A Case of Surgical Treatment of Lower Molars in a Mesolithic Sample from a Cemetery on the Yuzhny Oleniy Ostrov, Karelia, Russia

Author: Zubova A.V., Pikhur O.L., Moiseyev V.G., Malyutina A.A., Obodovskiy A.V., Kalmina O.A.
Journal: Archaeology, Ethnology & Anthropology of Eurasia @journal-aeae-en
Section: Anthropology and paleogenetics
Article in issue: 4 т.51, 2023.
Free access
Here, we present the earliest case of surgical treatment of mandibular permanent molars known in Northern Eurasia. It concerns an aged woman buried at a Mesolithic cemetery on the Yuzhny Oleniy Ostrov (Island) in Lake Onega, southern Karelia, 8250–8050 cal BP. Our objective was to reconstruct the technology of surgical intervention, and to diagnose and describe the underlying condition. To do this, we carried out an examination of teeth and bone tissues of the upper and lower jaws and a traceological analysis of identified lesions. As we found, in the last few months of her life, the woman underwent several dental operations, including the extraction of the lower left third molar and, in a stepwise fashion, of fragments of the distal part of crown and lingual part of the distal root of the lower right first molar. The first operation was successful—the woman survived for at least two months after it had been performed. The second operation was also successfully performed at least two months before death, likely immediately after the trauma. The mesial part of the crown was removed just before death. No ancient cases where fragments of an injured tooth were removed are known to us. The removal of the lower third molar can be compared only with the earliest previously known case, described in a sample from the Pucará de Tilcara fortress in Northern Argentina (15th–16th centuries AD). Indications for surgery partly coincide in both cases, and include complications of apical periodontitis and the development of osteomyelitis. However, the technology of surgery and its logistics are different.
Mesolithic, tooth extraction, osteomyelitis, paleopathology, septic cavernous sinus thrombosis
Short address: https://sciup.org/145146964
IDR: 145146964 | DOI: 10.17746/1563-0110.2023.51.4.135-141
Text of the scientific article A Case of Surgical Treatment of Lower Molars in a Mesolithic Sample from a Cemetery on the Yuzhny Oleniy Ostrov, Karelia, Russia
Cases of dental treatment are rarely described in paleoanthropological studies and are, thus, of a great interest for researchers. A thorough analysis of such cases can help to reconstruct the techniques of ancient dental treatment, contributing to the history of dentistry, as well as to the knowledge regarding human views about their body in the past. Some evidence of oral hygiene and dental treatment are found as early as in the Middle Paleolithic. Traces of the use of toothpicks for cleaning the dental spaces and, possibly, reducing the pain accompanying inflammatory diseases have been reported from various localities in Eurasia (Lozano et al., 2013). In a sample from Chagyrskaya Cave (Altai Mountains, Russia), a case of scraping of a carious cavern by a stone tool was detected (unpublished data of A.V. Zubova, L.V. Zotkina, and K.A. Kolobova, being prepared for publication).
There is evidence of the use of toothpicks in the Upper Paleolithic (see, e.g., (Alt, Pichler, 1998: 404, fig. 15)). A case of treatment of caries of the lower third molar by scraping the cavern by a stone edge was described at Villabruna in northern Italy (Oxilia et al., 2015).
In the Neolithic, the techniques of dentistry became even more diverse: drilling of carious cavities (Coppa et al., 2006), trephination of odontogenic abscesses (Bennike, Fredebo, 1986), and, probably, filling of teeth fissures with beeswax to reduce tooth sensitivity (Bernardini et al., 2012). But for quite a long time, between the Late Pleistocene and the period of the dispersal of Neolithic tribes in Europe, there have been no skeletal evidence of dentistry. In the present study, we describe the first case of surgical dental treatment for the Mesolithic of Northern Europe (and North Eurasia in general).
Traces of dental treatment were detected in an individual buried at the island of Yuzhny Oleny Ostrov in the Onega Lake (South Karelia). The necropolis is located in the northwestern part of a small island nearby a larger (Klimenets) island, and contains more than 170 burials. The number of burials might originally exceed 400, but most of them were occasionally destroyed in modern times. The burials are predominantly single (116), while double (16) and triple (3) burials are much rarer. These lie in boulder-pebble Quaternary sediment at a depth from 0.5 to 1.22 m (Gurina, 1956: 11–15). The deceased were typically buried in an extended supine position, with the head eastwards, with small deviations to the southeast or northeast. Several unique vertical burials were excavated as well. Most of the skeletons were thickly covered with ocher (Ibid.: 16). The site belongs to the Late Mesolithic Onega culture, and dates to the range from 8250 to 8050 cal BP. The necropolis is believed to have been used by various Mesolithic Onega populations as a common burial ground. The tribes might gather at the island in order to resolve the issues of using the hunting and fishing grounds that became acute due to the climate crisis related to the 8200 BP cooling event (Schulting et al., 2022).
The traces of dental treatment discussed in the present article were detected in the skull of a female from burial 142—a single burial at the northern margin of the necropolis. The deceased was placed to the grave in an extended supine position, with her head to the southeast. Her arms were bent in the elbows, while the hands were placed on the pelvis. Grave goods from the burial included only a bone borer and a fragment of bone arrowhead; the skeleton was thickly covered with ocher (Gurina, 1956: 412–413).
The aim of the present study was to reconstruct the techniques of the dental treatment applied to the dentition of the female. We set out to diagnose and describe the pathogenesis of the diseases that evoked the treatment, and to compare our cases with those published previously.
Material and methods
The skull from burial 142 (MAE collection, No. 5773-74) was studied. The specimen is well-preserved, with some small post-mortem damage. The cortical layer of the occipital bone displays subtle breaks around foramen magnum ; the sphenoid bone is destroyed; a small hole is present in the central part of the cranial vault. The right zygoma and mandible (two fragments) were remodeled with wax. The cortical layer of the anterior wall of the maxilla is partially broken; the roots of the frontal teeth and first molars are visible. The roots of the mandibular lateral incisors and canines are partially naked; the upper left central incisor, lower left canine, and lower first premolar were lost post-mortem. Teeth were covered with wax-rosin mastic and plasticine, which cannot be removed completely.
The sex of the individual could not be determined based on morphological criteria, since the innominates were severely damaged and thus not informative. The results of genetic analysis showed that the individual was a female (W. Haak, personal communication). The age-at-death is estimated as older than 50 years, based on complete obliteration of the endocranial sutures and severe dental wear, which led to the loss of more than a half of the teeth crowns height.
The diagnostic of the diseases that led to the dental surgery was based on both visual inspection of the dentition and CT imaging. The CT was performed using the direct geometric magnification technique at the Department of Electronic Instruments and Devices of LETI (St. Petersburg Electrotechnical University) by MRCT-04 scanner (scanning parameters: X-ray tube voltage 140 kV, amperage 50 μA, no filter, slice thickness 0.1 mm).
For reconstructing the surgical techniques, traceological analysis of the dental and bone lesions was carried out at the Laboratory of the Experimental Traceology of the Institute for the History of Material Culture RAS, using a binocular microscope MBS-9 (oblique illumination, magnification up to ×98). A multifocal photographical fixation of the traumatic lesions and surgical manipulations was performed using the CANON EOS Utility software. The resulting image was aggregated in the Helicon Focus 5.2 software.
Results
Paleopathological description of the dentition. Manifestations of chronic generalized periodontitis (II–III degree) were detected during the assessment of general condition of the dental system of the deceased. Both maxillary and mandibular alveolar margins are blunt; the alveolar ridges between the incisors and canines are porous. The roots of the mandibular frontal teeth are naked from both vestibular (3.2 mm on average) and lingual (3 mm) surfaces (post-mortem damage disregarded). The same values for the maxillary teeth: 3.5 and 2.5 mm, respectively. All the teeth exhibit dental calculus, many display pre-mortem chipping (the largest defects are observed in the molars). No visible signs of caries are present.
Traces of surgery. Our traceological analysis detected signs of intentional manipulations with two teeth of the mandible: right first and left third molars. In the area of the socket of the latter, a large lesion 17.32 mm long and 11.26 mm deep is observed. This was likely a result of the extraction of the tooth and lingual alveolar wall (Fig. 1). Traces of the initial penetration of a cutting tool were detected in the distal part of the socket (Fig. 1, a); the incision of the soft tissue and bone was then continued in the mesial direction (Fig. 1, b). The cut fragment was removed together with the tooth. Bone regeneration and pre-mortem polishing of the internal side of the incision are observable at the lesion. Newly formed cancellous bone is present at the bottom of the socket (Fig. 1, c). Enamel wear and regeneration of the edge of incision suggest that the individual have survived for at least several months after the surgery.
The lower right first molar was crushed pre-mortem simultaneously with its antagonist, which was likely due to biting a hard object. The upper tooth exhibits only a partial chipping of the crown, while the lower molar crushed completely in the longitudinal direction and lost the distal part of the crown and the distal root (Fig. 2). Two sets of lesions were detected in the vestibular part of its socket (Fig. 3). The first set includes chippings, 1.2 mm in size on average, that surround the apical part of the cell of the distal root (Fig. 3, a ). The force that caused those was directed from inside the socket to the external surface of the wall. Those lesions are likely a result of removing of a broken fragment of the root.
The second set of lesions includes traces of cutting the cell of the mesial root from the vestibular side. A jagged
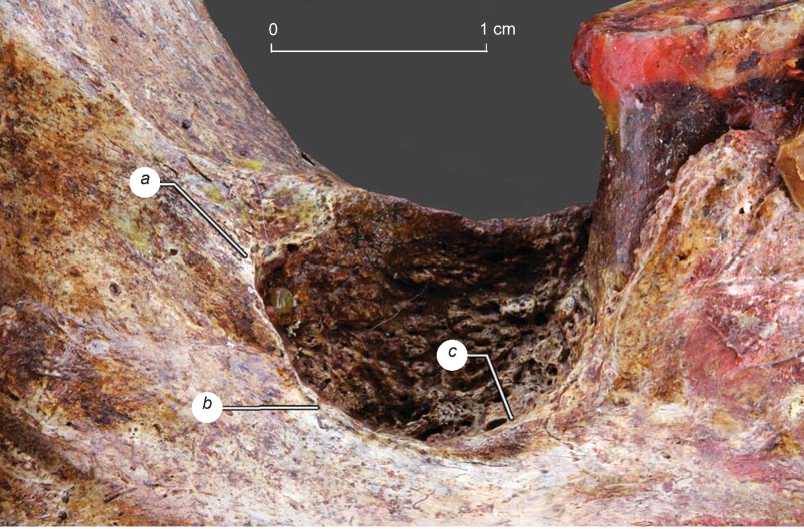
Fig. 1. Macrophotography of the socket of the extracted lower left third molar. Photo by A.A. Malyutina. a – trace of the initial penetration of the cutting tool; b – manifestations of the bone incision; c – newly-formed cancellous bone.

Fig. 2. A fragment of the right half of the mandible with a damaged lower first molar. Photo by A.A. Malyutina.
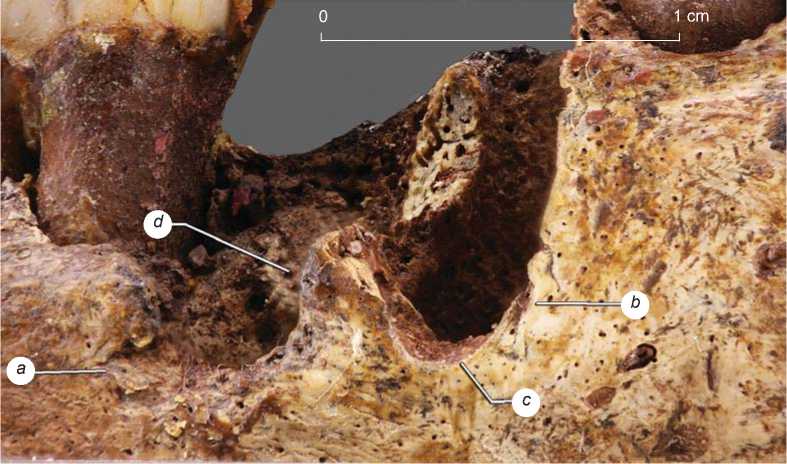
Fig. 3. Macrophotography of the signs of the surgery in the area of the lower right first molar. Photo by A.A. Malyutina.
a – traces of crushing the root; b – trace of the initial penetration of the cutting tool; c – manifestations of the bone incision; d – newly-formed cancellous bone.
indentation is visible in the vestibular surface near the mesial wall of the socket: a trace of the initial incision of bone by a cutting tool with a thin and sharp tip (Fig. 3, b ). The indentation continues as a straight cutting line, which can be traced along the whole preserved apical part of the cell of the mesial root (Fig. 3, c ). Signs of healing both at the chippings and cut marks are absent, but present in the lingual part of the cell of the distal root which is partially filled with spongy bone (Fig. 3, d ).
Reconstruction of the etiopathogenetic mechanisms of development of the diseases which led to the surgery. The lesions observed in the alveoli of the two described molars are the evidence of several dental surgeries carried out during the last several month of the woman’s life. The most large-scale of those was the extraction of the lower left third molar. It was difficult to determine the ultimate cause of the surgery based on a visual assessment only, since the process of bone healing has remodeled the initial lesions. However, the results of CT scanning and a detailed analysis of the general conditions of teeth and bone of the left half of the mandible have facilitated our reconstruction of the pathogenesis of the diseases that might have been the indications for the surgery.
The pathogenetic process was generalized and involved not only the left third molar, but the neighboring teeth as well. As was noted above, the deceased suffered from chronic periodontitis progressing due to the poor oral hygiene. A deep periodontal pocket had formed in the lower left first molar. The poor oral hygiene also led to the development of a carious lesion of the proximal surface of this tooth from the side of the second premolar (Fig. 4, a ). The cavity does not penetrate to the occlusal surface, which remains complete; thus, the lesion could not be detected visually. But it is visible in the CT image as a dimmed spot in the tooth crown of a T-shape and a heterogeneous structure.
Caries had likely progressed for a long time, since the cavity reached the pulp chamber (Fig. 4, b ). It had also triggered chronic pulpitis, which developed into apical periodontitis manifesting by forming of cystogranulomas in all the roots of the tooth (Fig. 4, c ). As all these lesions were quite large, the process had been developing for a long time.
Periodontitis was complicated by chronic osteomyelitis near the lower left first molar. Numerous cavities indicating the latter disease are visible in the CT image of the mandible as dimmed spots (Fig. 4, d). The pathological locus had extended and led to bone resorption not only in the area of the М1, but also of neighboring teeth, including the left third molar. The bone tissue surrounding the socket near the surgery point is porous and exhibits cavities similar to those detected near the first and second molars. A large bone cavity at the bottom of the М3 socket, reaching the mandibular canal, is also a manifestation of osteomielitis (Fig. 4, d). The development of chronic osteomyelitis from the first towards the third molar could have provoked a gradually increasing pain, redness, and swelling of the soft tissues of the maxillofacial area, the formation of fistulas with purulent exudate, increased body temperature, chills, and weakness. These symptoms might have been the cause for the extraction of the tooth.
The manipulations on the lower right first molar were of a different kind. Those were a result of an acute mechanical injury that led (according to the position of the sings of healing) to breaking the tooth crown into at least three parts two of which were extracted pre-mortem at different times. The removal of the lingual part of the distal root and the neighboring part of the crown was likely carried out without using any tool, immediately after the trauma, and at least two months before the death of the individual, which is suggested by a partial filling of the socket by newly formed bone. The mesial part of the root was removed much later, and no signs of healing is visible in this part of the socket. The part of the root was likely firmly anchored in the alveolus after the trauma owing to the pear-like shape of the root, which can be reconstructed based on the socket’s configuration. This had obstructed the surgery and led to the damage to the vestibular surface of the mandible and to forming the chips detected by the traceological analysis.
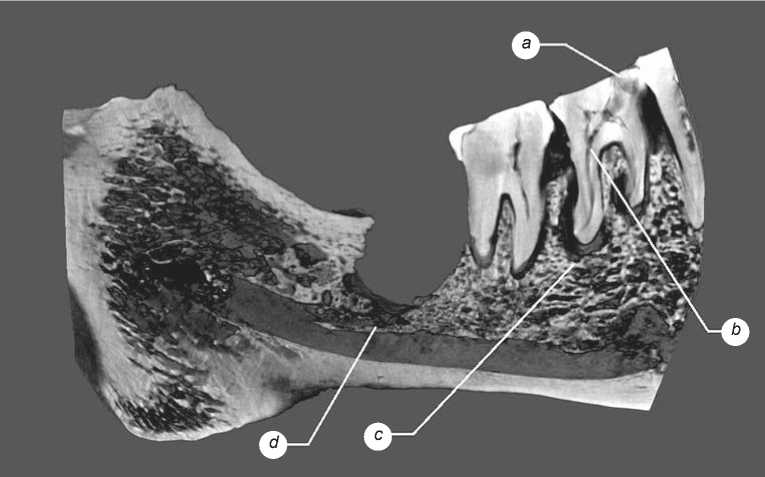
Fig. 4. A CT image of the left side of the mandible. a – carious cavity; b – manifestations of chronic pulpitis; c – area of cystogranulomas; d – cavity in the apical area.
An incision of the mesial root’s socket was performed simultaneously with removing the fragments of the distal root. The purpose of this is unclear: it could be an accessory manipulation during the root extraction, or a separate surgery carried out in order to heal the postoperative complications. Not more than a few days separated the extraction of the root and the incision of the socket: the woman died shortly after those surgeries.
Discussion
A thorough comparative analysis of the case presented in our study is obstructed by the almost complete absence of publications of detailed reconstructions of examples of dental surgery based on archaeological cranial data. The extraction of the lower third molar can only be compared with the most ancient known case (15th–16th centuries AD) described in the sample of the Omaguaca Indians from the Pucará de Tilcara fortress in Northern Argentina (Zubova et al., 2020). An individual from the fortress lost his both lower third molars due to a surgery. A comparison of that with the present study has shown that the indications for surgery were partially similar in both cases: complications of apical periodontitis and the development of osteomyelitis. But the techniques and organization of the surgeries were different.
At Pucará de Tilcara, the surgery was carried out in the plane of the mandibular occlusal surface via a subtle widening of the alveolar contour, followed by scraping of its filling by multiple semi-circular movements of a cutting tool. Every movement led to only a shallow penetration, with the aim to preserve the mandibular body as much as possible (Ibid.: 153). But in the Yuzhny Oleniy Ostrov individual, the tooth was extracted by one or two deep incisions from the lingual part of the mandible, excluding any possibility of preserving the bone tissue. The possibility for the Omaguaca surgeon to carry out the manipulations with multiple delicate movements likely suggests that the patient was immobile. But in our case, on the contrary, the extraction was performed with a minimal number of movements and disregarding the scale of the possible damage. This can suggest that the surgery was carried out rapidly, and no attempt to immobilize or anesthetize the patient was made.
Despite the clear superiority of the system of medical knowledge and technologies in the Inca Empire as compared to the South Karelian Mesolithic tribes, the outcome of the surgery was negative in both cases. While the extraction of the first tooth in the Argentinian individual was successful, the second surgery led to the death of the patient as the surgeon underscored the severity of pathology and missed the deadline for the intervention: this likely resulted in the development of fatal phlegmon and sepsis (Ibid.: 155).
The female buried at Yuzhny Oleniy Ostrov was alive for at least two months after the extraction of the lower third molar. The large alveolar resection stimulated an adequate blood outflow from the area of inflammation and the subsequent wound healing. But the patient died a few days after the removal of fragments of the right first molar. The cause of death was most likely septic thrombosis of the cavernous sinus, which developed as a result of an exacerbation of chronic osteomyelitis provoked by the additional traumatization. The removal of the right first molar’s fragments was carried out with a minimal opening of the socket. This provoked the formation of a hematoma, with its possible subsequent suppuration and spread of the infectious process along the venous outflow paths into the pterygoid venous plexus of the deep region of the face, anastomosing with the cavernous sinus through the system of the ophthalmic veins and the venous plexuses of the oval ( foramen ovale ) and torn ( foramen lacerum ) foramina of the middle cranial fossa.
Thus, the surgical molar extraction could not stop the development of the pathological process, which also partially affected the left mandibular canal. It is feasible that, similar to the Pucará de Tilcara individual, this led to the development of sepsis equally fatal for both a Mesolithic Karelian and an Omaguaca Indian person in the middle of the 2nd millennium AD.
Conclusions
The dental lesions detected in the female skull from burial 142 of the Oleniy Ostrov burial site evidence a unique for the Mesolithic Eurasia case of multiple dental surgical interventions in the same individual. The absence of similar cases in other burials of the necropolis cannot lead to a conclusion regarding a comprehensive and widespread system of surgical knowledge in that ancient population. But even this single case provides an insight about the medical traditions of the North European Mesolithic humans. A comparison of the case of a lower third molar extraction with a similar surgery performed by an experienced Inca surgeon at the Pucará de Tilcara fortress has shown that for almost 8000 years the technique of dental surgery did not influence the outcome of an extraction. The principal factors of the survival of the patient were the quality of the diagnosis determining the timeliness of an intervention; patient’s immune strength; the presence or absence of means of fighting with chronic infectious diseases and postoperative infectious complications. The latter were extremely limited in ancient times and clearly insufficient to ensure the patient’s recovery, in both cases discussed.
Acknowledgement
This study was supported by the Russian Science Foundation, Project No. 21-18-00376.
