Clinical Presentation of Febrile Illness and its Overlap with Infectious Mononucleosis among Young Adults

Author: Mamatkulova N., Martin Abhinaya, Pudupalli Sana Hussain, Suresh Sooraj
Journal: Бюллетень науки и практики @bulletennauki
Section: Медицинские науки
Article in issue: 2 т.12, 2026.
Free access
Young adults experience febrile illnesses (fever) with throat discomfort and exhaustion. Many infections that cause febrile illnesses in young adults also cause symptoms that coincide with bacterial throat infections (pharyngitis/endemic febrile illnesses in India), resulting in many cases of infectious mononucleosis being underdiagnosed. To fully explore how young adults present clinically with fevers and throat symptoms, this project aims to determine the specific clinical presentation, the diagnostic approach taken by doctors, as well as any potential misdiagnosis of infectious mononucleosis among young adults who have had febrile illnesses with throat symptoms. Using a cross-sectional survey, we collected information from 120 young adults (ages 18-30) who had experienced febrile illnesses within the last 6 months. The survey was conducted using anonymous questionnaire items that provided information about symptoms, duration of symptoms, swollen lymph nodes, fatigue, blood tests/investigations completed by the respondents, treatments, and recovery time. All survey response data and results were compiled using descriptive statistics. Fever (90.8%), sore throat (76.7%), fatigue (76%), and neck/lymph node swelling (60%) were the most reported symptoms. The presence of prolonged (longer than 2 weeks) fatigue and lethargy was reported by 40% of the respondents. Thirty percent of respondents had blood tests completed, and 5% completed heterophile/EBV tests. Antibiotics were given in 70% of the cases, and 20% of the respondents experienced a rash following antibiotic administration. Recovery from febrile illnesses took 1 to 2 weeks for 50% of respondents to return to their normal level of activity. Young adults with a febrile illness frequently report prolonged fever, sore throat, lymphadenopathy, and fatigue; understanding these symptoms can aid in the early diagnosis of conditions like infectious mononucleosis (IM) and help avoid misdiagnosis and inappropriate antibiotic use.
Infection, antibiotics, virus, treatment
Short address: https://sciup.org/14134450
IDR: 14134450 | UDC: 616.9-053.2-06:616.24-008.6 | DOI: 10.33619/2414-2948/123/38
Клиническая картина лихорадочного состояния и его совпадение с инфекционным мононуклеозом у молодых людей
У молодых людей часто встречаются лихорадочные заболевания (повышенная температура) с дискомфортом в горле и истощением. Многие инфекции, вызывающие лихорадочные заболевания у молодых людей, также вызывают симптомы, совпадающие с бактериальными инфекциями горла (фарингит/эндемичные лихорадочные заболевания в Индии), что приводит к тому, что многие случаи инфекционного мононуклеоза остаются недиагностированными. Для полного изучения клинических проявлений лихорадки и симптомов со стороны горла у молодых людей, данный проект направлен на определение специфической клинической картины, диагностического подхода (врача), а также любых потенциальных случаев ошибочной диагностики инфекционного мононуклеоза среди молодых людей, перенесших лихорадочные заболевания с симптомами со стороны горла. С помощью поперечного исследования собрали информацию от 120 молодых людей (в возрасте 18-30 лет), перенесших лихорадочные заболевания в течение последних 6 месяцев. Опрос проводился с использованием анонимных анкет, содержащих информацию о симптомах, продолжительности симптомов, увеличенных лимфатических узлах, усталости, проведенных анализах крови/исследованиях, лечении и времени выздоровления. Все данные и результаты опроса были обработаны с использованием описательной статистики. Наиболее часто сообщаемыми симптомами были лихорадка (90,8%), боль в горле (76,7%), усталость (76%) и увеличение лимфатических узлов шеи (60%). Длительная (более 2 недель) усталость и вялость отмечались у 40% респондентов. Тридцать процентов респондентов сдали анализы крови, а пять процентов — тесты на гетерофильные вирусы/вирус Эпштейна-Барр. Антибиотики назначались в 70% случаев, и у 20% респондентов после приема антибиотиков появилась сыпь. Восстановление после лихорадочных заболеваний занимало от 1 до 2 недель у 50% респондентов, которые возвращались к своей обычной активности. Молодые люди с лихорадочными заболеваниями часто сообщают о длительной лихорадке, боли в горле, лимфаденопатии и усталости; понимание этих симптомов может помочь в ранней диагностике таких заболеваний, как инфекционный мононуклеоз (ИМ), и помочь избежать неправильной диагностики и ненадлежащего использования антибиотиков.
Text of the scientific article Clinical Presentation of Febrile Illness and its Overlap with Infectious Mononucleosis among Young Adults
Бюллетень науки и практики / Bulletin of Science and Practice
When adolescents and young adults visit the medical office complaining of fever and throat-related symptoms, the most commonly diagnosed cause is a viral upper respiratory tract infection, or acute pharyngitis. While most of these conditions are self-limiting, it is important for clinicians to identify and differentiate these cases from each other to prevent misdiagnosis and unnecessary treatment [1].
One of the leading causes of prolonged febrile illness in young adults is infectious mononucleosis (IM). IM is generally due to an individual's first exposure to the Epstein-Barr virus (EBV). EBV is a member of the herpes virus family and can be transmitted through saliva or intimate personal contact [2].
EBV infections occur globally, but the way people exhibit symptoms of their initial infection varies according to age. Younger individuals (children) experience milder or no symptoms during their initial infection, whilst older adolescents and young adults typically experience the typical symptoms associated with IM (fatigue, fever, sore throat, lymphadenopathy, headache, and splenomegaly) and are generally considered highly contagious [3].
Diagnosing febrile illnesses accompanied by throat symptoms presents many difficulties due to the very high number of diseases caused by germs (infectious diseases) and overlapping signs and symptoms. Commonly included in the list of differential diagnoses are bacterial tonsillitis, dengue fever, malaria, typhoid fever, and tuberculosis [4].
Consequently, many young adults diagnosed with infectious mononucleosis (IM) incorrectly receive and are treated with antibiotics (generally β-lactam antibiotics, e.g., amoxicillin or ampicillin). These treatments do not improve their clinical state but rather produce potentially lifethreatening adverse drug reactions, particularly a maculopapular rash [5].
Understanding the clinical presentation pattern and duration of symptoms, treatment practices, and timelines of recovery in young adults is crucial to the early identification of IM, as well as distinguishing IM from other causes of febrile illness. Community-based, symptom-oriented surveys represent the most practical and cost-effective way to gather information about how these conditions present themselves, particularly when laboratory tests are not available or feasible. Using disease-blinded, neutral questionnaires will help reduce bias in the results and provide a more thorough understanding of the various symptom presentation patterns [6, 7].
To assess the clinical characteristics, time of symptom occurrence, treatment strategies, and outcomes from febrile illness with throat symptoms comparable to those presented in the Indian young adult population within the past year, this research was created to provide insight into these trends so that health professionals can recognize symptoms that may be indicative of infectious mononucleosis and, therefore, will be more likely to include infectious mononucleosis as one of the differential diagnoses when evaluating patients for febrile illness with any upper respiratory tract signs. As a result, less misdiagnosis will occur and unnecessary antibiotic usage will be minimized [8].
Methods
A cross-sectional survey was conducted among medical students enrolled in the International Medical Faculty and their friends in India online. One hundred and twenty young adults aged 18-30 who had experienced a fever or throat-related illness in the last 6 months and were willing to participate in the study were included. Participants with known immunosuppression, chronic liver disease, or hematologic malignancy, or who had completed less than 50% of the questionnaire were excluded. An anonymous survey consisting of 15 questions was created to obtain the following data about patients with infectious mononucleosis (IM), including those diagnosed with IM based on clinical diagnosis:
-
1. Demographics (Age/Gender).
-
2. Fever History (Duration/Severity).
-
3. Sore Throat/Tonsillar Symptoms.
-
4. Fatigue and Duration.
-
5. Swollen lymph nodes.
-
6. Abdominal Pain (Possible Splenomegaly).
-
7. Laboratory results (CBC, liver function testing, Heterophile/EBV).
-
8. Treatment Received (Antibiotics/Supportive care).
-
9. Adverse events after treatment (Antibiotic rash).
-
10. Time to recover from illness.
-
11. The survey was designed to remain unbiased by not mentioning IM or EBV, so that participants would provide truthful answers.
-
12. Respondents participated voluntarily, and responses were confidential.
-
13. Electronic consent to participate was obtained.
-
14. Secure data storage was implemented for the purposes of academic research.
Descriptive statistics were used to create tables of responses. Frequencies and percentages were determined for categorical data, and patterns of symptoms, antibiotic usage, and duration of recovery were examined. Potential cases of IM were defined as individuals with fever lasting longer than 7 days, sore throat, neck/lymph node swelling, and fatigue lasting longer than 2 weeks.
Results
The majority of respondents were between the ages of 21 and 25 years, at 76.7%, while those in the age group of 18–20 years represented 15% and 25–30 years represented 8.3%. Of the respondents to this survey, females represented 63.3% of the total population, whereas males represented 35.8%. A small percentage of participants declined to indicate their gender. Therefore, it can be inferred that young adults and female respondents were strongly represented in this study.
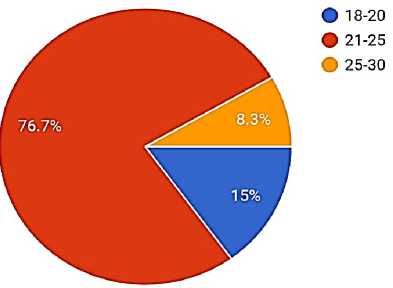
Age distribution
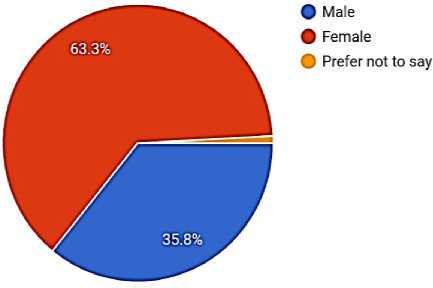
Gender Distribution
Duration of Febrile Illness
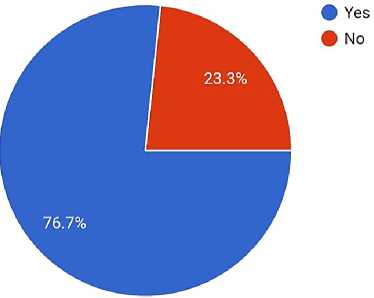
This study confirmed that approximately 90.8% of the individuals studied reported experiencing fever at least once over the previous six months, whereas only 9.2% denied any episodes of fever during this time. This shows that the prevalence of febrile illness in this population is quite high.
Of those who reported experiencing fever, most (60%) said that they had experienced an episode of fever of either acute or short duration, occurring less than 7 days after onset. An additional 34.2% had febrile episodes that persisted for 7 to 14 days, indicating that a significant portion of febrile illnesses were moderate in duration. Only 5.8% reported having experienced a febrile illness lasting over 14 days. These data indicate that febrile illnesses were generally acute in nature and of short duration.
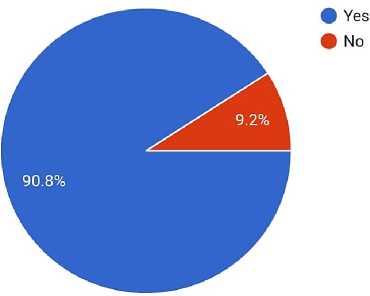
Fever Experienced
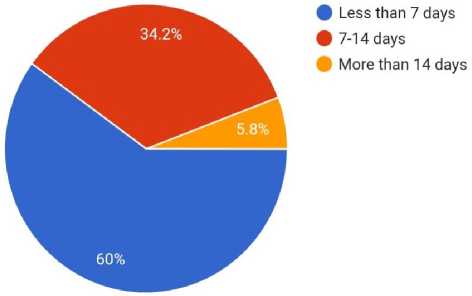
Duration
A notable number of participants also reported having upper respiratory symptoms associated with fever, including sore throat or pain when swallowing, which indicates that infections were likely common in this population. In summary, this study found a high rate of reported febrile illness among young adults, most of which were either acute and lasted for less than seven days or moderate in duration and lasted for seven to 14 days. The majority of respondents with febrile illness indicated that, in addition to fever, sore throat or pain when swallowing was the most frequently noted symptom. Fatigue and generalized weakness were also very common among respondents with febrile illness, and a large percentage experienced symptoms that extended beyond the acute febrile period.
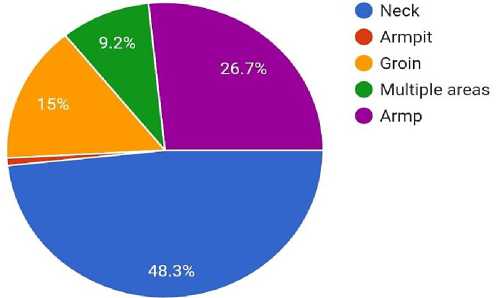
A significant number of respondents reported swelling of lymph nodes in the neck area, while a smaller number described abdominal discomfort or fullness, which may indicate splenic involvement. As shown by the symptom profiles, febrile illnesses in these respondents were mainly associated with upper respiratory tract symptoms, along with systemic features including throat-related symptoms and prolonged fatigue.
Symptom Sore throat and pain
White Patches On Tonsil
Swelling or Pain Presented
TREATMENT PATTERNS
|
Treatment |
Percentage |
|
Antibiotic prescribed |
70 |
|
Supportive care only |
30 |
Discussion
This study looked at how often and what types of febrile illnesses were found in young adults (ages 18–25). Although the study did include classical signs of IM (e.g., prolonged fever, significant lymphadenopathy, and prolonged fatigue), only 0.1% of the participants met all the clinical or laboratory criteria for IM. Therefore, this implies that while febrile illnesses are prevalent in young adults, IM caused by EBV is unlikely to be the primary cause of these febrile illnesses, and that most of these illnesses are likely due to self-limiting viral URIs.
The high rate of short-term fever and sore throat found in the present study supports the premise that viral pharyngitis is likely the most common cause of these febrile illnesses. In addition, most participants reported that their fever had been less than two weeks in duration and, therefore, did not support the diagnosis of IM or any other systemic infection as the source of their fever. However, in some individuals, they experienced fever lasting longer than 2 weeks, and lymphadenopathy, which are classical features of IM. Furthermore, the absence of laboratory tests that could be used to confirm cases of IM, such as a heterophile antibody test or EBV serology, limited the ability of the current study to identify definitive cases of IM.
These results indicate that using symptoms alone to distinguish between IM and other febrile illnesses will lead to diagnostic confusion in a significant proportion of young adults, since there are significant overlaps in the clinical presentation of IM and other febrile illnesses. Therefore, it is important to conduct targeted laboratory tests when evaluating febrile illnesses in young adults.
Conclusion
The data demonstrates that febrile illnesses appear to be quite prevalent at younger ages, with the majority of febrile illness episodes having been rated as either acute or moderate (transient in nature) in duration, and typically accompanied by mild upper respiratory symptoms, with sore throats prominently observed.
While evaluating typical symptoms associated with infectious mononucleosis, only 12 patients were definitively identified as having infectious mononucleosis based on what was evaluated during the study period. This indicates that it is difficult to confirm the diagnosis of herpesvirus disease without diagnostic laboratory studies; therefore, a comprehensive clinical evaluation should be performed, and laboratory testing should be used judiciously, particularly for prolonged fever and persistent significant systemic symptoms.
Overall, utilizing community surveys based on symptom surveys provides a useful method of understanding how febrile illness patterns among younger adults differ from the distinctions between what are benign or “self-limiting” and those which require additional evaluation, and as such, reduces unnecessary therapy while providing better quality patient care.
