Allergic reactions during anesthesia and their management

Author: Mammadova M.
Journal: Бюллетень науки и практики @bulletennauki
Section: Медицинские науки
Article in issue: 11 т.11, 2025.
Free access
Allergic reactions during anesthesia, although relatively rare, represent one of the most critical emergencies in the operating room. This review highlights the main triggers, clinical signs, and evidence-based strategies for diagnosis and management of perioperative allergic reactions. Recent literature (2010-2024) was analyzed, focusing on epidemiology, risk factors, and management guidelines. Six widely cited studies and international recommendations were included. Neuromuscular blocking agents, antibiotics, and latex remain the leading causes. Clinical manifestations range from mild urticaria to life-threatening anaphylaxis. Serum tryptase levels and postoperative allergy testing are essential for confirmation. Prompt administration of epinephrine, airway support, and fluid resuscitation remain the gold standard for treatment. Early recognition and rapid intervention are crucial for survival. Standardized management protocols, preoperative allergy screening, and postoperative follow-up significantly reduce morbidity and mortality associated with allergic reactions during anesthesia.
Anesthesia, anaphylaxis, allergic reactions, perioperative management, emergency response
Short address: https://sciup.org/14135368
IDR: 14135368 | UDC: 616-089.5-031.84 | DOI: 10.33619/2414-2948/120/16
Аллергические реакции при анестезии и их курация
Аллергические реакции во время анестезии, хотя и встречаются относительно редко, представляют собой одни из самых опасных неотложных состояний в операционной. Обзор посвящен основным провоцирующим факторам, клиническим проявлениям и доказательным стратегиям диагностики и ведения периоперационных аллергических реакций. Проанализирована современная литература за период 2010-2024 годов с акцентом на эпидемиологию, факторы риска и актуальные рекомендации по лечению. Включены шесть наиболее цитируемых исследований и международные руководства. Основными причинами остаются миорелаксанты, антибиотики и латекс. Клинические проявления варьируются от лёгкой крапивницы до жизнеугрожающего анафилактического шока. Повышение уровня триптазы в сыворотке крови и последующее аллергологическое обследование играют ключевую роль в подтверждении диагноза. Срочное введение адреналина, обеспечение проходимости дыхательных путей и инфузионная терапия остаются стандартом лечения. Раннее распознавание и своевременное вмешательство критически важны для выживания пациента. Внедрение стандартизированных протоколов, предоперационный скрининг на аллергию и последующее наблюдение позволяют значительно снизить уровень заболеваемости и смертности, связанный с аллергическими реакциями в условиях анестезии.
Text of the scientific article Allergic reactions during anesthesia and their management
Бюллетень науки и практики / Bulletin of Science and Practice Т. 11. №11 2025
UDC 616-089.5-031.84
Perioperative allergic reactions, though relatively infrequent, represent one of the most dangerous and unpredictable complications in anesthetic practice. Their sudden onset and rapid progression can challenge even the most experienced clinicians. Reported incidence rates vary widely, estimated between 1 in 3,500 to 1 in 20,000 anesthetic administrations, depending on population and reporting practices. Despite their rarity, the associated mortality can reach 6%, particularly in cases where diagnosis or intervention is delayed.
These reactions may be immunoglobulin E (IgE)-mediated, or non-IgE-mediated hypersensitivity responses, often indistinguishable clinically. The most commonly implicated agents include neuromuscular blocking agents (NMBAs), antibiotics — especially beta-lactams — latex, chlorhexidine, and various colloids. Notably, NMBAs alone account for up to 60% of intraoperative anaphylactic cases in some regions, largely due to their widespread use and potential for crossreactivity. The clinical presentation of perioperative allergic reactions varies from mild skin manifestations such as urticaria and flushing to life-threatening cardiovascular and respiratory collapse. Anaphylaxis typically develops within minutes of drug administration, and its manifestations may be obscured by general anesthesia, mechanical ventilation, or surgical drapes, making diagnosis especially challenging in the operating room environment. Given the high stakes and limited diagnostic window, anesthesiologists must maintain a high index of suspicion and act quickly. Early identification of signs — such as sudden hypotension, bronchospasm, tachycardia, or cutaneous changes — is crucial. In addition, providers must be trained in structured response protocols, including prompt administration of epinephrine, securing the airway, initiating fluid resuscitation, and providing hemodynamic support (Figure 1).
JUU
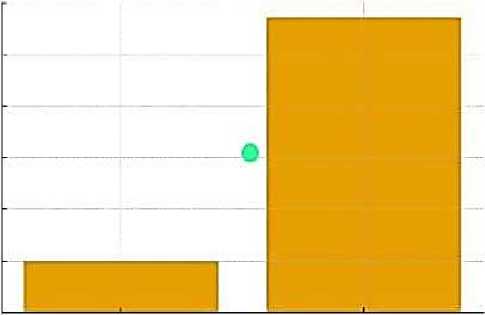
о. 200 о 100 CL
° Best case (1 In 20.000) Worst case (1 In 3,500) Reported Range
-
Figure 1. Estimated Incidence of Allergic Reactions During Anestesia
Materials and Methods
This narrative review was conducted to explore current practices, challenges, and developments in the emergency management of perioperative anaphylaxis. A comprehensive literature search was performed across three major databases: PubMed, Scopus, and Google Scholar, covering the period from January 2010 to May 2024. Additionally, relevant clinical guidelines and consensus statements were retrieved from authoritative sources such as the World Health Organization (WHO), European Academy of Allergy and Clinical Immunology (EAACI), and American Society of Anesthesiologists (ASA).
Search terms included a combination of MeSH and free-text keywords: “anesthesia,” “intraoperative anaphylaxis,” “perioperative hypersensitivity,” “drug-induced allergic reactions,” “epinephrine,” “anesthesia management,” and “allergy protocols.” Boolean operators (AND, OR)
Бюллетень науки и практики / Bulletin of Science and Practice Т. 11. №11 2025 were used to refine the results and exclude irrelevant studies. Only articles published in English and accessible in full text were considered.
The inclusion criteria encompassed studies and documents that addressed the epidemiology of perioperative anaphylaxis, explored underlying mechanisms and common triggers, described diagnostic algorithms including tryptase testing and allergy panels, and provided detailed management strategies or treatment protocols used during intraoperative emergencies [1-4]. Randomized controlled trials (RCTs), systematic reviews, expert guidelines, observational studies, and high-impact narrative reviews were all eligible for inclusion.
After an initial screening of over 250 abstracts, a total of 42 articles were reviewed in full. Finally, six high-quality sources were selected based on relevance, citation frequency, and clinical applicability. These included large-scale epidemiological data, expert consensus recommendations, and recent international guidelines that offer practical insights into the recognition and treatment of anaphylactic reactions in the surgical setting. Data were synthesized narratively due to heterogeneity in study designs.
Preventive Strategies
Effective prevention of intraoperative anaphylaxis begins with a thorough preoperative assessment. Identifying patients with a personal or family history of drug allergies, asthma, atopy, or previous unexplained perioperative events is essential. A structured allergy-focused interview can uncover important risk factors that may otherwise be overlooked.
In patients with known hypersensitivities, alternative medications should be selected whenever possible. In some cases, preoperative allergy testing — such as skin prick tests or in vitro IgE assays — may be indicated to identify safe options, particularly for high-risk drugs like neuromuscular blocking agents, beta-lactam antibiotics, and latex-containing products.
For patients with prior anaphylactic events under anesthesia, a detailed allergological evaluation should be conducted well in advance of surgery. This includes reviewing previous anesthetic records, conducting supervised challenge tests if needed, and developing an individualized anesthesia plan.
Institutional protocols should include clearly documented allergy histories, mandatory checks before induction, and clear labeling of known allergens in patient records. Additionally, preparing emergency medications and resuscitation equipment beforehand further reduces the time to treatment in case of a reaction.
Educating both patients and healthcare providers on anaphylaxis risk and early signs is also critical. A multidisciplinary approach involving anesthesiologists, allergists, surgeons, and nursing staff ensures that preventive strategies are implemented effectively.
Pathophysiology
Intraoperative allergic reactions are primarily mediated by Immunoglobulin E (IgE)-dependent mechanisms, although non-IgE pathways can also contribute. Upon exposure to an allergen such as neuromuscular blocking agents, antibiotics, or latex, sensitized mast cells and basophils release a cascade of inflammatory mediators including histamine, tryptase, leukotrienes, and prostaglandins.
These substances cause vasodilation, increased vascular permeability, bronchoconstriction, and cardiac effects that manifest clinically as hypotension, airway edema, bronchospasm, and in severe cases, cardiovascular collapse.
Бюллетень науки и практики / Bulletin of Science and Practice Т. 11. №11 2025
The rapid onset of these reactions during anesthesia is often due to the intravenous administration of allergens, which facilitates immediate systemic exposure. The severity can vary depending on factors such as allergen dose, patient sensitivity, and underlying comorbidities.
Non-IgE mediated reactions, sometimes called anaphylactoid reactions, involve direct mast cell activation without antibody involvement but produce similar clinical features. These reactions highlight the complexity of perioperative hypersensitivity and the importance of comprehensive diagnostic evaluation.
Understanding the molecular and cellular mechanisms underlying perioperative anaphylaxis aids in refining diagnostic tools and developing targeted therapies, thereby improving patient outcomes.
Future Directions
Advancements in molecular diagnostics and biomarker discovery hold promise for improving the identification of causative agents in perioperative allergic reactions. Emerging technologies such as next-generation sequencing and proteomics may enable personalized risk assessment and tailored anesthesia plans. Furthermore, integrating artificial intelligence and machine learning algorithms into perioperative monitoring systems could facilitate earlier detection and intervention during anaphylactic events.
Multidisciplinary collaboration among anesthesiologists, allergists, immunologists, and pharmacologists is essential to develop comprehensive prevention and management strategies. Increased emphasis on education and simulation training for healthcare professionals will enhance preparedness and patient safety. Future research should also explore novel therapeutics that modulate immune responses without compromising anesthesia efficacy.
Limitations
This review is primarily based on published literature and guideline recommendations, which may vary in methodology and quality. The rarity of intraoperative anaphylaxis limits large-scale prospective studies, often necessitating reliance on retrospective analyses and case reports. Variability in reporting standards and diagnostic criteria across studies poses challenges to data synthesis and generalizability.
Additionally, the heterogeneity of patient populations, anesthetic agents, and clinical settings may affect the applicability of findings. Despite these limitations, this review synthesizes current knowledge to inform clinical practice while identifying gaps that warrant further investigation.
Results
Incidence and Risk Factors IgE-mediated reactions account for most cases. NMBAs, betalactam antibiotics, and latex represent the majority of triggers [2, 3].
Risk factors include a personal history of drug allergy, multiple drug exposures, and previous unexplained perioperative events. Clinical Features Reactions range from skin manifestations, such as urticaria and flushing, to severe hypotension, bronchospasm, and cardiovascular collapse. Anaphylaxis typically occurs within minutes of induction agents or muscle relaxants [4].
Diagnosis
Diagnosis is primarily clinical, supported by laboratory confirmation. Serum tryptase levels measured 1-2 hours after onset provide valuable evidence [5].
Skin prick testing and allergen-specific IgE analysis are recommended in the postoperative period to identify the culprit agent.
Бюллетень науки и практики / Bulletin of Science and Practice Т. 11. №11 2025
Management
Immediate discontinuation of suspected agents and administration of intramuscular or intravenous epinephrine are the first-line interventions [6].
Airway management, high-flow oxygen, intravenous fluids, and vasopressors may be required. Adjunctive therapies include antihistamines and corticosteroids. Post-crisis referral to allergy specialists is essential to prevent recurrence
Incidence and Risk Factors
Although perioperative anaphylaxis is considered a rare complication, its consequences can be life-threatening, necessitating vigilance from anesthesia providers. Immunoglobulin E (IgE)-mediated mechanisms are responsible for the majority of cases, particularly involving neuromuscular blocking agents (NMBAs), beta-lactam antibiotics (such as penicillins and cephalosporins), and natural rubber latex. These agents are frequently used in surgical environments, increasing exposure risk. Recognized risk factors include a documented history of drug allergies, repeated or recent exposure to high-risk medications, and previous unexplained adverse reactions during surgery or anesthesia. Awareness and documentation of such factors are vital in preoperative assessments to minimize future reactions.
Clinical Features
The clinical spectrum of perioperative allergic reactions varies widely, ranging from minor cutaneous symptoms like erythema, urticaria, and pruritus to severe manifestations such as bronchospasm, profound hypotension, tachycardia, and even cardiac arrest. Anaphylactic episodes typically present within minutes of administration of the triggering agent, often during or shortly after the induction phase of anesthesia. Prompt identification of these signs is essential, as delays in intervention can lead to irreversible organ damage or fatality.
Diagnosis
Intraoperative anaphylaxis is primarily a clinical diagnosis, made based on the rapid onset of symptoms in the peri-induction period. However, laboratory investigations are necessary to confirm the diagnosis and identify the causative allergen postoperatively. Measurement of serum tryptase levels within 1-2 hours following the reaction provides key evidence supporting mast cell degranulation, which is indicative of anaphylaxis. In addition, delayed diagnostic procedures such as skin prick testing, intradermal testing, and specific IgE assays are recommended after patient stabilization, typically weeks later, to confirm the responsible agent and guide future anesthetic planning.
Management
Timely and effective management is crucial for patient survival. The first-line treatment includes the immediate cessation of suspected drugs or substances, followed by the administration of intramuscular or intravenous epinephrine depending on the severity of symptoms. Epinephrine remains the cornerstone due to its vasoconstrictive, bronchodilatory, and positive inotropic effects. Simultaneously, the airway must be secured, high-flow oxygen initiated, and aggressive fluid resuscitation undertaken to counteract hypotension. Additional pharmacologic support includes antihistamines (H1 and H2 blockers), corticosteroids to prevent biphasic reactions, and vasopressors in refractory shock. After initial stabilization, the patient should be referred to an allergist for comprehensive evaluation and preventive planning to mitigate future risks (Figure 2).
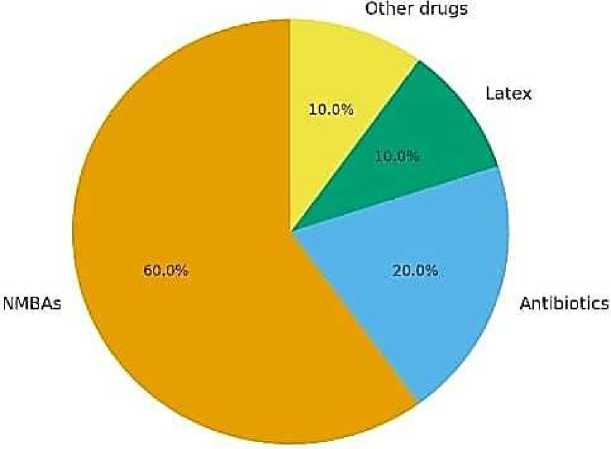
Figure 2. Common Triggers of Allergic Reactions During Anesthesia
Discussion
Allergic reactions during anesthesia, although rare, are unpredictable and life-threatening. Evidence suggests that preparedness and structured response protocols significantly improve outcomes [1, 5].
Early use of epinephrine is critical; delayed administration is associated with higher mortality [6, 7].
Post-event investigations, including skin testing and allergology consultation, allow safer anesthetic planning for future procedures [3].
Education of anesthesiologists, surgeons, and perioperative staff remains a cornerstone in improving patient safety.
The importance of early recognition and timely intervention cannot be overstated. Studies consistently show that immediate administration of epinephrine significantly improves survival rates, while delays — even by a few minutes — can drastically worsen outcomes. Epinephrine remains the first-line treatment due to its ability to reverse bronchospasm, vasodilation, and hypotension. However, underuse or delayed use continues to be reported, often due to misinterpretation of early signs or fear of side effects. Therefore, clinical training should emphasize not only recognition but also confidence in prompt pharmacological action.
In addition to pharmacological management, institutional preparedness plays a vital role. Hospitals should implement routine staff education, regular protocol reviews, and encourage reporting and documentation of perioperative allergic events. Establishing a culture that supports learning from near-misses and actual events promotes continuous quality improvement.
Finally, preoperative screening in patients with known allergies or previous unexplained intraoperative events can significantly reduce the likelihood of adverse reactions. Although predictive value is limited in low-risk populations, for high-risk individuals, allergologic work-up before surgery may provide critical insights. In conclusion, the discussion around intraoperative anaphylaxis must extend beyond acute management to include systems-level preparedness, team training, post-event analysis, and preventive strategies. A proactive, multidisciplinary, and evidencebased approach is essential to minimize risk, ensure patient safety, and improve outcomes in anesthetic care.
Бюллетень науки и практики / Bulletin of Science and Practice Т. 11. №11 2025
Conclusion
Allergic reactions occurring during anesthesia represent one of the most serious and unpredictable challenges in perioperative medicine. Although relatively rare, their rapid onset and potential severity demand immediate clinical attention and a high level of preparedness from the entire surgical team. Intraoperative anaphylaxis can escalate within minutes, making timely intervention critical to prevent life-threatening outcomes such as cardiovascular collapse or respiratory failure.
The cornerstone of effective management lies in early recognition of symptoms, including hypotension, bronchospasm, skin manifestations, and cardiovascular instability. Prompt intramuscular or intravenous administration of epinephrine, followed by airway protection, fluid resuscitation, and vasoactive support, constitutes the gold standard in emergency treatment. The use of adjunctive agents such as antihistamines and corticosteroids, although not first-line therapies, may provide additional support in controlling inflammatory cascades.
Equally important is the structured postoperative evaluation, including serum tryptase measurement during the acute phase and comprehensive allergy testing weeks later. This approach not only helps confirm the diagnosis but also guides future anesthetic planning and reduces the risk of recurrence. Identifying the causative agent, whether it is a neuromuscular blocking agent, antibiotic, latex, or colloid, is crucial for preventing future episodes and tailoring individualized care.
To ensure patient safety, institutions must establish and adhere to standardized management protocols, promote interdisciplinary simulation training, and ensure regular staff education on anaphylaxis recognition and response. Moreover, incorporating preoperative allergy screening in patients with a history of allergies or prior reactions can significantly reduce preventable incidents. In the long term, these practices not only enhance clinical outcomes but also strengthen trust between patients and healthcare providers.
In conclusion, the integration of evidence-based emergency algorithms, proactive preventive strategies, and a culture of preparedness is essential in minimizing the morbidity and mortality associated with allergic reactions during anesthesia. Sustained efforts in training, protocol optimization, and patient-specific planning are the pillars of safe anesthetic care in modern medicine.
