Stress radiography in the assessment of residual deformity of idiopathic clubfoot following serial casting (Ponseti method) in Thi Qar province
 in Thi Qar province")
Author: Abbas Z.A., AlBaghdadi F.A., Shaty W.G.
Journal: Гений ортопедии @geniy-ortopedii
Section: Оригинальные статьи
Article in issue: 6 т.31, 2025.
Free access
Background Clubfoot, or congenital talipes equinovarus, is a congenital foot malformation and condition. Its early detection and identification can ensure the best possible long-term outcomes for the infant. Stress radiographs provide objective evidence of residual deformity, guiding further treatment. Aim of the study was to compare radiographic findings of residual idiopathic clubfoot deformity in non-stress and stress positions to know the relationship of the angles difference and the type of treatment. Material and Methods This study is a cross-sectional comparative study conducted at Al-Nasiriyah Teaching Hospital. Data was collected for the period from the 1st of March 2024 to the 1st of March 2025. The study includes 73.3 % males in a mean age of 1.7 years. Unilateral deformities among them were 80 %, equinus 85.2 % and adduction 66.7 %. 112 children with clubfoot deformities and 45 with idiopathic clubfoot cases (54 feet) which had residual deformity were included. Results Stress radiographs revealed significant angular reductions in various deformities. Cutoffs of > 18° for the talo-first metatarsal angle in lateral view )adduction) and > 20° for the tibio-calcaneal angle (equinus), both with high sensitivity and specificity. Discussion Clubfoot is more prevalent in male patients and often presents as a unilateral deformity. The most common residual deformities observed are equinus and adduction. Conclusion Stress radiographs play a crucial role and show significant angular changes that help evaluate deformity flexibility and severity. Larger angle differences correlated with successful casting, while smaller differences predicted surgery.
Stress radiography, assessment, residual deformity, clubfoot, serial casting
Short address: https://sciup.org/142246507
IDR: 142246507 | UDC: 617.586-007.5-089.22-089.4:615.463:616-073.75 | DOI: 10.18019/1028-4427-2025-31-6-756-763
Стресс-рентгенография в оценке остаточной деформации идиопатической косолапости после серийного гипсования (метод Понсети) в провинции Thi-Qar
Введение. Косолапость, или врожденная эквиноварусная деформация стопы, является врожденным пороком развития стопы. Раннее выявление и идентификация могут обеспечить наилучшие долгосрочные результаты лечения для ребенка. Рентгенограммы с нагрузкой предоставляют объективные данные об остаточной деформации, определяя дальнейшее лечение. Цель работы — cравнение рентгенологических данных при остаточной идиопатической косолапости в положениях без нагрузки и с нагрузкой, а также определить взаимосвязь между разницей углов и видом лечения. Материал и методы. Данное исследование представляет собой сравнительное исследование, проведенное в клинической больнице Аль-Насирия. Данные были собраны за период с 1 марта 2024 года по 1 марта 2025 года. В исследовании приняли участие 73,3 % детей мужского пола, средний возраст которых составил 1,7 года. В исследование были включены 112 детей с деформацией косолапости и 45 детей с идиопатической косолапостью (54 стопы) с остаточной деформацией. Результаты. Нагрузочные рентгенограммы выявили значительное уменьшение углов при различных деформациях. Пороговые значения для угла между таранной и первыми плюсневыми костями в боковой проекции (аддукция) составили > 18°, а для угла между большеберцовой и пяточной костями (эквинус) — > 20°. Оба показателя характеризуются высокой чувствительностью и специфичностью. Дискуссия. Косолапость чаще встречается у пациентов мужского пола и часто проявляется односторонней деформацией. Наиболее распространенными остаточными деформациями являются эквинус и приведение. Заключение. Рентгенограммы под нагрузкой играют решающую роль, показывая значительные изменения углов, которые помогают оценить гибкость и тяжесть деформации. Более значительная разница углов коррелировала с успешным гипсованием, в то время как меньшая разница предсказывала необходимость хирургического вмешательства.
Text of the scientific article Stress radiography in the assessment of residual deformity of idiopathic clubfoot following serial casting (Ponseti method) in Thi Qar province
Clubfoot, or congenital talipes equinovarus, is a congenital foot malformation and condition. It is one of the most common musculoskeletal birth defects, presenting with four primary malformations that range in severity and degree of predicted contractures: Midfoot cavus, Forefoot adductus, Heel/hindfoot varus, and Hindfoot equinus [1].
Clubfoot, when identified early and treated effectively, has good success rates in correction and overall patient outcomes. Therefore, its early detection and identification can ensure the best possible long-term outcomes for the infant [2].
The incidence of clubfoot is reported to be between 0.5 and 2 cases per 1,000 newborns [3]. Males are twice as common as girls to be born with clubfoot [4].
Although the exact aetiology remains debated, the consensus favours multiple genetic and environmental risk factors that play varying levels of contributing roles in its clinical manifestations [5].
Approximately 7 % of clubfoot patients may present with an additional congenital defect at birth, and 7.6 % will exhibit a neurodevelopmental disorder of varying severity [6].
The foot in clubfoot is held in an abnormal position, with the toes pointing downward and inward (equinovarus). This leads to abnormal gait patterns and difficulty with normal weight-bearing. The rigidity of the deformity varies, with some cases being more flexible and others more resistant to correction [7].
Characteristic foot abnormalities include midfoot cavus, forefoot adductus, hindfoot varus and equinus, varying in severity and rigidity. The Pirani scoring system is the most commonly used method to assess severity due to its reliability [1].
The Pirani system entails evaluating six distinct factors in the foot. Each parameter is assigned a score of 0, 0.5, or 1 based on its severity. This rating establishes a minimum score of 0 per foot and a maximum value of 6. Three factors pertain to the hindfoot, whereas three relate to the midfoot [8].
Stress radiography plays an important role in evaluating residual deformities after the treatment of clubfoot using the Ponseti method. Although clinical examination is the primary tool for assessing the correction, stress radiographs provide detailed imaging that helps in visualizing subtle deformities that may not be evident during physical examination. These radiographs are taken under specific forces to highlight joint and bone alignment and stability in the foot [9, 10].
Stress radiographs provide objective evidence of residual deformity, guiding further treatment. If residual deformities are detected, additional interventions such as repeat casting, Achilles tenotomy, or even surgical procedures (e.g., tibialis anterior tendon transfer) may be necessary to prevent the recurrence of the deformity [11].
Aims To study the difference between degrees of angles of stress view and nonstress view of the residual deformity in idiopathic clubfoot and its relationship with type of treatment casting or surgical imtervention.
MATERIALS AND METHOD
This study is a cross-sectional comparative study conducted at Al-Nasiriyah Teaching Hospital to compare radiographic findings of clubfoot deformity in non-stress and stress positions and to assess the extent of residual deformities following Ponseti treatment of idiopathic club foot. Data was collected for the period from the 1st of March 2024 to the 1st of March 2025.
During the study period, 112 children with clubfoot deformities consulted the clubfoot clinic at Al-Nasiriyah teaching Hospital, and 45 with idiopathic clubfoot cases (54 feet ) which had residual deformity were included in the study. The remaining patients were excluded because they had other types of clubfoot deformity.
The study included 45 patients who were diagnosed with clubfoot; their mean age was 1.7 years and ranged between 3 months and 5 years. 73.3 % of them were male and 26.7 % of them were female. A positive family history of clubfoot was present in 24.4 % of patients. The consanguinity was present in 46.7 %. All these data are presented in Table 1.
Table 2 shows clinical features related to the clubfoot, regarding the site of the problem; it was unilateral in 80 % of patients and 20 % of them had bilateral involvement. Regarding the residual deformities, 85.2 % had equinus deformity, 66.7 % had adduction and only 14.8 % of them had cavus.
Table 1
Patients’ sociodemographic characteristics
|
Variables |
% |
No. |
|
|
Age |
3 months — 5 years |
||
|
Mean ± SD |
1.7 ± 0.9 |
||
|
Gender |
Male |
33 |
73.3 |
|
Female |
12 |
26.7 |
|
|
Residency |
City center |
29 |
64.4 |
|
Rural |
16 |
35.6 |
|
|
Family history |
Yes |
11 |
24.4 |
|
No |
34 |
75.6 |
|
|
Cosenguanity |
Yes |
21 |
46.7 |
|
No |
24 |
53.3 |
|
Clubfoot-related characteristics
Table 2
|
Variables |
No. of feet |
% |
||
|
Site of deformity |
Unilateral ( N = 36) |
Right |
26 |
72.2 |
|
Left |
10 |
27.8 |
||
|
Bilateral ( N = 9) |
18 |
33.3 |
||
|
Residual deformity |
Varus |
16 |
29.6 |
|
|
Adduction |
36 |
66.7 |
||
|
Equinus |
46 |
85.2 |
||
|
Cavus |
8 |
14.8 |
||
The Patients with incomplete treatment using the Ponseti method, patients unable to tolerate or cooperate during stress radiography, and other types of clubfoot such as postural, syndromic and neurological types were excluded from the study.
A prepared data collection sheet was used to gather the data for the following variables: demographic data (including age, gender, residency and socioeconomic status); family history (consanguinity of parents, age of father and mother and number of siblings); clinical presentation (including the site of the problem, unilateral or bilateral, and pre-and post-treatment severity) and were evaluated using the Pirani score as determined by an orthopaedic specialist. The patient was referred for radiographic imaging taken in two views: anteroposterior and lateral with and without stress. Each patient underwent radiographic imaging of the affected foot using X-RAY 500 MA (manufactured by GU/USA). Non-Stress Position: The foot is positioned in a neutral alignment with no external manipulation. Stress Position: Manual pressure is applied by the examiner to attempt correction of the deformity during radiography used to differentiate between rigid and flexible deformities. Two types of stress were applied. Abduction stress was used to check the forefoot and midfoot flexibility. Dorsiflexion stress was used to evaluate the hindfoot flexibility and ankle joint range of motion.
To obtain radiographs that ensure consistent pressure, one of the patient's relatives was informed how to apply the stress to capture corrected angles.
The following angles were measured.
Talocalcaneal Angle measures hindfoot alignment since decreased angles indicate residual varus. This angle was measured by obtaining an anteroposterior (AP) radiograph of the foot. Identify the central axis of the talus (line drawn along the talar body and neck) and the central axis of the calcaneus. Measure the angle formed by the intersection of these two lines. The normal value range between 25º and 40º. Below this value indicates residual varus deformity (Fig. 1).
Tibiocalcaneal Angle evaluates ankle position and Achilles tendon flexibility. This angle is measured by obtaining a lateral radiograph of the ankle. Identify the longitudinal axis of the tibia and the axis of the calcaneus. Measure the angle formed at the intersection of these two lines. Between 60º to 90º is the normal value and any increase in this value is considered as equinus deformity (Fig. 2).
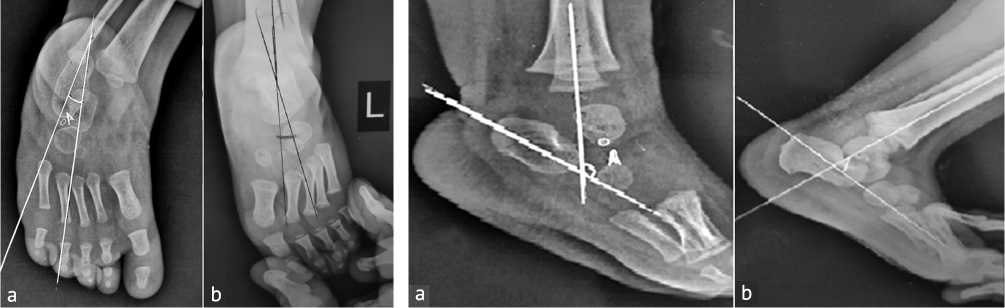
Fig. 1. Talo-calcaneal angle: (a) classic Fig. 2. Tibiocalcaneal angle: (a) classic view; (b) stress view view; (b) stress view
Talus-first metatarsal Angle (AP view) evaluates the alignment and structure of the midfoot and forefoot. It assesses medial-lateral alignment. The angle is formed between the long axis of the talus and the long axis of the first metatarsal. It is 0 to 20º in normal foot; any angle more than this range will consider forefoot adduction (Fig. 3).

Fig. 3. Talo-first metatarsal angle (AP view): (a) classic view; (b) stress view
Talo-first metatarsal angle (lateral view) assesses the longitudinal arch of the foot and the vertical alignment of the talus with the first metatarsal. It evaluates the degree of arch collapse or elevation. The normal value is 0 to 4º (Fig. 4).
Each measurement was performed by one radiology specialist and one orthopaedic specialist to ensure reliability and reduce observer bias. The College of Medicine, the University of ThiQar Ethical Committee, and the Thi-Qar Health Directorate's ethical committee all awarded their ethical approval. Participants' anonymity and confidentiality were preserved for the whole investigation. Additionally, informed consent was obtained from patients' parents or legal guardians.
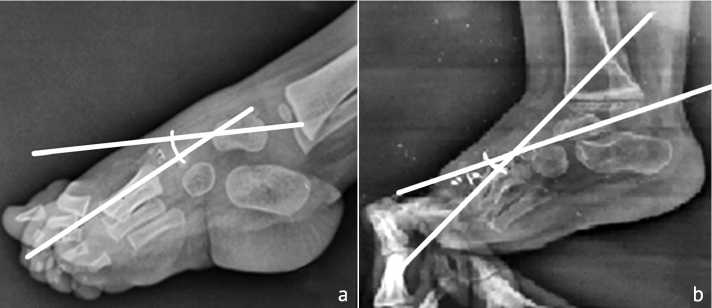
Fig. 4. Talo-first metatarsal angle (lateral view): (a) classic view; (b) stress view
A computerized statistical program called the Statistical Package for Social Sciences (SPSS) version 26 was used to enter and analyze the data. The proper statistical tests were conducted: two samples independent t-tests were used for the continuous variable, and a Chi-square test was used for categorical variables. The significance threshold (p-value) is set at ≤ 0.05 for all statistical analyses.
RESULTS
A significant decrease in the talocalcaneal angle was observed as the angle changed from 25.25º to 17.25º after the application of stress and the p-value = 0.001. Table 3 shows the difference in angles before and after the application of stress among different residual deformities.
Table 3
Difference in angles before and after the application of stress in different residual deformities
|
Variables |
With stress |
Without stress |
P -value |
|
|
(Mean ± SD) |
||||
|
Varus |
Talo-calcaneal angle |
25.25 ± 2.29 |
17.25 ± 1.43 |
0.001 |
|
Adduction |
Talo-first metatarsal angle (ap) |
40.11 ± 4.8 |
19.22 ± 8.03 |
0.001 |
|
Cavus |
Talo-first metatarsal angle (lateral) |
20.0 ± 2.3 |
8.0 ± 0.0 |
0.002 |
|
Equinus |
Tibio-calceneal angle |
115.42 ± 7.01 |
97.1 ± 7.45 |
0.001 |
Regarding the adduction deformity, the stress showed a significant reduction in the talo-first metatarsal angle (AP view) as the p = 0.001.
While the talo-first metatarsal angle (lateral view) also showed a significant reduction of angle with stress application from 20.0º to 8.0º and the p = 0.002.
Similarly, the talo-calcaneal angle and the tibio-calcaneal angle reduced with stress application ( p = 0.001).
The surgery was required in 26 patients (48.1 % of feet), and 28 patients (51.9 %) with residual deformity were treated with plaster casting.
Table 4 shows the association between the angle differences after the application of stress and the decision of casting or surgery. Regarding the varus deformity, the mean difference in the talo-calcaneal angle after stress was 7 among those who needed surgery and it was 9 among those who needed casting and the mean difference shows a statistically significant association with the fate of patients since p -value=0.002.
Talo-first metatarsal angle (AP view) for the adduction deformity, showed a significantly lower angle mean difference in the surgery group in comparison to the casting group (16.0 vs 24.0 among both groups respectively) and the p = 0.001.
Talo-first metatarsal angle (lateral view) for the cavus deformity, the mean difference in the angle after stress was 14.0 among the casting group and a lower mean 10.0 among the surgery group and the p = 0.005.
Finally, eqiunus deformity, tibio-calcaneal angle shows a mean difference of 23.7 in the casting group and a lower mean difference of 13.45 in the surgery group. The larger mean difference indicates the need for casting in all residual deformity of idiopathic clubfoot, for varus, adduction, equinus and the cavus.
As p = 0.05 there is a significant role for the angle difference after stress application in determining the proper treatment method.
Table 4
Association between mean difference in angles with and without stress and the fate of patients
|
Variables |
Surgery Mean difference |
Casting Mean difference |
P -value |
|
|
Varus |
Talo-calcaneal angle |
7.00 ±1.01 |
9.00 ± 1.06 |
0.002 |
|
Adduction |
Talo-first metatarsal angle (ap) |
16.0 ±5.65 |
24.0 ± 4.62 |
0.001 |
|
Cavus |
Talo-first metatarsal angle (lateral) |
14.00 ± 0.00 |
10.00 ± 0.00 |
0.005 |
|
Equinus |
Tibio-calceneal angle |
13.45 ± 4.9 |
23.7 ± 1.59 |
0.001 |
The ROC curve for the angle difference to choose casting and sensitivity, specificity and area under the curve were presented in Table 6, Figures 1 and 2. For adduction, when the talo-first metatarsal angle (AP view) showed a difference of more than 18 degrees the need for casting with 100 % sensitivity and only 57.1 % specificity. Regarding the equinus deformity, the tibio-calcaneal angle difference of > 20 degrees indicates the need for casting with a sensitivity and specificity of 100 % (Fig. 5 and 6).
Table 6
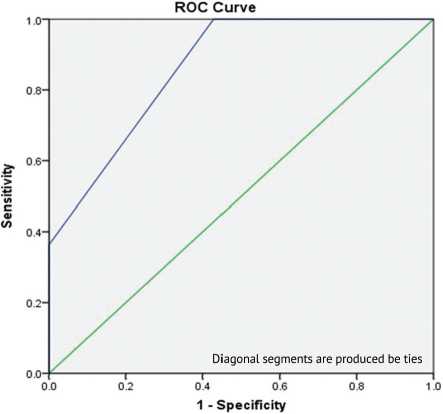
Fig. 5. ROC curve results for talo-first metatarsal angle (AP)
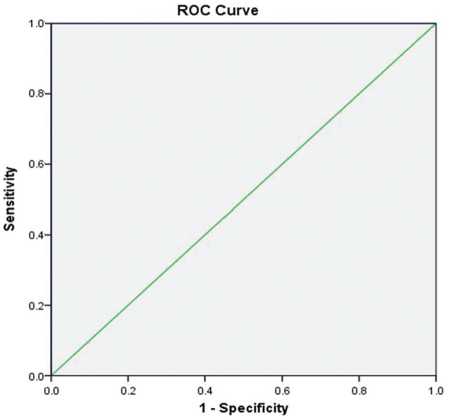
Fig. 6. ROC curve results for the tibio-calcaneal angle
ROC curve for the angle difference to choose casting and sensitivity, specificity and area under the curve
|
Variables |
Cut off point |
Sensitivity |
Specificity |
AUC |
|
|
Adduction |
Talo-calcaneal angle |
> 18 |
100.0 |
57.1 |
86.4 |
|
Equinus |
Talo-first metatarsal angle (ap) |
> 20 |
100.0 |
100.0 |
100.0 |
DISCUSSION
Congenital talipes equinovarus (CTEV), commonly known as clubfoot, is a complex pediatric orthopaedic condition characterized by musculoskeletal deformities, primarily involving the ankle and foot [1]. This study aimed to evaluate the utility of stress radiographs in assessing residual deformities in clubfoot patients and to determine their role in guiding treatment decisions between surgical and non-surgical interventions.
The study population included 45 patients with a mean age of 1.7 years, predominantly male (73.3 %), with nearly half having a history of consanguinity (46.7 %) and a quarter reporting a positive family history of clubfoot (24.4 %) (Table 1). These findings align with previous literature indicating a male predominance and a higher prevalence in populations with consanguineous marriages, suggesting a genetic predisposition [12]. Genetics likely has a role to play, although a specific gene alteration remains unclear. Research shows that 24.4 % of cases have an associated family history, though it has not identified a definite mode of inheritance [1].
Unilateral involvement was significantly more common (80 %) than bilateral cases (20 %) (Table 2), which is slightly different from the existing epidemiological data by 1) who found that clubfoot is usually bilateral in more than 50 % of the cases. Among residual deformities, equinus was the most frequent (85.2 %), followed by adduction (66.7 %) and cavus (14.8 %). This pattern reflects the classic presentation of clubfoot, where equinus and adduction are typically the most persistent deformities [13].
Table 3 demonstrates a statistically significant improvement in key radiographic angles following the application of stress. Notably, the talo-calcaneal angle (associated with varus deformity) significantly decreased from 25.25º to 17.25º ( p = 0.001), indicating improved alignment. Similarly, significant reductions were noted in the talo-first metatarsal angles (AP and lateral views) for adduction and cavus deformities ( p = 0.001 and p = 0.002, respectively), and in the tibio-calcaneal angle for equinus ( p = 0.001). These findings suggest that stress radiographs offer an objective and quantifiable method for assessing the flexibility and severity of residual deformities, as supported by S.N. Sambandam et al. (2016) and J. Li et al. (2024) who emphasized the value of dynamic radiography in treatment planning [9, 14].
Interestingly, nearly half of the patients (48.1 %) required surgical intervention, while 51.9 % were managed with casting (Table 4) and this is in line with the findings from J.A.F. Recordon et al. (2021) [15].
A significant association was found between the magnitude of angular change under stress and treatment modality. In particular, greater angle differences were consistently associated with conservative management (e.g., adduction deformity angle difference: 24.0º in the casting group vs. 16.0º in the surgical group, p = 0.001). This pattern suggests that greater flexibility under stress may predict successful casting outcomes, a concept supported by S.N. Sambandam et al. (2016), and R. Gunalan et al. (2016) who advocated for stress testing to differentiate flexible from rigid deformities [9, 16] .
The ROC analysis (Table 6, Fig. 1 and 2) confirmed the diagnostic utility of angle differences in guiding treatment. The talo-first metatarsal angle (AP view) had an AUC of 86.4 %, with a cutoff of > 18° indicating surgery with 100 % sensitivity. Similarly, the tibio-calcaneal angle in equinus deformity had perfect sensitivity and specificity at a > 20° difference (AUC = 100 %). These findings highlight the excellent predictive power of stress radiography for surgical decision-making, echoing similar conclusions by A. Kappel et al. (2020) and C. Radler et al. (2007) who demonstrated that rigid deformities with minimal radiographic response to stress necessitated operative correction [17, 18].
Overall, this study provides robust evidence supporting the int Stress radiographsegration of stress radiographs into routine evaluation of residual clubfoot deformities. By quantifying angular changes, clinicians can make more informed decisions regarding the need for surgery, potentially avoiding unnecessary operative interventions in cases amenable to casting. This approach may also standardize treatment across different settings and improve outcomes through earlier identification of rigid deformities.
Despite its strengths, this study has several limitations. The relatively small sample size may limit the generalizability of findings. Additionally, interobserver variability in radiographic interpretation was not assessed, which could influence angle measurements. Lastly, long-term functional outcomes were not evaluated, which are critical to understanding the ultimate efficacy of surgical versus conservative approaches.
CONCLUSIONS
The study highlights that clubfoot is more prevalent in male patients and often presents as a unilateral deformity. The most common residual deformities observed are equinus and adduction. Stress radiographs play a crucial role by showing significant angular changes that help evaluate deformity flexibility and severity. Larger angular differences indicate better flexibility and successful outcomes with casting, while smaller differences suggest the need for surgical intervention. Specific angle thresholds, like a talo-first metatarsal angle difference < 18° and a tibio-calcaneal angle difference > 20°, reliably predict the necessity for surgery with high sensitivity and specificity. Overall, stress radiographs are validated as an objective tool for assessing and guiding treatment decisions for residual clubfoot deformities.
Conflicts of interest The authors declare no conflict of interest regarding this article.
Funding None.
Ethical approval The Medical Ethical Committee of The College of Medicine, University of Thi-Qar approved this study (no. 7/54/142 on 27/2/2024).
