatstroke and freezing, but also to a worsening of symptoms and deaths in people with preexisting conditions, e. g. CHD. However, the various publications did not address the effects that are not typical of pollutants. Theory determines what can and cannot be observed (Einstein). Without considering the possibility of these ‘causally non-specific effects’, essential findings remain hidden.
A person's current organizational capacity can also be measured and used for health purposes. For example, it has been known for decades that the ability to distinguish flickering light as a sequence of individual light pulses rather than continuous light (‘flicker fusion frequency’) decreases from morning to evening, but also in the wake of, for example, attention-demanding activities. This becomes clear when one considers that biological effects are ultimately produced by individual cells (Virchow: cellular pathology!), which need their resources not only for ‘external services’ but primarily for cell-specific needs. The decrease in performance would be suitable, for example, for detecting the fatigue level of assembly line workers at an early stage before the rate of production errors increases — provided that the workers tested in this way do not deliberately give false information in order to avoid losing paid working time. [15] The flicker fusion frequency is the basis of the HEPATOM analyzer used at the University of Dьsseldorf to diagnose hepatic encephalopathy [7].
From a scientific point of view, it is significant that Kofler's assumption of a single ability that enables two ‘Janus-like coupled’ effects for energetic and meaningful effects can be traced back thousands of years. It was introduced by Aristotle as dynamis or, according to Potentia [1]. It enabled, for example, all objects within specified limits to have a self-determined orientation. This world view determined the natural sciences until Newton [14]. He felt compelled to abandon the prevailing notion that objects can only be moved by observable influences from other observable objects, since the famous apple falls without any visible connection to the ground. As a religious philosopher, he introduced God as the physically effective prime mover who, together with all creatures, created the all-compelling laws in seven days. According to this, there was only passive motion. Einstein refuted passive motion with his special theory of relativity: even each individual ray of light moves actively along the geodesics of the sun's field according to the spatial structure of the field, not because of a force with which the sun moves it. The elder Heisenberg took up the scientifically correct idea proposed by Bohr in 1924 but rejected again, namely to also grant quantum objects ‘dynamis or potentia’ and thus freedom of choice within narrow limits1 [6]. For Heisenberg, this eliminated the otherwise inherent absurdity of the quantum world [5]. His argument was taken up by only a few. This reference to the history of science is intended to show how diverse the theoretically accepted constructs can be. This also applies to the different approaches in medicine.
The Experimentum Crucis. The only technique that can be used to clearly prove which of several alternative solutions to a problem is scientifically more effective is the «Experimentum Crucis» (F. Bacon). This refers to an experiment in which two mutually exclusive hypotheses are tested at the same time. A classic example is Eddington's «Experimentum crucis», in which he used the deflection of light rays passing through the sun on their way to Earth to test whether the measured results better corresponded to what could be predicted using Newton's formula or Einstein's Theory of Relativity. Since then, it has been undisputed that the Theory of Relativity is more powerful. However, Einstein insisted that this should not be understood as a falsification of Newton's formulas and that the formulas should not be discarded, as Popper had demanded. Einstein pointed to their negligible inaccuracy in mechanics and therefore recommended their continued use in «classical questions» [4].
A. M. Stewart & G. W. Kneale (2000) presented a study whose approach allowed the results to be used as an experimentum crucis to distinguish whether the understanding of natural science, extended by a limited ability to organize, is more powerful in medical matters than the standard model they used, which does not recognize this limitation. In a lifelong follow-up study, Stewart & Kneale compared the mortality risk of survivors of the atomic bombs in Hiroshima and Nagasaki who, as a result of the atomic bombings, also suffered two or more physical injuries not caused by radioactivity (burns, purpura, injuries to the mouth and throat, epilation) and survived for five years with survivors who had no physical injuries but were exposed to the same level of radiation. They based their findings on the following assumptions: a) Five-year survivors with physical injuries are representative people; b) «Cancer is the only [late effect of radiation examined in the study]»; c) «The use of data from atomic bombs for risk assessment is generally based on the assumption that the survivors are representative people, apart from their radiation dose» [16].
Under these assumptions, there should be no difference in the mortality risk of the two groups.
However, significant and relevant differences were found between survivors with and without multiple injuries caused by the atomic bomb (Fig.). What explanations remain? Theoretically, the difference could be attributed to genetic factors. But in any case, what justification is there for continuing to use data from the atomic bomb survivors of Hiroshima and Nagasaki to draw countless conclusions, e. g. about the latency period of tumors?
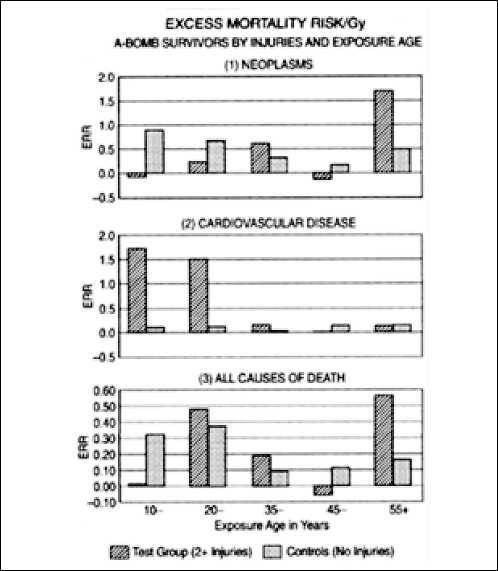
Fig. Excess relative risk (ERR) for three causes of death and live exposure ages (Stewart A. M., Kneale G. W., 2000).
But if we apply the model that assumes that both radiation exposure and physical damage require healing and thus the use of limited ability to organize, then the two groups differ: The survivors with and without physical damage as a result of the atomic bombings both belong to the «normal» population. Nevertheless, different effects must be expected, since although they were exposed to identical radiation doses, one group additionally had a need for organization to heal the somatic damage and the other did not. There is therefore no reason to reject the conclusions drawn from the follow-up studies in Hiroshima and Nagasaki.
The view extended to include the limited ability to organize has proven to be more effective in this experimentum crucis.
This epidemiologically proven statement is extremely important for practical medicine. Beyond general statement, the fundamental question of the consequences for individual patients must be answered. Doctors are accustomed to using the experience gained from large numbers of cases in the interests of their patients, based on their experience and empathy. However, every patient is an individual and therefore every illness is a unique event. Statistical statements about individual cases are not methodologically permissible, but they are indispensable in medicine. For this reason, medicine is considered an art. However, the extended approach advocated here is based on a fundamentally different premise. It is not a question of the plausibility of applying an average value, but rather of the assumption that each individual survivor in Hiroshima and Nagasaki had this empowerment, which was only available to a limited extent, at their disposal. This is comparable to the statement that every ray of light actively moves. This central conclusion of the work by W. Kofler et al. [10] was classified as the most significant of the papers submitted worldwide between 2000 and 2002 under the chairmanship of Nobel Prize winner Y. Tse Lee and was awarded the Th. Kuhn Hope for the Future for A Sustainable World Award 2002. The consequences of the Experimentum Crucis should also be far-reaching in practice: a new field has been opened up in which concrete predictions can be made for each individual case — without having to resort to empathy and art.
The approach has only been taken up in isolated cases. This may be due to a scientific counterargument from quantum physics: the effectiveness of radioactive radiation is based on quantum effects. In quantum theory, it is permissible to make predictions about the effect to be expected in large numbers. However, due to the uncertainty principle, extreme caution should be exercised before attributing epidemiologically proven statements to individual characteristics.
For this reason, a second experimentum crucis had to be carried out. The aim was to investigate whether a single person can achieve a change in biological effectiveness in their own body through targeted behavior. To do this, they had to deliberately influence the availability of their own limited ability to organize themselves in such a way that a predictable effect was achieved which would not have been expected without the deliberate influence, or at least not to the same extent.
The Challenges for the Methodology and Study Design
This requirement is almost impossible to meet methodologically: a general statement can only be expected if the person under investigation deliberately influences the result only with regard to the use of the ability to organize that is being tested, but does not influence the evaluation of the results of the effectiveness of the ability to organize achieved by him and on him. But self-confirming predictions are of no use to anyone. This sounds like trying to square the circle.
The prerequisites for the experimentum crucis were therefore as follows: The person concerned must be the researcher. He must voluntarily plan and carry out the self-experiment. These conditions were met because the researcher had been informed that he had lung cancer and would have to undergo surgery in a few weeks. He therefore had time to plan the experimental setup. He had to do this without knowing how the experiment/surgery would actually proceed.
At the time of diagnosis, histological confirmation of the suspected diagnosis (atypical carcinoid) was not yet available. The patient did not know which of the three methods would be used to remove the tumor: microsurgery or conventional surgery involving opening the chest with a more or less long incision. Or the third method, because the operation is started micro-surgically but then has to be continued macro-surgically, e.g. due to adhesions of the tumor to important blood vessels. The three techniques represent interventions of varying severity in homeostasis and the subsequent wound healing process. The study design must take all three options into account. According to the current state of knowledge, the patient has no influence on wound healing other than following the doctor's instructions. Based on the extended approach, the patient can influence the healing process by limiting competing reasons for the use of organizational ability after the operation so that this is available for the re-establishment of homeostasis and wound healing.
Setting benchmarks. As part of the researcher's lung cancer surgery, both scientific perspectives needed to be examined simultaneously. This required forecasts of the alternative courses of the disease and the establishment of a benchmark which, when exceeded or not reached, would show whether the standard theory without limited ability to organize or the extended view with limited ability to organize had enabled more accurate power for prediction. This benchmark had to be established before the operation.
It was also unclear whether any uses of the ability to organize could be influenced at all and how successful this influence could be. Therefore, as a precautionary measure, a second benchmark had to be set in case the result was unclear.
A benchmark was chosen over which the patient has no influence (length of hospital stay) and another over which he has only a minor but externally verifiable influence (length of home care compared to the doctor's recommendation). There is subjective influence here. However, the researcher is a doctor and knows from his own experience that healing processes should not be prematurely interfered with, especially in old age, as this can easily lead to permanent damage. He will therefore be careful not to place too much emphasis on this factor. Should this nevertheless be the case, it would have to become apparent during follow-up checks carried out by external experts.
The benchmarks were determined based on the results of routine operations and not on targeted research projects. It was therefore necessary to avoid any bias that could be caused by a pre-informed surgical team. The team, including the nursing staff at the hospital, was therefore not informed that the data would be used in a scientific publication. They only learned of this later, when the data collected at the clinic had to be made available for the study.
There are extensive publications worldwide on each of the three surgical techniques. Therefore, the current state of knowledge regarding the average length of hospital stay can be determined. In addition, the data available also allows for a more precise specification of the positive and negative factors influencing the length of hospital stay, which can be used to estimate the individual expected value. Finally, the surgeon involved had also provided information on the average length of stay for such operations in a globally cited publication. The average length of stay he reported was 11 days. This is largely consistent with the information in the international literature. Taking into account the influencing factors examined, only good general health and the fact that the patient was a non-smoker were found to be reasons that would lead to a below-average length of hospital stay. However, all other parameters indicated that an above-average length of hospital stay was to be expected: It was necessary to switch from microsurgical technique to open surgery, the patient is male, in his 80s, the tumor was very large at 74 x 78 mm, and two lung lobes had to be removed. The chest had to be opened to an above-average extent (approx. 13 cm incision length), requiring the ribs to be spread apart significantly. Accordingly, a longer than average hospital stay was to be expected. To be on the safe side and not to prematurely consider the prognosis as confirmed, the average of 11 days was nevertheless used as a benchmark. Only if the hospital stay was shorter than this was the prognosis considered to be confirmed.
In this case, the required proof would have been provided. However, prior to the operation, it could not be ruled out that the hospital stay would last exactly 11 days. In that case, the standard case would not have been more efficient. For this case, it should be possible to make a decision based on the second benchmark.
The second benchmark was the duration of home care expected by the doctor. Care was assumed to be necessary if the patient did not want to perform the activities at home that he had performed before the operation or could not perform them without assistance. This concerned, on the one hand, climbing stairs: the bedroom is on the first floor and the study is in the basement. The patient usually takes the (light) bag of plastic waste to the collection point. This is about 170 meters from the house and about 10 meters higher. The discharge letter stated 14 days of home care, measured from the day of actual discharge, not from the expected average length of hospital stay.
The maximum duration of the experimentum crucis was therefore set at 11 days for the average length of stay in hospital and 14 days of home care, i. e. 25 days in total.
Connection to the application-oriented followup study. In the event that the ‘extended approach’ proved to be more effective, the experimental approach offered the opportunity to address the medically challenging findings of Stewart and Kneale, which had been rejected for methodological reasons only. How should we reimagine the dynamics of achieving homeostasis in a way that makes it clear that seemingly trivial physical damage caused at the same time as radiation exposure would have lifelong consequences? In this case, it should be noted that prior to the operation, the tumor required a certain ability to organize, which was completely eliminated by the operation. At the same time as the tumor was removed, two lobes of the lung were also removed using a classic surgical technique that requires extensive healing processes. A separate study was planned for this purpose, in which objective and subjective data were collected over the course of a year. This will be reported on separately.
The Derivation of Techniques for Temporarily Saving Organisational Ability
On the potential for saving ability to organize. It is assumed that being able to organize and be energetically effective are only two aspects of one and the same empowerment, which, although they have different effects like the two sides of a coin, are quantitatively equivalent to each other. Based on this assumption, the corresponding equivalent of organizational ability can be inferred from the available or consumed amount of energy. Although the brain accounts for only about 2% of a person's biomass, it consumes about 20% of a person's oxygen and 40% of their glucose. Despite different activities performed within homeostasis, the resource consumption of an adult is practically unchanged at around 2500 kilocalories per day, of which 500 are accounted for by the brain. Potential savings can therefore be expected in the area of brain activity in particular.
The temporary restriction of intellectual activity therefore represents a potential saving that the patient can make targeted use of. The ability to organize is also tied up in social and emotional contacts, television, e-mail correspondence, reading books, computer games, professional activities, etc. From the point of view of saving organizational ability, it is therefore precisely those activities that patients like to see as indicators of their ability to successfully overcome the operation they have just undergone that should be consciously restricted.
The significance of these intellectual, cognitive and emotional demands on the available ability to organize, which is needed immediately after surgery for the reorientation towards a new homeostasis, can now be measured with great accuracy via energy consumption. For example, extremely strenuous eight-hour mental activity increases brain metabolism by 20 to 40 percent [8]. Such measurements have also shown that, due to the complex functioning of the retina, which has even been called the ‘brain within the brain,’ the reception, processing and transmission of visual stimuli and their interconnection with approximately 40% of all areas of the brain are of central importance for organizational processes [17]. These processes in particular can be temporarily restricted without any particular effort of will by wearing an eye patch all day during the hospital stay.
Preventive measures against impending postoperative additional requirements. Surgery often represents a physical and psychological stress. It should therefore be expected that the body's defense against infection will be compromised. This was taken into account in the study design, which was based on our own experience in managing the epidemic resulting from SARS CoV2 infection [12] .
Further individual needs were provided for according to the patient's specific situation. Appropriate offers from the clinic were incorporated in a targeted manner.
The Study Design for the Scientific Reasoning freedom of choice. Eddington's experimental setup does not allow any statement to be made on this point. Einstein's positions correspond to the world view of the religious philosopher Baruch Spinoza, whom Einstein professed to follow, just as he professed that he himself, like light rays, had no free will2. This characteristic of natural objects makes it understandable why Einstein was not compelled to grant quantum objects an empowerment that would enable them to observe and evaluate in order to actively change their spatial effectiveness. He only assumes observability and evaluation, not the transformation into something observable. However, in his understanding of science, only observation entitles us to make a reliable statement about nature [4]. Only spatial effectiveness is observable. If this is traced back to a non-scientific cause (God), there is no need to introduce an empowerment for non-energetic effectiveness, since God always has sufficient quality and quantity at his disposal. But is this really the simplest solution, to only watch the Austrian evening news in the hospital, but also the subsequent German news program at home? So, does Einstein's world view prove itself in this respect? So far, this has not been empirically tested. Aristotle's dynamis refers — albeit at different levels of quality — to all natural objects. Einstein's position in this regard is therefore not without relevance for the application of the ability to organize to the different levels between the intellectual level of the person and that of the individual cell. It therefore makes sense to raise the question of whether patients are free to adhere to the study design or not, and to what extent this is in line with Einstein's demand for the simplest practicable solution.
-
3) The patient should take his computer and mobile phone with him to the hospital, but not use them. The freedom to decide whether or not to comply with the study design was retained. He remained reachable from outside via the hospital's telephone system.
-
4) The patient was strictly prohibited from even thinking about his scientific questions while in the hospital. Instead, he was advised to focus on his wonderful holiday experiences and try to recall the beautiful images of snorkeling in tropical waters. Compliance with this voluntarily undertaken task was probably the greatest challenge for the test subject, as boredom during a hospital stay should not be underestimated. The patient used his stay for diagnostic clarification to write an article that can be read in Science [13].
-
5) Interpersonal contact with friends and family members should be restricted in the hospital as
2 Einstein answered Rabbi Goldstein's question: Do you believe in God: «I believe in Spinoza's God, who reveals himself in the lawful harmony of existence, not in a God who is concerned with the fates and actions of men». The New York Times 25 April 1929, «I am a determinist. I therefore do not believe in free will». In Isaacson W: Einstein: His Life and Universe, p 387)
much as possible, while maintaining politeness. However, it should not be completely prevented. This is to take into account the experience gained from the use of ‘artificial deep sleep’. This extensive sedation can be understood as an unconscious ‘heuristic’ application of the suppression of the ability to organize for intellectual, cognitive and emotional activities for therapeutic purposes. This technique of artificial sedation, which is often life-saving after serious accidents, is extremely successful in terms of wound healing, but it is not without risk: after several days of use, memory loss and anxiety can occur as a result of the non-use of brain functions. Speaking, writing, walking, eating independently, etc. sometimes had to be relearned. Even the slightest possibility of such influences should be avoided. For this reason, complete isolation was not sought in the hospital.
-
6) Prevention of immediate and indirect causes of an increased need for organizational ability in the immediate postoperative phase
-
a. Consistent use of pain management.
-
b. Supporting the daily rhythm by promoting sleep.
-
c. Removing possible irritation of the lips caused by protruding beard hair, which could lead to the recurrence of cold sores.
-
d. Regular use of N-chlorine taurine nasal spray to prevent various potential respiratory infections [12]. e. Permanent wearing of the ‘Norwegian socks’ purchased as a precaution during the planning phase prior to surgery: During the hospital stay for diagnostic clarification, it was found that patients easily slide forward in the hospital bed and then constantly have their bare feet in contact with the cold wall at the foot of the bed. This requires constant temperature regulation and thus the use of organizational skills. This was to be avoided by instructing patients to wear the ‘Norwegian socks’ at all times.
This approach was intended to ensure that the ability to organize was reduced to such an extent that it was made available to the wound healing process, so that this would lead to the benchmarks set before the operation being undercut. Requirement 1) was limited to the duration of the hospital stay. All others were limited to the duration of the experimentum crucis, i.e. a maximum of 25 days.
This study design was an essential part of the design for the overall study. It lasted a whole year. Its aim was to describe the healing process and to relate the findings and personal experiences to the Extended View model. This will be reported separately.
The Results
-
a) The operation was performed on Tuesday. The patient's state of health for discharge was assessed on Friday, three days later, and was included in the
discharge letter, which was also written on Friday. The letter stated that the patient would be discharged to home care on Monday. The patient therefore left the hospital six days after the operation. This means that the benchmark was clearly and significantly undershot. The prognosis based on the limited available ability to organize proved to be more accurate than without assuming the ability to organize.
Discussion
Regarding c): Sceptics may still argue that those who believe they have determined the study design were compelled by a factor beyond the control of science to determine the design in this way without being aware of its determinism. The same could be assumed of the patient, so that he too, without realizing it, would have been determined by this non-scientific factor to act differently in hospital than at home. Since neither the designer nor the patient has a method of investigating a non-scientific factor, this objection cannot be ruled out. However, Einstein's criterion that this would have been the simplest option can be ruled out. Furthermore, there is no method that could prove what the difference is in practice if the non-scientific factor obviously always forces the actor to do what he imagines he has decided or has actually decided himself. There can therefore be no medically relevant advantage in adopting Einstein's world view in this respect.
Regarding a) When assessing the length of hospital stay as a criterion for assessing the speed of recovery, it should be noted that the assessment of health was made on a Friday and the patient was discharged on the following Monday morning. It should also be noted that the assessing doctor did not know that his findings would be used for a scientific study. It can therefore be assumed that his approach was in line with that of any comparable routine operation. The patient is a private patient. It is not unusual for private patients to be discharged on Monday rather than on Friday, Saturday or Sunday. In any case, even at 6 days after the operation, the benchmark of 11 days of hospitalization is clearly not exceeded.
Regarding b): To evaluate whether the criterion is only formally fulfilled because the patient behaved in accordance with his subjective experience, or because the increase in his own contribution is the result of the natural healing process, the results of the external checks can be used. The discontinuation of external care for activities that were usual before the operation was confirmed on the 9th day after the operation. The wound healing was checked when the staples were removed on day 15. A very good healing process was observed. This finding therefore also confirms the higher performance of the state of knowledge extended by the limited ability to organize.
The planned maximum duration of the experimentum crucis of 25 days did not need to be exhausted. After 9 days, the study design for the physiological and application-related long-term study could be started.
It was thus proven that the performance of the current world view can be expanded, thereby opening up questions that were previously unanswerable. In this respect, the world view becomes more powerful than before. However, this does not mean that it is appropriate to work with the expanded approach in every case. In this respect, too, lessons can be learned from the practical implementation of Eddington's experimentum crucis. Einstein refused to comply with Popper's demand to understand this as a falsification of Newton's theory and to no longer apply Newton's formulas. Einstein pointed out that in classical questions, the benefits of the Theory of Relativity are minor, while the additional effort is unreasonably high. For pragmatic reasons, Newton's formulas should therefore continue to be used as simplifying special cases in classical questions.
The same applies to proving that individual health conditions are decisive in determining whether additional exposure leads to significant health disadvantages through
