Results of supracondylar osteotomy and bone fixation with the Ilizarov apparatus for cubitus varus and valgus deformities

Author: Kaul R., Prasad M., Akhoon N.
Journal: Гений ортопедии @geniy-ortopedii
Section: Оригинальные статьи
Article in issue: 3 т.31, 2025.
Free access
Introduction Cubitus varus denotes the inward deviation of the supinated forearm on the extended elbow. In cubitus valgus, the forearm is angled away from the body with the arm fully extended. Both deformities manifest clinically as an abnormal carrying angle, along with a cosmetically unsightly appearance, with or without restricted range of motion (ROM). The aim of the study is to evaluate the results of one-stage supracondylar corrective osteotomy and bone fixation using the Ilizarov apparatus in varus and valgus deformities of the elbow joint, using the angulation‑translation principle (osteotomy rule 2); to determine the effect of this method on the humerus-elbow-wrist angle (HEW), ODD and lateral prominence index (LPI). Materials and Methods A total of 12 patients, age ranging from 7–24 years, who presented with cubitus varus of ≥ 10° (n = 9) and cubitus valgus (n = 3) of ≥ 20°, were included in the study. All patients underwent acute correction using a mini-incision, supracondylar osteotomy and fixation with the Ilizarov frame. Results The mean time to union was 14.2 weeks (range, 11–18 weeks). The average duration of follow-up was 24 months. Functional outcome was graded as excellent in 9 cases (75 %), good in 2 (17 %) cases and poor in 1 case (8 %) using the grading system of Oppenheim. For cubitus varus, the mean HEW angle improved significantly, from (–15.5 ± 4.2) pre-operatively to (8.2 ± 1.5) post-operatively. For cubitus valgus, the mean HEW angle was (28.3 ± 5.3) pre-operatively, which improved to (14.1 ± 3.1) post-operatively, which was statistically significant. Complications encountered included superficial pin-tract infection in 1 case, lateral condylar prominence in 1 case and complete radial nerve palsy in 1 case. Discussion Conventional methods of treatment of cubitus varus or valgus include various corrective osteotomies, typically stabilized with internal fixation. Despite being successful, a substantial number of distressing complications have been reported with the use of internal fixation. The mandatory requirement of post-operative immobilization, resulting in stiffness and disuse atrophy, is a deterrent to the use of internal hardware, which can be easily circumvented by the versatility of the Ilizarov apparatus. Conclusion External fixation with the Ilizarov apparatus is a versatile means of correction of cubitus varus and valgus. It precisely achieves the desired carrying angle and cosmetic appearance of the elbow. It facilitates residual adjustments in under/over-corrected scenarios. The stability is indisputable. Early joint mobilization leads to an improved functional outcome.
Cubitus varus, cubitus valgus, osteotomy rules, Ilizarov fixator, deformity correction
Short address: https://sciup.org/142244803
IDR: 142244803 | DOI: 10.18019/1028-4427-2025-31-3-269-278
Результаты надмыщелковой остеотомии и фиксации костей ап- паратом Илизарова при варусной и вальгусной деформациях локтевого сустава
Введение. Варусная деформация локтевого сустава — это девиация внутрь супинированного пред- плечья при разогнутом локтевом суставе. При вальгусной деформации предплечье отклонено от тела при полностью разогнутой руке. Обе деформации проявляются клинически в виде аномального угла отведения, а также косметически неприглядного внешнего вида, с ограничением или без ограничения диапазона движения (ОДД). Цель работы — оценить результаты одномоментной надмыщелковой корригирующей остеотомии и фиксации кости аппаратом Илизарова при варусной и вальгусной деформациях локтевого суста- ва по принципу ангуляции-трансляции (правило остеотомии 2); определить влияние этого метода на плече-локте-запястный угол (HEW), ОДД и индекс латерального выступа (LPI). Материалы и методы. В исследование были включены 12 пациентов в возрасте от 7 до 24 лет с вару- сом ≥ 10° (n = 9) и вальгусом ≥ 20° (n = 3). Всем пациентам была проведена одномоментная коррекция с использованием мини-разреза, надмыщелковой остеотомии и фиксации аппаратом Илизарова. Результаты. Среднее время сращения составило 14,2 недели (диапазон 11–18 недель). Средняя продол- жительность наблюдения составила 24 месяца. Функциональный результат был оценен как отличный в девяти случаях (75 %), хороший — в двух случаях (17 %) и плохой — в одном случае (8 %) с использо- ванием системы оценок Оппенгейма. Для варусной деформации средний угол HEW значительно улуч- шился с (–15,5 ± 4,2) до операции до (8,2 ± 1,5) после операции. Для вальгусной деформации средний угол HEW составлял (28,3 ± 5,3) до операции и улучшился до (14,1 ± 3,1) после операции, что было ста- тистически значимым. Осложнения включали поверхностную спицевую инфекцию в одном случае, ла- теральный мыщелковый выступ — в одном случае и полный паралич лучевого нерва — в одном случае. Обсуждение. Традиционные методы лечения варусной и вальгусной деформации локтевого сустава включают различные коррегирующие остеотомии, обычно стабилизируемые внутренней фиксацией. Несмотря на их успешность, при использовании внутренней фиксации было зарегистрировано значи- тельное количество осложнений. Обязательное требование послеоперационной иммобилизации, при- водящее к ригидности сустава и атрофии мышц, является сдерживающим фактором для использования внутренних фиксаторов, что можно легко избежать с помощью универсальности аппарата Илизарова. Заключение. Внешняя фиксация аппаратом Илизарова является универсальным средством коррек- ции варусной и вальгусной деформаций локтевого сустава, благодаря ей достигают желаемых угла переноса и косметического вида локтя, облегчают остаточную коррекцию в случаях недостаточной/ избыточной коррекции. Стабильность не вызывает сомнений. Ранняя мобилизация суставов приводит к улучшению функциональных результатов.
Text of the scientific article Results of supracondylar osteotomy and bone fixation with the Ilizarov apparatus for cubitus varus and valgus deformities
Supracondylar fractures are the most common fractures encountered in paediatric population, accounting for 50–70 % of elbow injuries [1]. Treatment can vary from conservative management to open reduction with or without pinning, depending upon the fracture geometry [2, 3]. Cubitus varus is the most common angular deformity, presenting as late sequel to poorly-treated or untreated supracondylar fractures in children [4]. The main reason for development of this deformity is a varus tilt along with internal rotation and medial displacement of the distal fragment, resulting in an abnormal carrying angle [5]. Cubitus valgus, on the other hand, is a rather uncommon deformity arising most often from a lateral condylar non-union or malunion, with or without ulnar nerve symptoms [6]. The indications for corrective surgery include an undesirable cosmetic deformity or a limitation of elbow motion or both. Numerous osteotomies have been described for the treatment of cubitus varus and valgus [7]. The goal of correction is to address not only the coronal component, but the rotational and sagittal plane deformity, if any. Prevention of joint stiffness, by virtue of a stable fixation, and early mobilization is highly desirable.
The choice of osteotomy as well as of fixation methods is a topic of contention till date. Most surgeons prefer a lateral closing wedge osteotomy for cubitus varus for its technical simplicity and reproducibility [8]. Cubitus valgus is frequently addressed with a dome osteotomy along with ulnar nerve transposition [9]. Problems associated with acute corrective osteotomies include under- or over-correction, failure of fixation, neuropraxia, unsightly scars, re-fractures at the osteotomy site, joint stiffness, and infection [10]. The introduction of the Ilizarov method of a low-energy osteotomy, combined with gradual distraction, offered the unique ability to perform post-operative titration of angular correction, as well as early joint mobilization [10].
The aim of the study is to evaluate the results of one-stage supracondylar corrective osteotomy and bone fixation using the Ilizarov apparatus in varus and valgus deformities of the elbow joint, using the angulationtranslation principle (osteotomy rule 2); to determine the effect of this method on the humerus-elbow-wrist angle (HEW), ODD and lateral prominence index (LPI).
MATERIALS AND METHODS
Twelve patients, in the age range from 7 to 24 years, who presented with either cubitus varus or valgus, and desired surgical correction, were included in this retrospective study. We retrieved hospital records, radiographs, and clinical photographs from 2020 to 2024, of individuals who underwent deformity correction using a percutaneous, low-energy osteotomy, and bone fixation with an Ilizarov frame application, and analysed various clinical and radiological parameters, using Microsoft Excel 2024 (v.16). Those with an incomplete database or follow-up were excluded from the study. The objectives of the study were to assess the bearing of this method on the Humerus-Elbow-Wrist (HEW) angle, the Lateral Prominence Index (LPI) and elbow range of motion (ROM). Preoperative clinical examination included recording of the carrying angle and ROM, using a goniometer. The internal rotation element was assessed using the Yamamoto method [11]. The three-point bony relationship and inter-condylar distance measurements were recorded in all cases, although their clinical relevance is a matter of debate [12]. The HEW angles were measured on anteroposterior radiographs of both upper extremities, in addition to the LPI [7, 13]. In normal individuals, the LPI is predominantly a negative value, due to naturally-existing slight medial condylar prominence. All pre-operative planning and software simulation was performed using the Bone Ninja iPad mobile application [14].
Surgical technique
The Ilizarov frame design consisted of two rings, one proximal at the level of the mid-arm, and one distal at the level of the elbow joint (Fig. 1, a, b). The orientation of the distal ring was parallel to the distal humeral articular surface, whereas that of the proximal ring was perpendicular to the diaphysis (Fig. 1, b).

Fig. 1. Pre-assembled frame design: a — front view showing juxta-articular hinge placement, and side view, showing the motor/distraction assembly; b — intra-operative images of frame orientation before and after the osteotomy
The rings were connected to each other using juxta-articular hinges mounted on connecting rods, and a medially placed distraction assembly, orthogonally, as shown in the figure 1, b.
Two counter-opposed olive wires and one 5-mm Shanz pin, inserted along the safe corridors, were used to affix the distal ring (Fig. 2 a). The medial wire was inserted with the elbow in semi-extended position, palpating the ulnar nerve, and ensuring the wire entry anterior to the nerve. The proximal ring was affixed with two 5-mm Shanz pins and a wire. A 1-cm skin incision was sufficient to perform a low-energy osteotomy using the multiple drill-hole method (Fig. 2, b) [15]. The osteotomy was distracted acutely and an angulation-translation was performed, using the juxta-articular hinges (Fig. 2, c). Once satisfactory correction was confirmed under fluoroscopy, the osteotomy was compressed and the nuts tightened (Fig. 2, d). For larger deformities of more than 15° of angular correction, anterior transposition of the ulnar nerve was contemplated, both in cubitus varus and valgus. Any residual deformity detected in post-op radiographs was corrected subsequently.
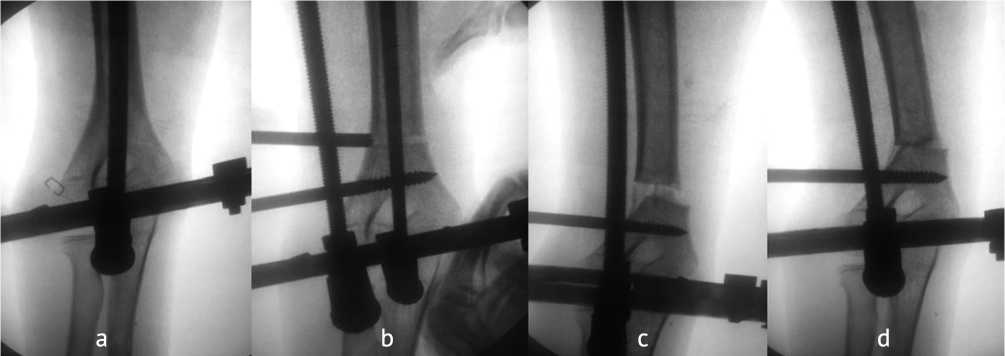
Fig. 2. The Ilizarov frame assembly: a — orientation of distal ring with counter-opposed olives; b — multiple drillhole osteotomy; c — acute distraction followed by angulation of the osteotomy; d — compression of the osteotomy after satisfactory alignment
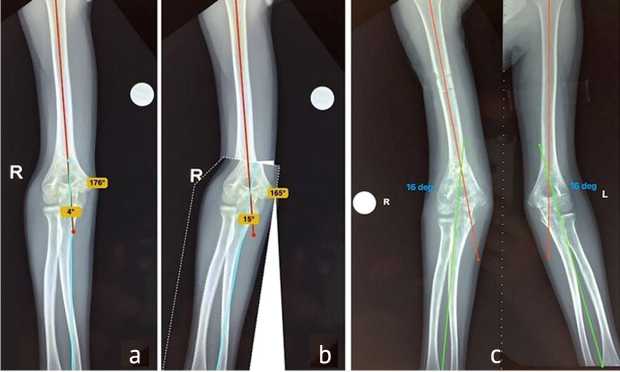
Fig. 3. Case of a 7-year-old male with cubitus varus: a — pre-op radiographs; b — simulation of correction using the bone Ninja application; c — final follow-up radiograph showing comparable HEW angles on both sides; d — clinical images before, during and after correction
Pre-op During correction
After correction

For skeletally mature patients with closed physes, a mini-Ilizarov assembly was used, which was less cumbersome as compared to the standard Ilizarov frame. Two 5-mm Shanz pins were placed percutaneously in the distal humerus from the lateral side, in the same plane, parallel to the joint line (Fig. 4, a), and two pins were placed in the mid-third of the humerus, perpendicular to the shaft, but in different planes, subtending an angle of around 45° when viewed from above (Fig. 5, b, d). The biplanar placement of pins was planned to circumvent the course of the radial nerve and increase the stability of fixation. The pins in the distal segment were mounted on a swivel-type Rancho cube (Fig. 5, d, circled in red), to allow angulation of the distal fragment following the osteotomy, which was performed precisely as described above. It is noteworthy to state here, that while performing all acute corrections, translation precedes angulation, in accordance with osteotomy rule 2 (Fig. 4, c, d) [16]. Fine adjustments and fastening of all connections was performed under C-arm guidance. Derotation was performed only in one patient who had impaired shoulder function compared to the contralateral side.

Fig. 4. Mini-Ilizarov frame: a — with 2 parallel Shanz pins in the distal fragment; b — multiple drill hole supracondylar osteotomy; c — medial translation performed first; d — followed by angulation to the desired degree; e, f — measurement of the angular correction intra-op, using a radiolucent, sterile goniometer
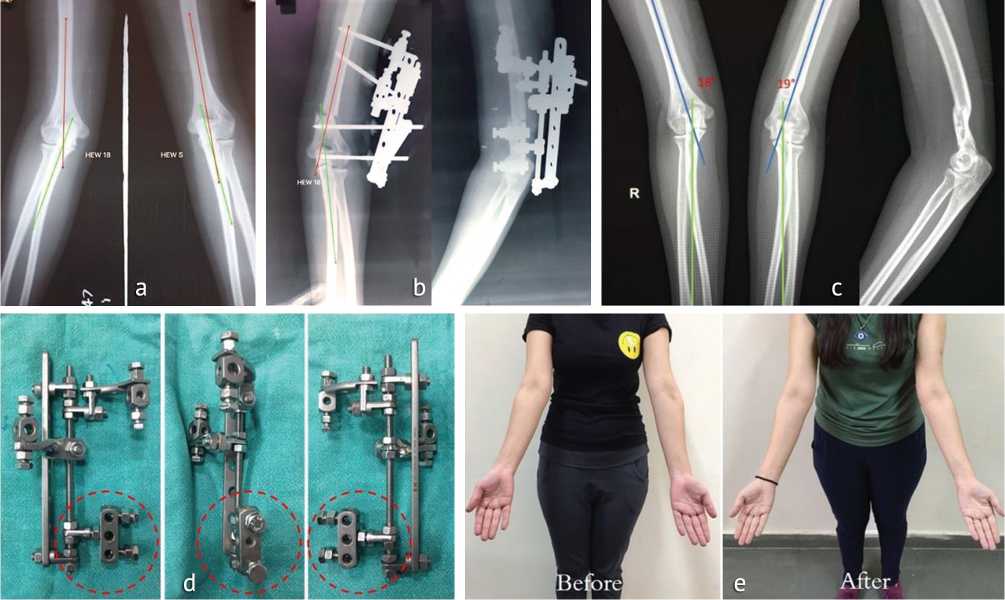
Fig. 5. Case of a 17-year-old girl: a — pre-operative radiographs of cubitus rectus; b — post-operative radiographs following mini-Ilizarov correction; c — final follow-up radiographs showing accurate correction, comparable to contralateral elbow; d — mini-Ilizarov frame assembly, red circled portion represents the swivel-type Rancho cube for the distal fragment; e — clinical images before and after correction
Post-operative protocol comprised of assisted joint ROM exercises at the end of week 1, followed by strengthening exercises at 4 weeks. Crutch-assisted walking using the operated upper limb was encouraged in older patients, to simulate weight-bearing in the lower extremity, in order to promote union. Frame removal was done after satisfactory consolidation was seen on orthogonal radiographs. Follow-up was done at 2-week intervals until frame removal, and every 6 month thereafter. The functional outcome was assessed and graded as excellent, good, or poor according Oppenheim’s criteria [17]. Statistical analysis was done using Microsoft Excel 2024 (v.16), applying Student’s paired t-test, with a p -value of < 0.05 considered as significant.
RESULTS
The mean patient’s age recorded was 16.2 years. Of the 12 patients, 4 (33.3 %) were males and 8 (66.7 %) were females. The mean time to union was 14.2 weeks (range 11–18 weeks). The average duration of follow-up was 24 months. Functional outcome was graded as excellent in 9 cases (75 %), good in 2 (17 %) and poor in 1 case (8 %) using the grading system of W.L. Oppenheim et al. [7, 17]. There was no significant difference between the mean pre- and post-operative arc of motion ( p -value: 0.16). The cumulative results are summarized in Table 1 and Table 2.
Table 1
Comparison of pre-op and post-op assessment parameters
|
Parameter |
Pre-op ° ± SD |
Post-op ° ± SD |
P -value |
|
Mean HEW* angle |
|||
|
Cubitus varus |
–15.5 ± 4.2 |
8.2 ± 1.5 |
< 0.05 |
|
Cubitus valgus |
28.3 ± 5.3 |
14.1 ± 3.1 |
< 0.05 |
|
Mean flexion / extension |
125 / –5 |
120 / 0.5 |
0.16 |
|
Mean LPI* (cubitus varus) |
2.5 ± 0.5 |
–1.6 ± 0.2) |
< 0.05 |
|
Mean MPI*(cubitus valgus) |
–8.4 ± 1.3 |
–3.7 ± 0.4 |
< 0.05 |
* HEW — Humerus Elbow Wrist angle; LPI — Lateral prominence index; MPI — Medial prominence Index.
Table 2
Functional results as per Oppenheim’s grading
|
Interpretation |
Criteria |
No. of cases |
|
Excellent |
1. Correction of varus or valgus to within 5°of contralateral elbow |
9 |
|
2. Loss of motion ≤ 5° of pre-op value |
||
|
3. No complications |
||
|
Good |
1. Correction of varus or valgus to within 6–10°of contralateral elbow OR |
2 |
|
2. Loss of motion ≤ 6–10° of pre-op value OR |
||
|
3. Scarring or a lazy-S deformity |
||
|
Poor |
1. Residual (uncorrected) varus or valgus differing by >10° of contralateral elbow OR |
1 |
|
2. Loss of > 10° in any plane of motion OR |
||
|
3. Any complication |
Cubitus varus ( n = 9): The mean HEW angle improved significantly from (–15.5 ± 4.2) pre-operatively to (8.2 ± 1.5) post-operatively. The average lateral prominence index pre-operatively was (2.5 ± 0.5), which improved to (–1.6 ± 0.2), negative indicating normal values. We included in our series one patient who had a straight elbow (cubitus rectus), who had esthetic concerns and who underwent correction with a mini-Ilizarov frame yielding gratifying results. Complications encountered included superficial pin-tract infection in one case managed with antibiotics and local dressings, and lateral prominence in one case which was managed conservatively.
Cubitus valgus (n = 3): The mean HEW angle was (28.3 ± 5.3) pre-operatively and improved to (14.1 ± 3.1) post-operatively, which was statistically significant. Mean medial prominence index (MPI) was calculated for valgus deformities [7], and found to be (–8.4 ± 1.3) pre-operatively and (–3.7 ± 0.4) post-operatively. One patient who underwent corrective osteotomy with the mini-Ilizarov frame (Fig. 6 and Fig. 7) had a post-operative wrist drop, which was initially managed expectantly, with no improvement for the first 14 weeks. Nerve conduction studies (NCS) suggested complete axonotemesis involving the radial nerve and radiographs showed a consolidated osteotomy with satisfactory limb alignment. The patient underwent radial nerve exploration along with frame removal (Fig. 7). Intra-operatively, one of the Shanz pins had inadvertently damaged a portion of the radial nerve, forming a neuroma in continuity (Fig. 7, c). Using a nerve stimulator, the non-conducting segment of the nerve was excised, and end-to-end epineural repair was performed using 9–0 polypropylene sutures (Fig. 7, d, e). The patient had a complete recovery of his elbow, wrist, and finger movements at the end of around 12 months after the repair (Fig. 8). One patient, with a large valgus deformity of 33° underwent a prophylactic anterior transposition of the ulnar nerve along with the osteotomy.
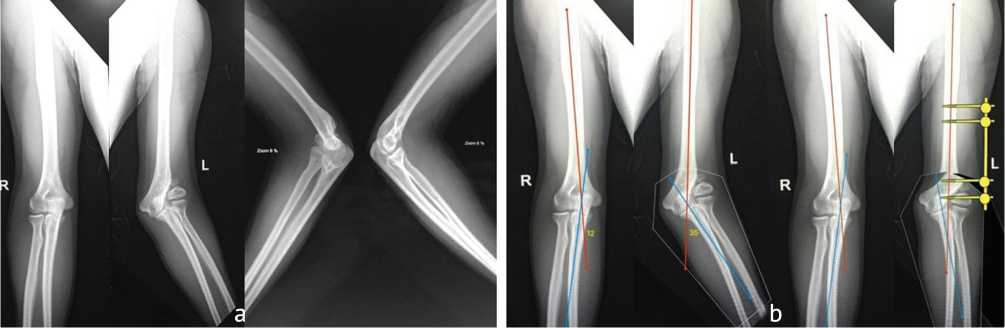
Fig. 6. Case of a 24-year-old male with cubitus valgus: a — pre-operative radiographs; b — simulation of correction using the Bone Ninja application
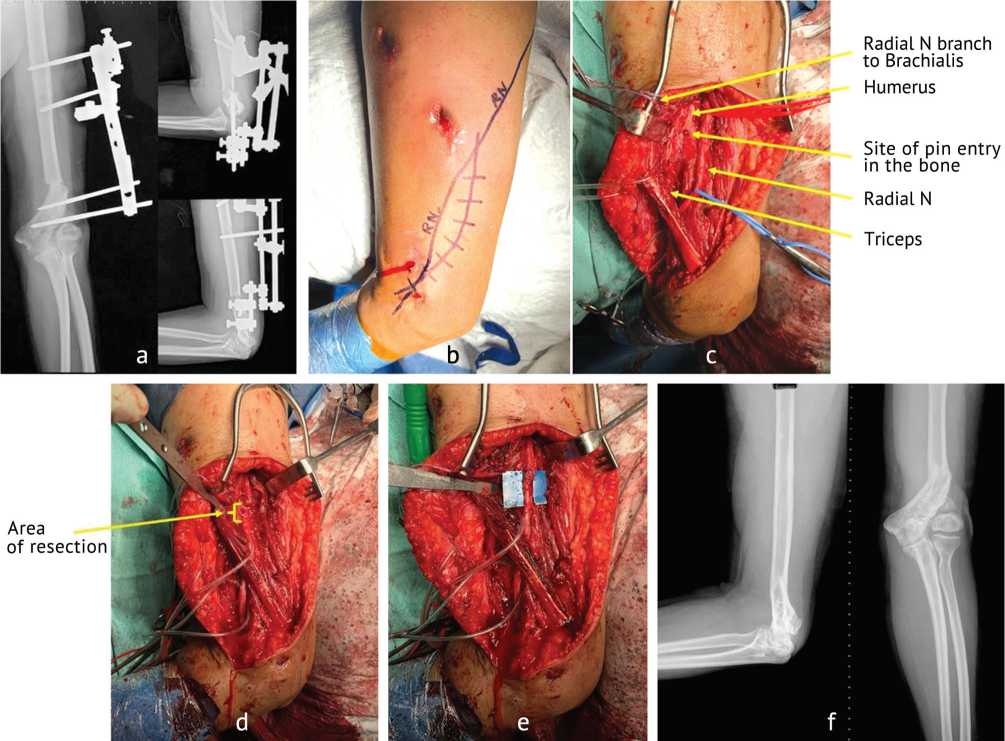
Fig. 7. Case of a 24-year-old male with cubitus valgus: a — post-operative radiographs following mini-Ilizarov correction; b — skin marking for radial nerve exploration; c — intra-operative findings during exploration, showing the pin entry into the bone, immediately adjacent to the neuroma; d — resected non-conducting segment, as determined by nerve stimulation; e — end-to-end epineural repair, reinforced with Tisseal® fibrin sealant; f — final follow-up radiographs showing satisfactory consolidation and limb alignment

Fig. 8. Clinical images of the same individual: a — before and after correction; b — functional status post-radial nerve repair
DISCUSSION
Traditional methods of treatment of cubitus varus include the lateral closing wedge osteotomy [18], the medial opening wedge osteotomy (D. King and C. Secor) [19], the modified French osteotomy [20], the oblique osteotomy [21], the dome osteotomy [22] and the step-cut osteotomy [23]. Subsequently, many authors described various modifications of the prevailing techniques, such as the penta-lateral osteotomy [24], the 3-dimensional osteotomy [25], the lateral equal-limbs osteotomy [13], the double-dome osteotomy [26], the oblique lateral closing wedge osteotomy [27], and the reverse step-cut osteotomy [28]. Cubitus valgus is most commonly treated with a step-cut translation osteotomy or a rotational dome osteotomy [7]. Despite being successful, a substantial number of complications such as elbow stiffness, nerve injuries, under-correction, recurrence, non-union, osteomyelitis and skin sloughing have been reported with the use of internal fixation following various osteotomies [10, 29]. Furthermore, the mandatory requirement of a relative period of immobilization post-operatively, resulting in stiffness and disuse atrophy, is a deterrent to the use of internal hardware.
External fixation, be it the Ilizarov apparatus, or a standard uniplanar fixator, has gradually gained acceptance and approbation as an effective means of treatment of these deformities. C.C. Hasler et al., in their series of 9 patients, reported excellent functional outcomes and cosmetic appearance with the closing wedge osteotomy coupled with a Hoffman (Stryker, USA) external fixator without any major complications [30]. T. Slongo et al.. described a technique of lateral closing wedge osteotomy, along with a mini-external fixator (DePuy Synthes, USA) application, with reasonable success [31]. However, their technique involved a long surgical incision over the lateral aspect of the elbow, with direct visualisation of the radial nerve. The Ilizarov apparatus, by virtue of its inherent stability, has a definite advantage over other fixators in the fixation of small and unstable fragments [10, 29, 32]. The counter-opposed olive wires provide sufficient stability to resist torsional and bending forces acting on the osteotomized fragment, minimizing the chances of recurrence of the deformity [29]. Another distinctive advantage over conventional methods is the ability to perform residual deformity correction in the post-op phase, with early mobilization and resumption of activities of daily living. Early mobilization leads to better functional rehabilitation and may have an impact on the outcome. Unsightly scars as in traditional approaches are avoided. The internal rotation component of the deformity can be addressed by derotation of the distal ring, if necessary.
Unlike the lateral closing wedge, where the resultant cortical mismatch creates a ‘lazy-S’ deformity, the Ilizarov method, which entails the use of a low-energy osteotomy with careful preservation of the periosteum and gradual distraction through the regenerate, can avert this ugly deformity [33, 34]. Previous studies on the Ilizarov method by V. Karatosun et al. [32], A. Piskin et al. [10], and C. Ozkan et al. [35] described an opening wedge osteotomy along with gradual correction with outstanding results and low rate of complications. A recent study by R. Agrawal et al. illustrates an angulation-translation osteotomy (rule 2) by using juxta-articular hinges placed at or very near the centre of rotation of angulation (CORA) [29]. The medial translation, achieved thus, minimizes the chances of lateral prominence. In our study, we have achieved the necessary angulation and translation for both cubitus varus and valgus, by performing acute correction abiding by the osteotomy principles [36], and by measuring the degree of correction achieved under C-arm guidance with a sterile radiolucent goniometer. This, in turn, led to a more accurate correction of the angular deformity, comparable to the contralateral, normal limb. A comparison of our study with similar ones utilizing external fixation is summarized in Table 3. Although we encountered just one major complication [37], it is prudent to mention that the risk of nerve injuries remains substantial, and is best circumvented by careful soft tissue dissection, following safe corridors, and using tissue-protection sleeves while drilling and inserting pins.
Table 3
Summary of similar studies on the use of corrective osteotomies coupled with external fixation for cubitus varus and valgus deformities
|
Title of study |
No. of cases |
Technique |
Mean follow-up (months) |
Functional outcome |
Complications and their number# |
|
V.A. Karatosun et al. [32] |
7 |
Supracondylar osteotomy + gradual correction |
66.7 |
Excellent outcome in all 7 cases ( Bellemore score ) |
Major: Nil Minor: 02 |
|
P.P. Koch, G.U. Exner . [38] |
4 |
Medial opening wedge osteotomy + acute correction |
24 |
Good outcome in all 4 patients. Mean valgus correction of 21.8° was achieved; One patient additional flexion modification was required |
Minor: 02 |
|
A. Piskin et al. [10] |
24 |
Medial/lateral open wedge osteotomy + gradual correction |
18.3 |
Excellent outcome in 18 cases; good in 6 ( Bellemore score ) |
Major: 03 Minor: 05 |
|
C. Ozkan et al. [35] |
5 |
Medial opening wedge osteotomy + gradual correction |
28 |
Excellent in all 5 cases ( Bellemore score ) |
Minor: 01 |
|
R. Agrawal et al. [29] |
32 |
Supracondylar osteotomy (angulation-translation) + gradual correction |
48 |
Excellent in 25 cases (78.12 %), good in 2 (6.25 %) and poor in 5 (15.63 %) ( Oppenheim score ) |
Major: 02 Minor: 04 |
|
Present study |
12 |
Supracondylar osteotomy (angulation-translation) + acute correction |
24 |
Excellent in 9 cases (75 %), good in 2 (17 %) and poor in 1 case (8 %) ( Oppenheim score ) |
Major: 01 Minor: 02 |
Note : # — Major complications include: fracture, lateral prominence, nerve palsy, deep infection; minor complications include: superficial pin-tract infections, loss of motion
CONCLUSION
External fixation with the Ilizarov apparatus is a versatile means of correction of cubitus varus and valgus. It precisely achieves the desired carrying angle and cosmetic appearance of the elbow. Additionally, it facilitates residual adjustments in under/over-corrected scenarios. The stability is indisputable, despite there being only a small area of bony contact. No implant is left after frame removal. Early joint mobilization undeniably leads to an improved functional outcome.
Conflicts of Interest . None to declare.
Funding . This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
