A case of systemic connective tissue disorder in a Pazyryk male from the Altai Mountains

Author: Aristova E.S., Chikisheva T.A., Pozdnyakov D.V., Elyasin P.A.
Journal: Archaeology, Ethnology & Anthropology of Eurasia @journal-aeae-en
Article in issue: 3 т.51, 2023.
Free access
We present the results of an anthropological and paleopathological study of a male skeleton from a Pazyryk kurgan 1 burial 1 at Ak-Alakha-1, the Altai Mountains. The archaeological context testifi es to a rather high social status of this person. His appearance was modeled using a modern facial reconstruction method. The combination of craniometric and anthropometric traits indicates a brachycranic Caucasoid type, which predominated in the male population of the Volga-Ural region and Western Kazakhstan in 600–200 BC. The individual suffered from a systemic disorder of the connective tissue affecting virtually all parts of the skeleton. The case is unique, and the condition is diagnosed as DISH—diffuse idiopathic skeletal hyperostosis, possibly caused by grave metabolic and endocrine disorders. Judging by his physical type, the male was not native to the Altai Mountains and belonged to a population that was not genetically adapted to that region. This may account for the severity of the rheumatoid disorder, which was aggravated by 4th degree osteoporosis of lumbar vertebrae and pelvic bones and by traumatic lesions of the shoulder girdle.
Pazyryk culture, Altai Mountains, anthropological reconstruction, rheumatoid diseases, diffuse idiopathic skeletal hyperostosis (DISH)
Short address: https://sciup.org/145146916
IDR: 145146916 | DOI: 10.17746/1563-0110.2023.51.3.140-152
Text of the scientific article A case of systemic connective tissue disorder in a Pazyryk male from the Altai Mountains
Manifestations of musculoskeletal connective tissue diseases (i.e. those of the muscular tendons, synovial joint membranes, ligaments, cartilage and bone tissues) are the most commonly observed markers in a paleopathological study of ancient skeletons. In modern medicine, such diseases are classified as rheumatic. Their common and the most typical manifestations are inflammatory lesions of the joints of both axial and appendicular skeletons. The number of various nosological forms and syndromes is extremely high—from 150 (Adzhigaytkanova, 2013: 5) to 200 (Turdialieva et al., 2015). There are no specific locations mainly affected by the systemic connective tissue diseases: the lesions can be detected in any part of the skeleton.
In the case presented in this study, the whole skeleton was affected by a disease. As such a unique combination of manifestations of connective tissue destruction can be of interest for both medicine and anthropology, we provide a thorough description of the individual.
Importantly, in modern clinical practice, a patient cannot be subjected to whole-body imaging, as in this case permissible exposure limits will be exceeded. Thus, the information regarding the scale and distribution of skeletal lesions not included in classic lists of the main diagnostic criteria of inflammatory rheumatic diseases is of a particular practical value. In the anthropological context, the same information can be employed for reconstructing the aspects of ancient social life that were protecting and supporting physically impaired members of the Pazyryk society. In this line, we set out to integrate the data on the burial rite and morphology of the studied skeleton in order to evaluate the social specific of the individual in the context of the ethno-cultural and geographic diversity of the Pazyryk population.
Material and methods
The male skeleton from the Al-Alakha 1 kurgan burial, located at the basin of the Al-Alakha River, at the Ukok Plateau, was the focus of a complex anthropological and paleopathological study. This site of the Pazyryk archaeological culture was excavated by N.V. Polosmak in 1990 (Polosmak, 1994: 16–60; Naseleniye…, 2003: 17–21). Remains of two individuals were excavated from two burials of the kurgan, one of which— a 45–50-year-old male (burial 1)—is the subject of the present study*.
A complex construction and ritual elements of the burial suggest a high social status of both individuals from the kurgan. The larch log coffins, in which the buried had been placed, were as large as those from the “royal” 1st Pazyryk mound (Rudenko, 1953: 44). These were enclosed by two logworks—internal with five layers of logs and external with seven layers. In a special compartment of the latter, an accompanying burial of nine horses was found. Both coffins contained sets of weaponry, including iron pick-axes with wooden handles, iron daggers in wooden scabbards, gorytos-quivers with arrows, and bows. This kurgan was the first unplundered “frozen” burial of noble warriors-horsemen in the history of research of the Pazyryk culture, with fully preserved burial goods and fragments of outfit (Polosmak, 1994: 16–60; 2001: 45–59).
The male skeleton from burial 1 was almost completely preserved, with only minor post-mortem damage to the anterior wall of the right maxilla and the floor of the right orbit. Several teeth were lost postmortem as well. A craniometric study of the individual (Naseleniye…, 2003: 216–220), as well as a brief general description of the skeleton (Ibid.: 259–261), were published earlier. A facial reconstruction based on the skull of the individual was created employing the methods developed by leading Russian specialists (Gerasimov, 1949, 1955; Lebedinskaya, 1998; Balueva, Veselovskaya, 2004; Veselovskaya, 2015; Nikitin, 2009) to visualize the appearance of the male. The pathological lesions of the skeleton were assessed visually and using computed tomography (CT) imaging.
Anthropological type of the individual
Craniometric data describe the individual as a representative of a brachycranic Caucasoid type with a tall and wide face. Such a combination is found in the craniologically polymorphic Saka population of Western Kazakhstan (Kitov, Mamedov, 2014: 300–349). An analysis of the correlations between craniometric variables in the 6th–4th and 4th–3rd centuries BC samples carried out by Kitov and Mamedov shows that this morphological combination is the basal component of the male population of the Volga-Urals and Western Kazakhstan in the 6th–3rd centuries BC (Ibid.: 177).
The sculptural portrait of the individual (Fig. 1) visualizes the craniometric features mentioned above, as well as his reconstructed somatological traits. The final reconstruction employs the age and pathological lesions of the individual and is supplemented with elements of clothing and jewelry. This reflects the most typical appearance of a representative of the Pazyryk culture.
Pathological status of the individual
Axial skeleton
Cervical spine ( pars Cervicalis ). All the seven cervical vertebrae have survived. Of these, six (except for C2) display large marginal outgrowths, up to 12 mm. In the left occipital condyle, the osteophytes form an almost continuous band 3 to 7 mm wide (Fig. 2, 1 ). In the right condyle, one of the lesions forms a false joint with the anterior arch of the atlas (C1), while another appears as a flat and wide vertical plate (12 × 4 mm). Those osteophytes could severely limit side head tilt. A bone spine at the upper surface of the anterior arch of the atlas and an osteophyte of the right condyle make another false joint. The joint surfaces of the C1 lateral
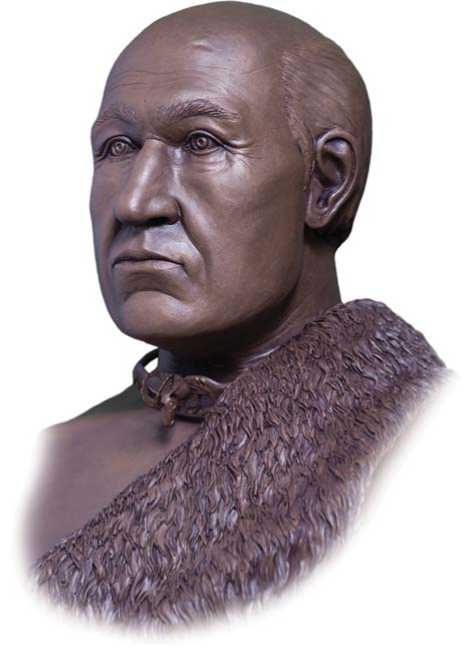
Fig. 1. Facial reconstruction of the male from Ak-Alakha-1 kurgan 1 burial 1.
masses also display substantial marginal outgrowths of the same morphology as the occipital osteophytes (Fig. 2, 2 ). The right mass is affected by osteoporosis, while the left mass is of a decreased size due to the “advent” of the marginal outgrowths.
The axis (C2) displays the least number of lesions among the cervical vertebrae. The superior articular facets was only slightly affected, while the inferior articular processes are porous and lack the cortical bone layer. C2 is fused neither with C1 nor with C3. Thus, manifestations of spondyloarthritis are observed in the lateral atlantoaxial joints, while the medial joint is less affected; the ligament at the apex of the dens is partially ossified (Fig. 3, 1 ).
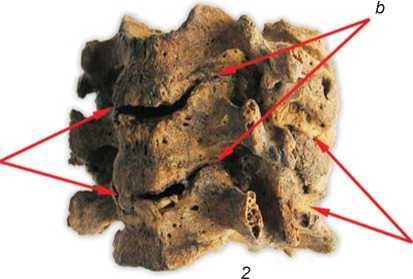
The 3rd to 5th (Fig. 3, 2 ) and 6th to 7th vertebrates are partially fused in the area of the arcuate connections of their bodies. The joints between C5 and C6 are pathologically changed, but preserved. The articular processes of these vertebrae are enlarged to 2–3 cm and display prominent “cauliflower” marginal outgrowths. The joint spaces are present. The fusion of the articular processes has likely occurred due to the growth of the marginal osteophytes towards each other and the ossification of the joint capsule: these turned the posterior parts of the vertebrae into an immobile conglomerate of fused bone structures (Fig. 3, 2 , а ). Neoartrhroses and uncovertebral fusions between the posterior aspects of C3, C4, and C5 are clearly visible (Fig. 3, 2 , b ). New joints between the anterior elevated parts (hamuli) of the C4–C5 bodies and the lower convex surfaces of the upper vertebrae were formed as a result of the thinning and destruction of the intervertebral disc (Zharkov, 1994: 26). The vertebral bodies in some places are connected with vertical or horizontal bone “bridges” (Fig. 3, 2 , c ), located between their margins or even inside the intervertebral space. This indirectly suggests that the new joints were formed in the absence of the intervertebral disc. The intervertebral spaces are substantially narrowed (almost absent). The cervical
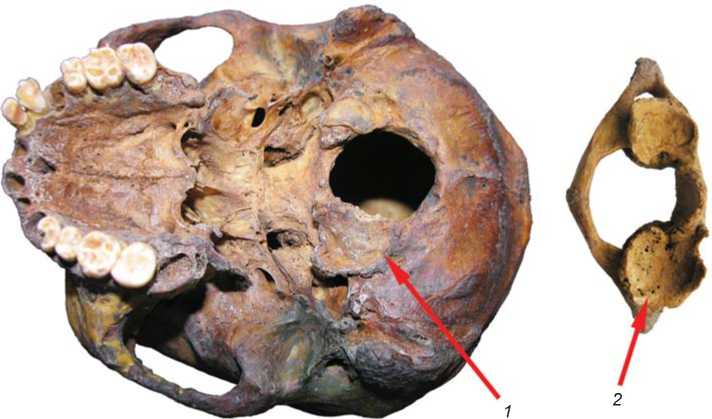
Fig. 2. Deformation of the occipital condyle ( 1 ) and the superior articular fossa of the atlas ( 2 ).

а
Fig. 3. The axis displaying ossification of the ligament of the dens apex ( 1 ); vertebrae 3rd to 5th fused into a bone conglomerate ( 2 ).
a – ossification of the articular capsules; b – uncovertebral fusions; c – bone “bridges” in the intervertebral spaces.
part of the vertebral column is thus severely compressed vertically.
The sequence of the pathological changes in the cervical vertebrae can be tentatively reconstructed as follows. First, the structure of the intervertebral disc was altered, likely due to a chondrosis triggered by extreme physical loadings at a young age. Later, a number of pathological processes began: subligamentous bone formation (osteochondrosis), decrease of the intervertebral spaces, formation and fusion of uncovertebral neoarthrosis, increase of the load on the posterior vertebral parts, spondyloarthrosis, ossification of the connective tissue structures in the area of the intervertebral joints and their complete fusion. These led to a significant limitation of functions and shortening of the neck. A patient with such changes in the cervical spine involuntary displays a “proud” posture, conspicuous to those around him, who might have an impression that the patient is flaunting self-confidence and arrogance (Rokhlin, 1965: 264–267). This severe pathology of the cervical spine makes it really difficult to turn one’s head towards his interlocutor.
Thoracic spine (pars Thoracales). Seven thoracic vertebrae are present, all displaying some pathological changes in the bodies, but not in the articular processes. The articular surfaces of the latter preserve the cortical layer, and some of the surfaces exhibit stand-alone osteophytes up to 7 mm long. Bone outgrowths up to 3 mm long were detected on the margins of the costal facets of the transverse processes (Fig. 4, 1), which were likely an outcome of osteoarthrosis of the costal transverse joints. The costal facets of the vertebral bodies do not display marked pathological manifestations. The spinous processes exhibit bone outgrowths at the supraspinous ligament attachment site (Fig. 4, 2).
The bodies of all of the thoracic vertebrae (right and anterior surfaces) clearly display bony subligamentous layers forming a flat band interrupted in the intervertebral spaces. The band, 3 to 3.5 cm wide, is of a lighter color than the surfaces of the vertebral bodies. The margins and surface of the lesion in the intervertebral space display a typical “candlewax” appearance (Fig. 4, 3 ). This bone formation represents a cast of a fragment of the soft tissue spine, and based on its morphology, it can be hypothesized
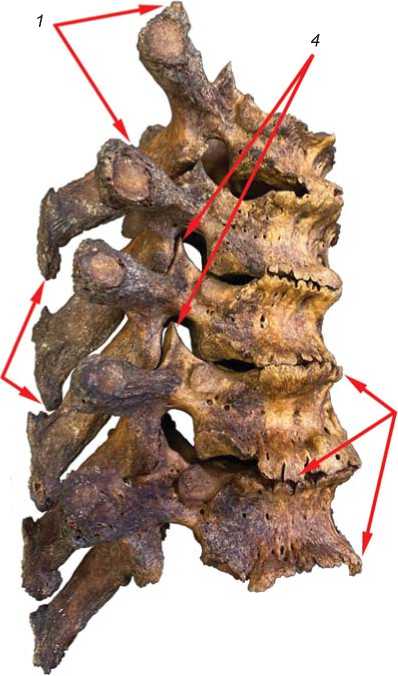
Fig. 4. Thoracic spine.
1 – osteophytes at the margins of the articular facets of the transverse processes; 2 – ossification of the supraspinous ligament; 3 – subligamentous bone deposits, right and anterior;
4 – unaffected intervertebral joints.
with a high probability that the intervertebral discs of the thoracic spine were lowered and bulged aside the margins of the vertebral bodies.
It is well known that such manifestations are typical for the spine pathology entitled “spine idiopathic fixing hyperostosis”, or the “Forestier disease” (Zharkov, 1994: 78; Starkova, Erdes, 2016: 80). The modern clinical literature describes this pathology as a form of non-inflammatory spine lesions (Starkova, Erdes, 2016: 80) similar, according to many formal criteria, to spondylosis (Ivashkin, Sultanov, 2005: 497–501). It must be differentiated from the Bekhterev’s disease (Starkova, Erdes, 2016: 81; Skryabina, Magdeev, Korneeva, 2020: 68–69), for which severe lesions of the intervertebral joints and their fusion (ankylosis) are typical (Ivashkin, Sultanov, 2005: 497). But in the skeleton under study the articular processes are the least affected structures (Fig. 4, 4). In addition, the Bekhterev’s disease is always accompanied by ankylosis of the synovial part of the sacroiliac joins. Morphology of the pelvic bones and their joints is considered below, but it is of note that this part of the skeleton was not affected and the sacroiliac joint space is clearly visible throughout.
The Forestier’s disease affects the thoracic spine first, while the lumbar or cervical vertebrae get affected later. As is detailed below, the right surfaces of the bodies of the lumbar vertebrae also display subligamentous bone formation. The disease is characterized by generalized ectopic ossification of tendons and ligaments not only of the spine, but of the appendicular skeleton as well (Ibid.: 496). In our study case, numerous loci of ossifying entesopathy (i.e. pathologic bone formation at the attachment sites of connective tissue structures— ligaments and capsules of joints, muscle tendons) and hyperostosis were detected. A description of those lesions follows.
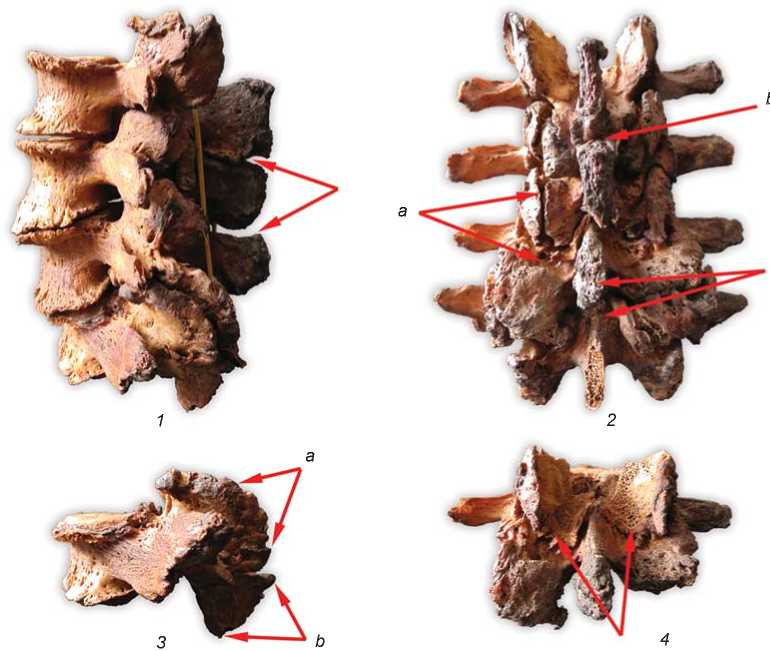
Lumbar spine ( pars Lumbales ). Four lumbar vertebrae (L2–L5) are present. These are extremely light and display marked pathological changes in both bodies and arches. The height of the L5 body is reduced by a third. At the lateral surfaces of the vertebral bodies, a subligamentous bone formation bulging at the intervertebral spaces is clearly visible (Fig. 5, 1 ),
c
Fig. 5. Lumbar spine.
1 – left view (the arrows indicate the false joints between the spinous processes); 2 – posterior view: a – intervertebral joints, b – false joints between the spinous processes, c – newly formed articular facets in the overgrown spinous processes;
3 – L5: a – large “shell-like” articular processes, b – overgrown spinous processes; 4 – L2 (the arrows indicate the articular processes forming a “stand” for the overlying vertebra).
which confirms the diagnosis of the Forestier’s disease (Zharkov, 1994: 77). The intervertebral space between L4 and L5 is almost absent. The bodies display a “fish vertebra” shape in the sagittal plane. Marked hyperlordosis and spondylolisthesis of L4 are observed.
The vertebral arches display huge bone outgrowths located mainly in the articular, spinous and, to a lesser extent, transverse processes. The articular processes are flattened and reach 4.5 cm in diameter; their margins exhibit a wavy “shell-like” outline (Fig. 5, 3 ). The compact layer of the articular surfaces is absent. The lower aspect of the upper articular processes is bent down posteriorly and reminds a “stand” for the upper vertebrae (Fig. 5, 4 ). These changes might reflect the adaptation of the skeleton to extreme physical loading via enhancing the articulations of the vertebrae. The huge articular processes of the individual exhibit numerous vessel pores (even canals in some cases); thus, the observed pathological process began quite early and was developing for at least 10–15 years. From a formal point of view, such vertebral lesions—enlargement, destruction of the chondral and subchonrdal layers, extensive outgrowths of the articular margins—when not accompanied by bone fusions (Fig. 5, 2 , а ), are typical of spondyloarthrosis. But the scale of the changes in this case is impressive. Spondyloarthrosis of any joint develops only in the cases of a substantial functional overload (Ibid.: 67–68). This, in turn, might provoke spondylolisthesis: under excessive loadings, the intervertebral discs, which are the main amortizing structures, collapse, and the upper vertebra just “slide” in the anterior direction.
The spinous processes are enlarged and display large bone outgrowths along the posterior borders, at the supraspinous ligament attachment site. Both their upper and lower margins exhibit clear signs of false joints between the processes (Fig. 5, 1 , 2 , b , c ). Such a phenomenon is known in the clinical practice as the Baastrup syndrome* or the “kissing spine”: the overgrown spinous processes come into contact and gradually form false joints. The pathology is fairly rare, emerges at older age, and is typically accompanied by a lasting and burning pain. Such patients receive fairly long conservative therapy, and then a surgery if the pain is still present. The factors provoking the disease are osteochondrosis, bending of the spine (in our case, hyperlordosis of the lumbar spine), and metabolic syndromes.
Cases of the Baastrup syndrome in ancient populations, according to the Russian and foreign
*The disease was thoroughly studied and described by Christian Baastrup, a roentgenologist from Copenhagen.
literature on the subject, were rare. A description of spine pathologies in the Middle Paleolithic Neanderthal individual from La Chapelle-aux-Saints (male, 50–60 years old), diagnostic for the syndrome, was published by Haeusler and colleagues (Haeusler et al., 2019). False joints between the spinous processes of С6 and С7, L4, L5, and S1 (first sacral vertebra) were detected. As a probable factor, hyperlordosis of the cervical and lumbar spine was suggested. Three cases of the Baastrup syndrome were observed in the individuals from late medieval burials in France (Kacki, Villotte, Knüsel, 2011). The authors suggest that in those cases the disease was related to trauma, kyphoscoliosis, and metabolic disorders.
Our study of the CT images of the bones has shown serious defects in the internal bone structure of the lumbar vertebrae. The cortical layer is thinned, while the spongy bone displays loci of angiomatosis (i.e. excessive growth of small blood vessels). This picture is different from hemangioma, where some “swelling” of the vertebral body is typical—not present in our case. Most vertebral hemangiomas are associated to some extent to the degenerative and dystrophic processes of the spine, namely with involution of the red bone marrow and osteoporosis (Kravtsov et al., 2015: 2). In our case, many typical features of osteoporosis are present: partial lytic loci of trabecular bone are separated by vertically-oriented sclerotized trabeculae, i.e. “velvet” symptom (Kavalerovskiy et al., 2008); absence of horizontally-oriented trabeculae (Kravtsov et al., 2015: 8). Such vertebral lesions are interpreted as spondylopathies.
Pelvic bones. These are extremely light. The iliac crests of both bones exhibit massive bone overgrowths in the area of the broad abdominal muscles attachments (Fig. 6, 7). The lateral labrums—the enthesa of the external oblique abdominal muscle—are particularly enlarged. The sacrum and the left innominate are fused at the sacroiliac joint (Fig. 7). It is unclear if this fusion is a case of true ankylosis or a result of ossification of the chondral layer covering the auricular surfaces of the sacrum and iliac bone in the area of the synovial joint*? The cavity of the synovial part is clearly visible in the CT images (Fig. 8, a ), as well the ossified interosseous sacroiliac ligament in the upper part of

Fig. 7. Ankylosis of the upper part of the left sacroiliac joint and hyperostosis of the iliac crest.
Fig. 6. Right pelvic bone with hyperostosis at the iliac crest and anterior superior spine (indicated with arrows).
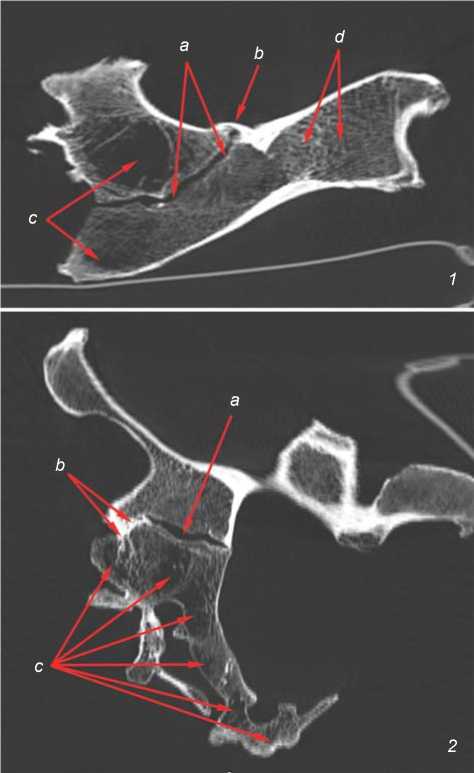
the articular surface (Fig. 8, b ), which forms the fusion of the bones. The pelvic auricular surfaces are clearly outlined by ossified connective tissue structures: joint capsule and ventral sacroiliac ligament. A large area of lysed trabecular bone tissue of the lateral parts of the sacrum—classic marker of osteoporosis—is also visible in the CT images (Fig. 8, c ). The pelvic bones display some manifestations of osteoporosis as well: areas of lysed bone intervening with sclerotized trabeculae-“honeycombs” (Fig. 8, d ) (Ibid.: 5).
Appendicular skeleton
Ankylosis formed as a result of synchondrosis between the sternum and first left rib is observed; no fusion between the sternum and the rib is visible on the right side, though the costal cartilages of both first ribs are ossified. The ossification at the right
Fig. 8. CT images of the pelvic bones.
1 – vertical projection; 2 – sagittal projection.
a – articular cavity of the synovial part of the sacroiliac joint (unaffected); b – ossified sacroiliac ligaments penetrating into the spongy bone; c – large lysed loci inside the cancellous bone of the sacrum and pelvic bones; d – “honeycombs”.
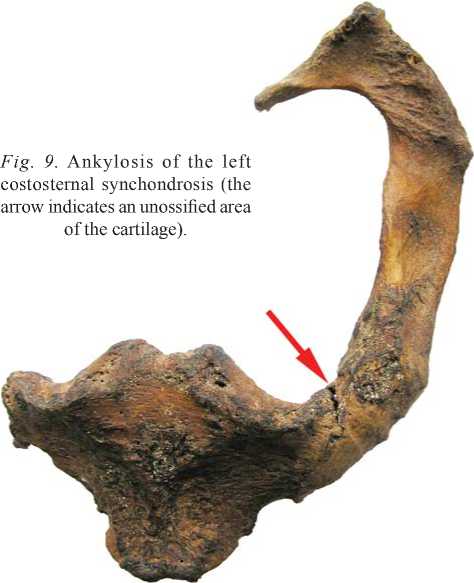
Fig. 9. Ankylosis of the left costosternal synchondrosis (the arrow indicates an unossified area of the cartilage).
system has been described for DISH as compared to the Forestier’s disease (idiopathic fixing spine hyperostosis). It has been long thought that the Forestier’s disease is limited to the ossification of the spine ligaments. But since the middle 1970s, it has become gradually understood that the disease is a generalized pathological process affecting numerous ligaments and tendons of both spine and appendicular skeleton (Resnick, Niwayama, 1976; Mazières, 2013; Mader et al., 2009; Holgate, Steyn, 2016). In the skeleton from Ak-Alakha-1 kurgan 1 burial 1, the main skeletal manifestations of this process were detected. The combination of skeletal lesions typical for DISH has been detected and described in many ancient populations (Buzhilova, 2005: 190–192; Rokhlin, 1965: 191, 195–197; Klaus, Novak, Bavka, 2012; Karapetian, Mkrtchyan, Simonyan, 2019).
The etiology of DISH is not completely understood, but it is known that it is associated with elderly age, metabolic disorders, and associated diseases: hyperuricemia and gout, hyperinsulinemia and type 2 diabetes mellitus, obesity (Pillai, Littlejohn, 2014). Paleopathological studies have detected an association between DISH and social differentiation, which rib was not complete, which is suggested by the presence of a prominent fissure in the internal side of the joint (Fig. 9).
Numerous loci of ossifying enthesopathy are present in the limb bones. These are most pronounced in the distal parts of the limbs, where the pathological process affected not only the structures surrounding the joints but diaphyses as well (Fig. 10). The ossifying hyperostosis and enthesopathy are in some cases accompanied by deforming arthrosis (Figs. 11, 12, 13, 1 ). Hyperostosis and enthesopathies are detected in the acromial and coracoid processes of both clavicles (Fig. 13, 2 ); at several attachment sites: the calcaneus to the Achilles tendon
(Fig. 14, 1 ), quadriceps femoris to patella (Fig. 14, 2 ); triceps brachii tendon to olecranon (Fig. 14, 3 ).
The complex of pathological lesions of the skeletal elements suggests that the individual from Ak-Alakha burial 1 was affected by the diffuse idiopathic skeletal hyperostosis (DISH). A wider array of manifestations in the musculoskeletal indirectly suggests an influence of the lifestyle on its occurrence. The prevalence of DISH in medieval Europe was analyzed based on a large corpus of sources. The markers of the disease are significantly more often detected in the samples from burials of clergy, monks, and benefactors of monasteries, churches, and chapels than from lay burials (Rogers,
Fig. 10. Fibulae.
1 – enthesopathy in the area of the distal tibiofibular syndesmosis; 2 – hyperostosis of the fibular diaphyses . 1


Fig. 11. Proximal tibial epiphyses displaying marked osteoarthritic manifestations in the knee joints (note the large bone defects of the articular surfaces and the subchondral area; ossified remains of the intraarticular structures; massive coarse ostephytes of various shapes surrounding the articular surfaces).

Fig. 12. Ulna and radius.
1 – ossifying enthesopathy of the capsules of the proximal radioulnar joints; 2 – deforming arthritis of the distal epiphyses; numerous eburnated areas at the distal ends of the ulnae; complete loss of the articular disc and the styloid process of the left ulna.

Fig. 13. Right humerus with an ossifying enthesopathy of the articular capsule, massive osteophytes near the tubercles, pronounced narrowing of the intertubercular groove, remnants of an ossified tendon of the long head of the biceps ( 1 ), and the scapulae displaying hyperostosis and numerous massive osteophytes of the acromial and coracoid processes ( 2 ).

Fig. 14. Typical manifestations of the Forestier syndrome: “fringe” osteophytes (indicated with arrows) around the attachment sites of the triceps surae at the calcaneus ( 1 ), quadriceps femoris at the patella ( 2 ), and the triceps brachii at the ulna ( 3 ).


Fig. 15. Clavicles (bottom view).
1 – left clavicle with an improperly healed fracture of the diaphysis and an ossified area of the torn coracoclavicular ligament; 2 – right clavicle (unaffected).
Waldron, 2001; Holgate, Steyn, 2016). An analysis of written sources has shown that the monastic daily ration was richer on animal protein and fat, vegetable oil, as well as wine and ale, and more nutritional in general. This could lead to the development of the disease in the individuals predisposed to it (Rogers, Waldron, 2001).
In the studied skeleton, traumatic pre-mortem lesions were detected as well. The diaphysis of the left clavicle displays a consolidated oblique (spiral?) fracture with a substantial displacement of the bone fragments and shortening of the bone by 2 cm (Fig. 15). It was accompanied by some damage to the coracoclavicular ligament, a part of which got ossified during the process of healing. The possible cause of the fracture was a fall on the shoulder.
A rectangular opening 40 × 7 mm in size was detected in the body of the left clavicle (Fig. 16). It is located near the lateral margin of the bone along the line crossing the scapular notch and its lower angle approximately at the level of the 4th and 5th ribs. The

г 1
Fig. 16. Left scapula displaying a healed fracture.
margins of the lesion are straight and smooth. Possible causes of such defects in the body of the scapula can be pathological processes of an osteolytic character: skeletal metastases, myelomas (Pate et al., 1985: 275), or trauma. The lesions produced by malignant diseases have uneven edges, and other bones of the skeleton are involved in the osteolytic process: the picture we do not observed in the studied skeleton. The trauma of the man’s scapula is accompanied by a fracture of the left clavicle due to a fall on his left shoulder, which resulted in hitting his back against a hard object.
A number of cases of healed fractures of the scapular body have been described in the literature (Blondiaux et al., 2012), and can be employed here as a reference. Blondiaux and colleagues have analyzed bilateral fractures and interpreted those as a result of strong repeating blows to the back given during punishments (Ibid.). An examination of the left ribs revealed the presence of consolidated fractures with a relocation of the fractures in their anterior portions (i.e. along the anterior axillary line), as well as damages to the exterior cortical layers of the 4th and 5th ribs, lateral to the tubercles. The observed combination of lesions in the scapula and ribs suggests that the trauma might have been caused by a blow with a flat-faced pick-axe. The trauma was not fatal, because it did not lead to pneumothorax due to a rupture of lung tissue; thus, the fractures have gradually healed.
Manifestations of a traumatic lesion were detected in the right half of the shoulder girdle as well. The remains of an ossified joint capsule and its outgrowths were found in the articular surface of the head of the right humerus (see Fig. 13, 1 ). The area of the articular surface is substantially decreased and displays numerous Pommer’s nodes along the margin. The upper posterior portion of the surface exhibit an area of eburnation, 25 × 15 mm in size. The surface of the superior part of the greater tubercle is also smooth and partially eburnated. The intertubercle groove is severely narrowed and filled with bone outgrowths and with the remains of a torn off and ossified tendon of the long head of the biceps muscle. These pathological manifestations, together with the trauma of the left bones of the shoulder girdle, were necessarily associated with significant dysfunction of both shoulder joints and severe pain syndrome.
Conclusions
Our study of the male skeleton from the Pazyryk burial at Ak-Alakha has detected numerous pathologic manifestations that cannot be explained by the elderly age of the individual only. Bone tissue changes throughout a person’s life, and loci of bone remodeling are always present in the skeleton. In an adult individual, during a year, approximately 25 % of spongy tissue and 3 % of the compact layer gets substituted by new bone (Avrunin, Tikhilov, Klimov, 2005: 23; Avrunin, Parshin, Abolin, 2006). Any change in the internal structure and shape of bones reflects the adaptation of the skeleton to a specific lifestyle and physical loadings—the main determinant of the bone mass (Riggs, Melton, 2000: 43). Our CT examination has shown a severe disturbance of the internal bone structure of the individual from Ak-Alakha: an almost complete destruction of the cancellous bone of the lumbar vertebrae and pelvic bones, and the development of osteoporosis of the 4th stage. This suggests prolonged inactivity, which might have been a result of the trauma of the shoulder girdle bones, which occurred long before death, and its consequences. Metabolic and endocrine disorders of a genetic nature provoked serious diseases and syndromes, which caused severe sufferings to this undoubtedly strong-willed, courageous, and strong man at the end of his life. These disabilities caused unbearable pain, with some relief coming only in a lying position.
The archaeological context of the burial points towards a high social status of the individual. According to his anthropological features—both craniometric and reconstructed somatological—the origin of this individual was not connected to the aboriginal local populations: a migrant status of his parents can be reasonably assumed. Thus, the individual was not genetically adapted to the conditions of the Altai Mountains. This might be the reason for the large-scale and generalized pattern of the clinic picture of the rheumatologic disease that he suffered, as well as for the extreme severity of the skeletal pathological manifestations.
Acknowledgement
References A case of systemic connective tissue disorder in a Pazyryk male from the Altai Mountains
- Adzhigaytkanova S.K. 2013 Diagnostika i lecheniye otdelnykh form revmaticheskikh zabolevaniy s pozitsii dokazatelnoy meditsiny: Uchebnometod. posobiye. Moscow: Izd. Ros. Nats. Issled. Med. Univ. im. N.I. Pirogova.
- Avrunin A.S., Parshin L.K., Abolin A.B. 2006 Vzaimosvyaz morfofunktsionalnykh izmeneniy na raznykh urovnyakh ierarkhicheskoy organizatsii kortikalnoy kosti pri starenii. Morfologiya, vol. 129 (3): 22–29.
- Avrunin A.S., Tikhilov R.M., Klimov A.V. 2005 Stareniye kostnoy tkani: Teoreticheskoye obosnovaniye novykh putey optimizatsii protsessa mekhanotransduktsii. Morfologiya, vol. 128 (5): 19–28.
- Balueva T.S., Veselovskaya E.V. 2004 New developments in facial reconstruction. Archaeology, Ethnology and Anthropology of Eurasia, No. 1: 143–150.
- Blondiaux J., Fontaine C., Demondion X., Flipo R.-M., Colard T., Mitchell P. D., Buzon M., Walker P. 2012 Bilateral fractures of the scapula: Possible archaeological examples of beatings from Europe, Africa and America. International Journal of Paleopathology, vol. 2 (4): 223–230.
- Buzhilova A.P. 2005 Homo sapiens: Istoriya bolezni. Moscow: Yazyki slavyan. kultury.
- Gerasimov M.M. 1949 Osnovy vosstanovleniya litsa po cherepu. Moscow: Sov. nauka.
- Gerasimov M.M. 1955 Vosstanovleniye litsa po cherepu (sovremenniy I iskopayemiy chelovek). Moscow: Izd. AN SSSR. (TIE. Nov. Ser.; vol. XXVIII).
- Haeusler M., Trinkaus E., Fornai C., Müller J., Bonneau N., Boenia T., Frater N. 2019 Morphology, pathology, and the vertebral posture of the La Chapelle-aux-Saints Neandertal. Proceeding of the National Academy of Sciences, vol. 116 (11): 4923–4927.
- Holgate R.L.V., Steyn M. 2016 Diffuse idiopathic skeletal hyperostosis: Diagnostic, clinical, and paleopathological considerations. Clinical anatomy, vol. 29 (7): 870–877.
- Ivashkin V.T., Sultanov V.K. 2005 Bolezni sustavov: Propedevtika, differentsialniy diagnoz, lecheniye. Moscow: Litterra.
- Kacki S., Villotte S., Knüsel C.J. 2011 Baastrup’s sign (kissing spines): A neglected condition in paleopathology. International Journal of Paleopathology, vol. 1 (2): 104–110.
- Karapetian M., Mkrtchyan R., Simonyan H. 2019 Ankylosing spondylitis: Antiquity and differential diagnosis a case study of a Bronze Age skeleton from Norabak, southeastern Armenia. Homo, vol. 70 (3): 171–183.
- Kavalerovskiy G.M., Chenskiy A.D., Makirov S.K., Cherepanov V.G., Smolyanskiy Y.Z., Lisenkov K.A. 2008 Gemangiomy pozvonochnika: Znacheniye luchevoy diagnostiki. Radiologiya – praktika, No. 1: 23–30.
- Kitov E.P., Mamedov A.M. 2014 Kochevoye naslediye Zapadnogo Kazakhstana v rannem zheleznom veke. Astana: Fil. Inst. Arkheologii im. A.K. Margulana v g. Astana.
- Klaus M., Novak M., Bavka M. 2012 Four cases of ankylosing spondylitis in medieval skeletal series from Croatia. Rheumatology International, vol. 32 (12): 3985–3992.
- Kravtsov M.N., Manukovskiy V.A., Manashchuk V.I., Svistov D.V. 2015 Diagnostika i lecheniye agressivnykh gemangiom pozvonkov: Klinicheckiye rekomendatsii. Moscow: Assotsiatsiya neyrokhirurgov Rossii.
- Lebedinskaya G.V. 1998 Rekonstruktsiya litsa po cherepu (metodicheskoye rukovodstvo). Moscow: Stariy sad. Mader R., Sarzi-Puttini P., Atzeni F., Olivieri I., Pappone N., Verlaan J.-J., Buskila D. 2009 Extraspinal manifestations of diffuse idiopathic skeletal hyperostosis. Rheumatology, vol. 48: 1478–1481.
- Mazières B. 2013 Diffuse idiopathic skeletal hyperostosis (Forestier-Rotes- Queroldisease): What’s new? Joint Bone Spine, vol. 80: 466–470.
- Naseleniye Gornogo Altaya v epokhu rannego zheleznogo veka kak etnokulturniy fenomen: Proiskhozhdeniye, genesis, istoricheskiye sudby (po dannym arkheologii, antropologii, genetiki). 2003 V.I. Molodin, M.I. Voevoda, T.A. Chikisheva, A.G. Romashchenko, N.V. Polosmak, E.O. Shulgina, M.V. Nefedova, I.V. Kulikov, L.D. Damba, M.A. Gubina, V.F. Kobzev. Novosibirsk: Izd. SO RAN.
- Nikitin S.A. 2009 Plasticheskaya rekonstruktsiya portreta po cherepu. In Nekropol russkikh velikikh knyagin i tsarits v Voznesenskom monastyre moskovskogo Kremlya. In 4 vols. Vol. 1: Istoriya usypalnitsy i metodika issledovaniya zakhoroneniy. Moscow: Gos. Ist.-Kult. Muzey-Zapovednik “Moskovskiy Kreml”, pp. 137–167.
- Pate D., Kursunoglu S., Resnick D., Resnik C.S. 1985 Scapular foramina. Skeletal Radiology, vol. 14: 270–275.
- Pilipenko A.S., Trapezov R.O., Polosmak N.V. 2015 A paleogenetic study of Pazyryk people buried at Ak-Alakha-1, the Altai Mountains. Archaeology, Ethnology and Anthropology of Eurasia, vol. 43 (4): 147–153.
- Pillai S., Littlejohn G. 2014 Metabolic factors in diffuse idiopathic skeletal hyperostosis: A review of clinical data. The Open Rheumatology Journal, vol. 8: 116–128.
- Polosmak N.V. 1994 Steregushchiye zoloto grify. Novosibirsk: Nauka.
- Polosmak N.V. 2001 Vsadniki Ukoka. Novosibirsk: INFOLIO-press. Prives M.G., Lysenkov N.K., Bushkovich V.I. 2006 Anatomiya cheloveka. St. Petersburg: Izd. dom Sankt-Peterburg. akademii poslediplom. obrazovaniya.
- Resnick D., Niwayama G. 1976 Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology, vol. 119: 559–568.
- Riggs B.L., Melton III L.J. 2000 Osteoporoz: Etiologiya, diagnostika, lecheniye. Moscow: Binom, St. Petersburg: Nevskiy dialekt.
- Rogers J., Waldron T. 2001 DISH and monastic way of life. International Journal of Osteoarchaeology, vol. 11: 357–365.
- Rokhlin D.G. 1965 Bolezni drevnikh lyudey. Moscow, Leningrad: Nauka.
- Rudenko S.I. 1953 Kultura naseleniya Gornogo Altaya v skifskoye vremya. Moscow, Leningrad: Izd. AN SSSR.
- Skryabina E.N., Magdeeva N.A., Korneeva Y.M. 2020 Ankiloziruyushchiy giperostoz pozvonochnika ili bolezn Forestye: Trudnosti diagnostiki ili nedostatochnaya osvedomlennost? Arkhiv vnutrenney meditsiny, vol. 10 (1): 68–73.
- Starkova A.S., Erdes S.F. 2016 Slozhnosti v diagnostike idiopaticheskogo giperostoza skeleta (bolezni Forestye). Nauchno-prakticheskaya revmatologiya, vol. 54 (1): 80–82.
- Turdialieva S.A., Mozharovskaya E.A., Kudrina O.M., Cherkashin D.V. 2015 Naiboleye chasto vstrechayushchiyesya zabolevaniya sustavov: Aktualniye voprosy diagnostiki i lecheniya. Vestnik Rossiyskoy voyenno-meditsinskoy akademii, No. 3 (51): 227–233.
- Veselovskaya E.V. 2015 Kraniofatsialniye proportsii v antropologicheskoy rekonstruktii. Etnograficheskoye obozreniye, No. 2: 83–98.
- Zharkov P.L. 1994 Osteokhondroz i drugiye distroficheskiye izmeneniya pozvonochnika u vzroslykh i detey. Moscow: Meditsina.
