The role of monocyte chemotactic protein-3 (MCP3) in pyelonephritis patients in Al- Najaf governorate, Iraq
 in pyelonephritis patients in Al- Najaf governorate, Iraq")
Author: Al-janabi D.R.A., Aljanaby A.A.J.
Journal: Cardiometry @cardiometry
Section: Original research
Article in issue: 31, 2024.
Free access
Pyelonephritis is a serious disease that is widespread in Iraq and is mostly caused by Gram-negative bacteria, which are highly contagious and can spread from an infected person to others. The aim of this article was to evaluate the immunomodulatory role of Monocyte chemotactic protein-3 (MCP3) in the blood serum of patients with acute pyelonephritis and chronic pyelonephritis. A group of patients suspected of having nephritis were sampled in Najaf city, Iraq. Clinical and biochemical tests were performed to confirm their infection. Where 30 patients had acute pyelonephritis and 30 patients had chronic pyelonephritis, in addition to 29 healthy people who were considered control. MPC-3 was measured in the serum of the affected person using ELISA technology. MPC3 levels were significantly elevated (P
Monocyte chemotactic protein-3 (mcp3), acute pyelonephritis, chronic pyelonephritis
Short address: https://sciup.org/148328837
IDR: 148328837 | DOI: 10.18137/cardiometry.2024.31.105109
Text of the scientific article The role of monocyte chemotactic protein-3 (MCP3) in pyelonephritis patients in Al- Najaf governorate, Iraq
Cardiometry; Issue 31; May 2024; p. 105-109; DOI: 10.18137/ cardiometry.2024.31.105109; Available from:
Pyelonephritis infections are more common in patients who suffer from kidney failure compared to other kidney diseases [1] and is an inflammation caused by bacteria that primarily effects the interstitial area and the renal pelvis or, less often, the renal tubules [2], [3]. It is one of the most common renal diseases, pyelonephritis cases are classified to acute and chronic [4]. To diagnose pyelonephritis, physicians must rely on evidence of urinary tract infection (UTI) from urinalysis and culture, along with signs and symptoms suggesting upper urinary tract infection (fever, chills, flank pain, nausea, vomiting, and costovertebral angle tenderness) [5]. The most common causative organism is Escherichia coli , but Proteus , Pseudomonas, Staphylococcus aureus , and Enterococcus faecalis (formerly Streptococcus faecalis ) may also cause this infection[6]. The risk of pyelonephritis has increased in people with obstruction of the ureters, diabetes and in people with a weakened immune system which reduces the body’s ability to combat infection[7] .
Cytokines they are classified into lymphokines (cytokines that are secreted by T cells and regulate the immune response), proinflammatory cytokines (cytokines that amplify and perpetuate the inflammatory process), growth factors (cytokines that promote cell survival and result in structural changes in the airways), chemokines (cytokines that are chemotactic for inflammatory cells) and anti-inflammatory cytokines (cytokines that negatively modulate the inflammatory response) [8], [9]. Human Monocyte Chemotactic Protein 3 (MCP-3) also known as Chemokine Ligand 7 (CCL7) (CC Motif) has been reported to interact with several CC chemokine receptors [10]. Monocyte chemotactic protein 3 (MCP-3) belongs to the MCP subgroup of CC chemokines that are chemoattractants and attractants for various types of leukocytes [11]. Full-length CCL7 is composed of 99 amino acids after transcription and translation and contains a 23-amino acid signal peptide [12].
2. MATERIALS AND METHODS: 2.1. Ethical Consideration
It was approved by the Institutional Ethics Committees of the College of science at the University of Kufa and the Scientific Committee for Research in the Health Department of Najaf.
2.2. Patients
The study was conducted in the laboratory of the College of Medical Technologies, Islamic University in Najaf, Iraq, where 89 samples were collected from people distributed into three groups: people with acute pyelonephritis, people with chronic pyelonephritis, and people in normal health in the period between April and December 2023. Ages Participants (18-45 years) All patients were diagnosed by specialist physicians in Al-Hakim General Hospital, as having pyelonephritis, and all samples were collected in sterile conditions. The concentration of the immune marker was measured by an immunoassay called enzyme-linked immunosorbent assay (ELISA) to estimate Monocyte chemotactic protein-3 (MCP3) levels in all groups of subjects. For the determination of MCP-3 in blood serum, the Human MCP-3 ELISA kit (Catalog No.: EKHU 0134) by MELSIN / China was used, and the serum Human MCP-3 was estimated according to the method described by the kit instruction.
2.3. The inclusion criteriaand exclusion criteria
2.4. Statistical analysis
SPSS statistical package version 26 was utilized to conduct a data analysis.P-value less than 0.05 considered significantly [13][14]
3. RESULTS
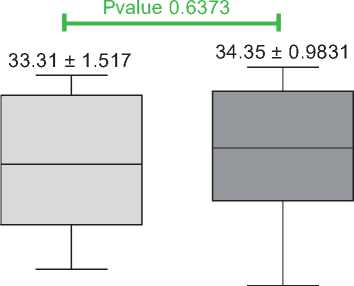
Figure (1) shows the statistical analysis regarding the ages of the healthy control group, which was medium aged (33.31 ± 1.517), and the group with patients infected with pyelonephritis, medium aged (34.35 ± 0.9831), the results showed that there were no statistically significant differences (P 0.6373). While figure 106 | Cardiometry | Issue 31. May 2024
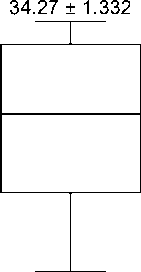
(2) indicated that there was no significant increase (P 0.4596) in age in relation to sex (males and females), the medium aged of females was (34.27 ± 1.332), while the medium aged of males was (34.48 ± 1.446).
50 -1
40 J
w
CD
£ 30 H
W Q.
О
CD
□) 20 J
Ф
<
10-I
0J------------1--------
Total control
-----------------------1-----------------------
Total patients
Figure (1) Medium of age in pyelonephritis patients and healthy controls
P value 0.4596
50 -I
40 ч
30 4
20 J
34.48 ± 1.446
10H
0J---------------1-------------------------------1-----
Male Female
Figure (2) Medium of age in total female and male
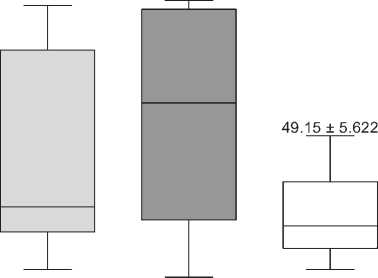
The results showed that there was significant increase (P < 0.0001) in total (Monocyte Chemotactic Protein 3) serum concentration in patients infected with pyelonephritis (113.0±9.338 pg/ml) as compared with control (49.15± 5.622 pg/ml) (Figure 3). Also, the results demonstrated that there was a significant increase (P 0.0006) in serum concentrations of MCP-3
in patients infected with acute pyelonephritis (96.82 ± 12.5 pg/ml) as compared with control (49.15± 5.622 pg/ml). Also, the results proved that there was higher level of MCP-3 in patients infected with chronic pyelonephritis (129.3 ± 13.43 pg/ml) as compared with control with significant differences (P < 0.0001) While, the results of the current study indicated that there was significant differences (P 0.0411) of MCP-3 levels in serum of patients infected with acute pyelonephritis and chronic pyelonephritis (Figure 4).
250 -I
E 200 4
U) Q.
°? Q. О s 4-O (0 Ф > о
E 5
50 4
— . -***
Pvalue < 0.0001
49.15 ± 5.622
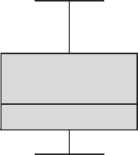
113.0 ± 9.338

Total control
Total patients
Figure (3) MCP-3 levels in serum of total patients infected with pyelonephritis caused by E.coli and control.
I 200 4
O) Q.
°?
6 150 s о w
> 100
CD
E □
CD 50 J
Pvalue 0.0006
***
Pvalue 0.0411 * Pvalue < 0.0001
96.82 ± 12.50 129.3 ± 13.43
T------------------------------1------------------------------г
Acute infection Chronic infection Total Control
Figure (4) MCP-3 levels in serum of patients infected with acute pyelonephritis and chronic pyelonephritis by E.coli and control.
4. DISCUSSION:
Pyelonephritis infections has been studied as one of the most common kidney diseases, especially in Iraq, specifically in Najaf Governorate, and it affects females, males, and all ages.[1]. In our study, the age of the patient was defined in a specific category from 18 to 45, because at these ages their immune system was complete, in addition to that they did not suffer from other functional diseases when compared to elderly people over 50 years of age[15]. The MCP-3 immune marker was studied for what It has an important action and effect against infections in general [16]. This is what became clear to us when its percentage in patients was much higher and with a significant difference when compared to healthy people. It also increased proportionally with the progression of the disease, so the results showed that patients with chronic kidney inflammation were more Concentration in patients with acute kidney disease, which indicates its action is similar to some interlequins, which are increased in chronic diseases when compared with acute diseases [17]. MCP-3 is one of the most mul-tipotent chemokines because it activates all types of white blood cells, by binding to at least four different chemoreceptors [18]. Only small amounts of MCP-3 are stimulated in different cell types by endogenous (cytokines) or exogenous (bacteria, viruses) factors. However, this omnipotent chemokine, which can be induced in most parts of the body, may play an important role in normal homeostasis as well as in many diseases including cancer, autoimmune diseases, and chronic inflammation [19], [20]. MCP-3 is expressed by endothelial cells and monocytes after stimulation with interleukin (IL)-1b, tumor necrosis factor alpha (TNF-a), interferon (IFN)-g, lipopolysaccharide (LPS), fibroblasts and mononuclear cells [21].
These chemoattractant cytokines belong to the MCP/eotaxin subfamily of inflammatory and immune regulatory beta chemokines. Within this group are five human (MCP-1, MCP-2, MCP-3, MCP-4 and eotaxin). They share 51-78% amino acid homology (Boshtam et al. , 2017; Singh et al. , 2021). The four MCPs activate monocytes via CC chemokine receptor (CCR) 2. In addition, MCP-3 and -4 activate both CCR1 and CCR3, while MCP-2 activates CCR5 [23]. Human MCP-3 also activates monocytes or macrophages to halt the growth of certain tumor target cells by supporting the formation of the tumor microenvironment and facilitating tumor invasion and metastasis, although some studies suggest that CCL7 has tumor suppressor effects, monocyte chemotactic and activating factor (MCAF) [24]. MCPs are major attractants for human CD4 + and CD8 + T lymphocytes and play a key role in recruiting activated T lymphocytes to sites of infection [23].
Chemokine (CC Motif) Ligand 7 (CCL7), however, an abnormal increase in CCL7 aggravates the progression of various disorders, such as lesional psoriasis, acquired immunodeficiency syndrome, acute neutrophilic pneumonia, and pulmonary fibrosis [25]
5. CONCLUSIONS
In Iraq – Najaf Governorate – the results of the current study indicated that there are significant differences in the levels of MCP-3 patients with pyelonephritis when compared with healthy controls, also showed that MPC-3 is related to pyelonephritis and can be used to help in diagnose the disease.
Thanks:
To the doctors who specialize in nephrology in Najaf Governorate, especially Dr. Mustafa Hassan Al-Hakim and Dr. Haider Shawkat Al-Shakraji.
References The role of monocyte chemotactic protein-3 (MCP3) in pyelonephritis patients in Al- Najaf governorate, Iraq
- B. M. Muhammad-Baqir, A. A. Fattah, D. R. A. Al-janabi, and A. A. J. Aljanaby, “The prevalence study of patients infected with pyelonephritis by in Al Najaf Governorate, Iraq,” in BIO Web of Conferences, EDP Sciences, 2023, p. 5049.
- S. Siriwardana and C. Piyabani, “Role of Imaging in Renal Infections: A Narrative Review,” 2023.
- J. J. Djuraevich, “Gestational Pyelonephritis in Pregnancy,” Am. J. Pediatr. Med. Heal. Sci., vol. 2, no. 1, pp. 348–352, 2024.
- S. Woo et al., “Clinical factors distinguishing renal infarction from acute pyelonephritis: A randomly matched retrospective case-control study,” Am. J. Emerg. Med., vol. 72, pp. 88–94, 2023.
- R. Yamashita, Y. Izumi, K. Nakada, and J. Hiramoto, “Utility of urinary presepsin in the diagnosis of pyelonephritis: a cross-sectional study,” BMC Infect. Dis., vol. 23, no. 1, p. 365, 2023.
- D. R. A. Al-janabi and A. A. J. Aljanaby, “Bacteriological investigation of pyelonephritis in AL-Najaf Governorate, Iraq: a cross-Sectional study,” in BIO Web of Conferences, EDP Sciences, 2024, p. 3014.
- H. Trujillo-Santamaría et al., “A novel mortality risk score for emphysematous pyelonephritis: A multicenter study of the Global Research in the Emphysematous Pyelonephritis group,” Curr. Urol., vol. 18, no. 1, pp. 55–60, 2024.
- K. Gulati, S. Guhathakurta, J. Joshi, N. Rai, and A. Ray, “Cytokines and their role in health and disease: a brief overview,” Moj Immunol, vol. 4, no. 2, p. 121, 2016.
- J. J. O’Shea, M. Gadina, and R. M. Siegel, “Cytokines and cytokine receptors,” in Clinical immunology, Elsevier, 2019, pp. 127–155.
- S. She, L. Ren, P. Chen, D. Chen, and Y. Wang, “Functional roles of chemokine receptor CCR2 and its ligands in liver disease,” Front. Immunol., vol. 13, p. 812431, 2022.
- S. Zhu, M. Liu, S. Bennett, Z. Wang, K. D. G. Pfleger, and J. Xu, “The molecular structure and role of CCL2 (MCP‐1) and C‐C chemokine receptor CCR2 in skeletal biology and diseases,” J. Cell. Physiol., vol. 236, no. 10, pp. 7211–7222, 2021.
- Y. Liu, Y. Cai, L. Liu, Y. Wu, and X. Xiong, “Crucial biological functions of CCL7 in cancer,” PeerJ, vol. 6, p. e4928, 2018.
- D. R. A. Al-Janabi, A. A. Fattah, A. A. J. Aljanaby, and W. H. Alhissnawy, “Comparison of Some Blood Parameters and Vitamin D3 for Patients with Pyelonephritis and Renal Failure in Najaf Governorate, Iraq,” Ren. Fail., vol. 91, no. 50.93, p. 10.
- D. R. A. Al-janabi, Y. A. Shallani, L. A. D. Albakaa, and A. A. J. Aljanaby, “Prevalence of types of cancer in Najaf Governorate and comparison of leukemia with other types,” J. Biomed. Biosens., vol. 4, no. 2, pp. 1–10, 2024.
- H. M. H. Al-aaraji, M. R. Mansor, and D. R. A. Al-janabi, “The role of IL-6, IL-8 and TNF-α in COVID-19 patients in Karbala Governorate,” in E3S Web of Conferences, EDP Sciences, 2023.
- S. Singh, D. Anshita, and V. Ravichandiran, “MCP- 1: Function, regulation, and involvement in disease,” Int. Immunopharmacol., vol. 101, p. 107598, 2021.
- S. M. Y. Mhana and A. A. J. Aljanaby, “Bacteriological and Immunological study of kidney failure patients infected with urinary tract infections,” in E3S Web of Conferences, EDP Sciences, 2023, p. 3110.
- H. Strang et al., “Role of cytokines and chemokines in wound healing,” in Wound healing, tissue repair, and regeneration in diabetes, Elsevier, 2020, pp. 197–235.
- Y. Bao and X. Zhu, “Role of chemokines and inflammatory cells in respiratory allergy,” J. Asthma Allergy, pp. 1805–1822, 2022.
- R. Yudhawati and K. Shimizu, “PGE2 produced by exogenous MSCs promotes immunoregulation in ARDS induced by highly pathogenic influenza a through activation of the wnt-β-catenin signaling pathway,” Int. J. Mol. Sci., vol. 24, no. 8, p. 7299, 2023.
- T. C. Dos Santos et al., “Approaches of marine compounds and relevant immune mediators in Autism Spectrum Disorder: Opportunities and challenges,” Eur. J. Med. Chem., p. 116153, 2024.
- M. Boshtam, S. Asgary, S. Kouhpayeh, L. Shariati, and H. Khanahmad, “Aptamers against pro-and anti-inflammatory cytokines: a review,” Inflammation, vol. 40, pp. 340–349, 2017.
- A. Mantovani, S. Sozzani, P. Proost, and J. Van Damme, “The monocyte chemoattractant protein family,” in Chemoattractant ligands and their receptors, CRC Press, 2020, pp. 169–192.
- L. Wang, J. Lan, J. Tang, and N. Luo, “MCP-1 targeting: Shutting off an engine for tumor development,” Oncol. Lett., vol. 23, no. 1, pp. 1–9, 2022.
- A. Gowhari Shabgah, F. Jadidi-Niaragh, H. Mohammadi, and J. Gholizadeh Navashenaq, “The role of atypical chemokine receptor D6 (ACKR2) in physiological and pathological conditions; friend, foe, or both?,” Front. Immunol., vol. 13, p. 861931, 2022.
