Cranial injuries in the late Bronze and early iron age population of the Shnogh river basin, Armenia

Author: Khudaverdyan A.Y., Hobosyan S.G.
Journal: Archaeology, Ethnology & Anthropology of Eurasia @journal-aeae-en
Section: Ethnography
Article in issue: 2 т.45, 2017.
Free access
Short address: https://sciup.org/145145306
IDR: 145145306 | DOI: 10.17746/1563-0110.2017.45.2.149-157
Text of the review article Cranial injuries in the late Bronze and early iron age population of the Shnogh river basin, Armenia
Analysis of characteristic lesions of the skull and postcranial skeleton can provide indirect evidence about social relationships in ancient societies (Rokhlin, 1965: 62–63; Buzhilova, 1995: 100; Khudaverdyan, 2005: 59–64; 2014b; Dobrovolskaya, 2009; Ortner, Putchar, 1981: 72–85). The patterns and localities of fractures are indicative of the social circumstances related to the emergence of particular types of traumas. Therefore, skeletal samples are an independent source of data for historical reconstructions made during complex archaeological research.
In the second half of the 2nd millennium BC, an irrigation system already existed in Armenia; and both viticulture and horticulture were widespread. The development of weaponry (from the dagger to the long bronze and iron swords and other types of armor) points to violent conflicts for territory and booty between different tribes (Martirosyan, 1964: 83–84; 130, 194– 198; Areshyan, 1974). Studying skeletal samples for evidence of trauma is thus necessary to confirm the participation of a particular individual or group in military conflicts.
In this study, we describe the skeletal lesions we have detected in the burials of the 13th–11th centuries BC from the Shnogh River basin (Lori Region, Armenia).
Materials and methods
This study employs skeletal samples from the cemeteries of Bover ( n = 40), Bageri Chala ( n = 32), Bartsryal ( n = 40), Karakotuk ( n = 6), and Tekhut ( n = 6) that were obtained in 2006–2014 during excavations by the Institute of Archaeology and Ethnography of the National Academy of Sciences of the Republic of
Armenia, led by S.G. Hobosyan*. The examination of the 124 skulls (59 male, 26 female, and 39 of unidentified sex) has shown that lesions are typical of both adults and subadults of this archaeological population. The excavations at Bageri Chala, Bartsryal and Bover cemeteries are now finished; thus this study may be considered a summary as regards the samples from those sites. The less numerous materials from the Karakotuk and Tekhut cemeteries were used as comparative data.
Injuries to the cranial vault (compression fractures, sharp-force wounds) and facial skeleton (nasal-bone fractures, lesions of the maxilla and mandible) were identified. Their descriptions include localization, pattern, form, and size of the injury; presence of inflammation; and other features seen in the affected area. Fractures were recorded as single (the line of fracture can be traced, irrespective of the character of the fracture plane—transverse, complete or incomplete) or numerous (more than two per individual).
The methods of bioarchaeological reconstruction, based on the achievements of forensic medicine, make it possible to detect:
-
1) The weapon or other object used to cause the trauma. A sharp weapon (stabbing, cutting, or chopping) leaves characteristic lesions on bones, which are indicative of the transverse section and mechanism of action of the weapon. Incisions, furrows, and scratches emerge during the slip of the weapon along the bone’s surface. Lesions from penetration wounds (e.g. into the cranial cavity) are in the shape of a truncated cone. The surfaces of blunt objects can be of the following types: wide and flat (prevailing or restricted), spherical, cylindrical, conical, faceted, or indefinite in shape;
-
2) Position of the individual causing the trauma, and of his victim;
-
3) Consequences of the trauma: whether it was fatal, or whether there is evidence of healing of the injury. The differential diagnosis of pre-mortem injuries is related to detecting changes in the ends or margins of lesions in the form of the callus or smoothening of the bone’s margins. Healed perforated cranial fractures accompanied by penetration of the vault fragments into the cranial cavity are characterized by a smoothening of the external and internal plates, a fusion of separate fragments with neighboring bone, and a retraction of the central part of the lesion;
-
4) How long the individual lived for after being injured, and how successful the healing was. We were
following the recommendations of A. Galloway (1999: 250–252) for diagnosis and determination of the time of the trauma;
-
5) Methods of surgical intervention: clearing for removal of bone fragments, scraping of purulent-molten bone tissue. In the cases of healing after a surgical intervention, the perforation has relatively flat outlines of oval or round shape, with smooth and round (sometimes thin) margins. Classification of wounds according to the trepanation method: a) scraping, b) cutting, c) boring and cutting, d) excision of the fragment (Lisowski, 1967).
Description of traumas
In the Bageri Chala sample, evidence of trauma was observed in 7 out of 32 individuals studied (14 male, 9 female, 6 subadults, and 3 of unidentified sex).
Burial 8. Male, 20–29 years. Possible penetrating crushing injury of the right parietal (20 × 11 (?) mm). A radiating fracture was observed, but no signs of necrosis or healing.
Burial 9. Male, 40–49 years. There were mechanical breaks of the occipital (left side) on the skull base; the left mastoid process and mandibular condyle were damaged. The injuries were perimortem, and undoubtedly point to decapitation incurred when the individual was in an upright position (Manchester, 1983: 63). Linear breaks of the mastoid and condyle provide evidence that the blow was inflicted from behind (in the tangent direction), most likely by a right-hander.
Burial 10. Female, 20–29 years. Signs of a healed blunt-force injury on the left parietal. The lesion was oval in shape (13 × 8 mm). The trauma was followed by an inflammation of the affected area.
Burial 15. Adolescent male, 16–18 years. Signs of two traumatic lesions in the skull. In the right side of the frontal bone, a linear fracture was detected. Its length outside the orbit was 58 mm, and inside the orbit, 11 mm. The trauma was ante-mortem, and the diploë was closed throughout the fracture line. This suggests that the individual lived for one and a half years after receiving the injury. No signs of surgical intervention were observed. In the left parietal (closer to the coronal suture), a successfully healed blunt-force injury was detected (6.5 × 8.0 mm).
Burial 18. Male, 30–39 years. Evidence of an incomplete surgical intervention was observed in the right parietal. The size of the wound on the external surface was 23.7 × 18.5 × 9.5 × 8.2 mm. A fracture line radiated from the lesion. The injury was lethal to the individual.
Burial 22. Subadult, 8–9 years. Two penetration wounds on the left parietal. The surgery was carried out ante-mortem. The locations of the incisions were clearly visible. The first incision was located close to the sagittal suture (2 × 15 × 2 (?) × 15 (?) mm). The size of the second wound was 16 × 9 × 16 (?) × 9 (?) mm. No signs of inflammation around the wounds. The edges of the incisions were straight, sharp, and displayed no signs of healing.
Burial 28. Male, 40–49 years. A small elongated depressed fracture was observed in the right parietal (16 × 6 mm). This was probably a result of a healed blunt-force trauma. The injury had healed successfully, though there was an inflammation in the affected area.
In the sample from Bover (40 individuals: 19 males, 8 females, 2 subadults, and 11 individuals of unidentified sex), signs of trauma were detected in 8 skeletons.
Burial 7. Male, 30–39 years. A round depression of the outer bone table (33.5 × 27.0 mm) was observed on the frontal bone. Inside the lesion, there were manifestations of inflammation, which probably led to healing of the injury.
Burial 10. Male, 50–59 years. Ante-mortem blunt-force trauma of oval shape was observed on the occipital bone (supposedly 12.0 × 5.5 mm). The injury had successfully healed.
Burial 13. Male, 30–39 years. Signs of two traumatic lesions were detected on the skeleton. A round blunt-force injury healed long before death could be seen in the right parietal (size 42.0 × 35.5 mm, depth 1.5 mm). No signs of necrosis. In the sacrum, a transverse fracture was observed, which had occurred as a result of a fall on the buttocks. Manifestations of healing of the bone were detected.
Burial 27. Female, 20–29 years. Signs of two non-penetration successfully healed wounds were observed on the right parietal (28.0 × 20.0 × 5.5 and 8 × 8 mm).
Burial 35. Male, 40–49 years. Blunt-force antemortem trauma was detected on the left parietal (16 × × 15 mm).
Burial 41. Male, 40–49 years. An injury caused by a chopping weapon in the tangential direction (24 mm) was detected on the left parietal. There were signs of an acute inflammatory response, which probably led to the death of the individual.
Burial 44. Male, 40–49 years. Signs of three traumatic lesions were detected. An oval depressed fracture (26 × 16 mm), which only affected the outer table of the vault, could be seen on the right parietal. The two other lesions were on the frontal bone: an elongated lesion on the left of the metopion (16 × 4 mm), and a non-penetrating depressed fracture (8 × 3 mm) some
37 mm from the first lesion. There were no signs of inflammation in either case. Apparently, both injuries were caused during the same encounter.
Burial 51. Female, 30–39 years. Blunt-force trauma of the nasal bones was found.
In the sample from Bartsryal cemetery (38 individuals: 19 males, 6 females, 3 subadults, and 10 of unidentified sex), signs of trauma were detected in 9 cases.
Burial 1. Male, 40–49 years. Oval aperture on the left side of the frontal. Its size on the outer table was 9 × 3 mm, on the inner table 7.0 × 4.5 mm. The contours of the aperture were irregularly shaped, and asymmetrical. Such a perforation, even if small, can lead to the infiltration of infectious agents inside the cranial cavity. Six or more incisions (3 to 10 mm in size) were detected in the affected area. The individual apparently died from general sepsis, caused by an active necrosis stimulated by the infection of the cranial cavity, shortly after being injured.
Burial 9. Individual of unidentified sex, 20– 29 years. Quadrangular wound on the lateral side of the right parietal (12.0 × 10.0 × 12.8 × 5.5 mm). A surgical cleaning was carried out after the injury was caused. Healing was not complicated by inflammation.
Burial 12. Male, 30–39 years. Three traumatic lesions. A part of the right supra-orbital margin (16.5 mm), close to the lateral half of the lateral orbital margin, was cut off. Blunt-force traumas on the right parietal and on the right side of the occipital. Manifestations of healing were present.
Burial 22. Male, 50–59 years. An ante-mortem trauma (3 × 4 mm) was detected on the mandible, just above the mental eminence, at the level of the medial incisors. A small fracture line could be seen on the right side of the lesion. There was a local inflammatory response in the affected area.
Burial 34. Male, 50–59 years. Successfully healed depressed fracture of the frontal bone.
Burial 45. Subadult, 8–9 years. Probable gross crushing injury of the frontal bone, just beyond the frontal eminences. This trauma may have been a cause of the death of that individual.
Burial 57. Male, 30–39 years. A healed injury was detected in the right supra-orbital area: a round lesion (11.0 × 11.5 (?) mm) on the temporal line, near frontotemporal point. Despite successful healing, there were manifestations of a local inflammatory response. A healed blunt-force trauma suffered long before death (14.5 × 9.0 mm) was detected on the left parietal.
Burial 60. Male, 20–29 years. Blunt-force trauma (13 × 14 mm), healed long before death, on the left parietal.
Burial 67. Male, 20–29 years. Non-penetrating successfully healed oval injury on the right side of the frontal.
From 6 individuals of the Karakotuk sample (3 male, 2 female, and 1 individual of unknown sex), only one showed manifestations of trauma.
Burial 10. Male, 30–39 years. Successfully healed blunt-force (?) trauma (18.8 × 7.0 mm) on the left parietal, suffered long before death. The healing was successful, despite a local inflammatory response.
From 6 individuals of the Tekhut sample (2 male, 1 female, and 3 individuals of unknown sex), only one showed manifestations of trauma.
Burial 9. Male, 30–39 years. Rhomboid trepanation on the right parietal, 14 × 13 × 7 (?) × 9 (?) mm. Manifestations of inflammation were detected inside the lesion.
Discussion
On the basis of the results of the present study, it is possible to assess the prevalence of different types of trauma in individual cemeteries, and in the studied region in general. Lesions with the bone reaction due to a healing process were observed in 19 individuals (15 male, 3 female, 1 adolescent). Lethal traumas were described for 4 male skulls and 1 subadult skull. Three of the males had suffered traumas during the fourth decade of life, and one at the age of 20–29.
What does the pattern of prevalence of traumatic lesions tell us about the social conditions in those past populations? There are facial traumas: a healed fracture of the nasal bones (Bover, burial 51, female,
30–39 years), a lesion of the mandible (Bartsryal, burial 22, male, 50–59 years) and of the supra-orbital area (Bartsryal, burial 12, male, 30–39 years; burial 57, male, 30–39 years). The nasal-bones trauma was caused by a blow from the left, thus the woman probably stepped back and right in trying to avoid the blow. The mandibular injury was a result of a blow to the face, to the area of the anterior teeth. The supraorbital traumas were caused by contact blows from the right. This means that the men were not able to react to the blows.
Another type of trauma is the depressed blunt-force injuries to the center of the frontal bone or to its right or left sides (Bartsryal: burial 34, male, 50–59 years; burial 67, male, 20–29 years; Bover: burial 7, male, 30–39 years; burial 44, male, 40–49 years). In one case, a weak blow, caused by a right-hander standing in front of the injured, led to the emergence of a fracture line (Bageri Chala, burial 15, male, 16–18 years; Fig. 1). In all cases, signs of a healing process and the absence of an inflammatory reaction suggest that the injuries were suffered long before death.
Two other types of traumatic lesion are found on the parietal and occipital bones. Healed fractures of the parietals were observed in 9 male and 2 female individuals. In 4 male skulls (Bageri Chala, burial 28; Bover, burial 13, 44; Bartsryal, burial 12) and 1 female skull (Bover, burial 27), depressions of the outer table of the right parietal were detected. In 5 male (Bartsryal, burial 57, 60; Bover, burial 35; Karakotuk, burial 10; Bageri Chala, burial 15) and 1 female (Bageri Chala, burial 10), the lesions were found on the left side of the skull: the blows were delivered from the right. In one case, an elongated incision (24 mm) caused by

Fig. 1. Fracture line on the right side of the frontal bone (Bageri Chala, burial 15). a – outer surface; b – orbital surface.

Fig. 2. Sharp-edge incision on the skull (Bover, burial 41).

Fig. 3. Depressed fracture of the parietal bone ( a ) and transverse fracture of the sacrum ( b ) (Bover, burial 13).

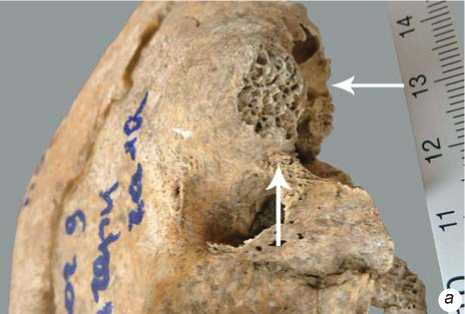
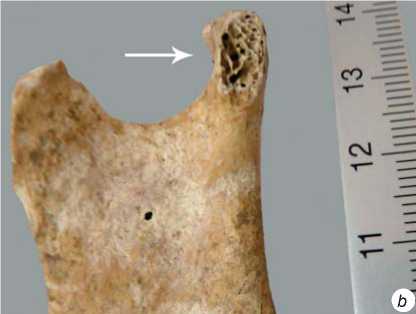
Fig. 4. Skull-base ( a ) and mastoid process ( b ) with signs of decapitation (Bageri Chala, burial 9).
a weapon with sharp cutting edge was observed on the left parietal (Bover, burial 41, male, 40–49 years; Fig. 2). The attacker was standing behind the victim; the latter was able to react to the attack, and tried to avoid it. Depressed lesions on the occipital bone were found in 2 male skulls (Bover, burial 10; Bartsryal, burial 12).
The next type is penetration wounds (perforating fractures). A penetration wound exhibiting bonereaction due to healing was observed in one individual (Bartsryal, burial 9), and without signs of healing in three individuals. Injuries of the same type on the frontal bone were detected in 2 individuals (Bartsryal, burial 1, female, 40–49 years; burial 45, subadult, 8–9 years). The pattern of the injuries suggests that sharp, straight blows were delivered to the frontal bones by a small object. The attacker was standing face to face with the victim. A young man (Bageri Chala, burial 8) displayed an oval aperture on the right parietal, with no signs of inflammation or healing.
Severe traumas are characterized by lesions of mixed type that involve several parts of the skeleton (Fig. 3). A male (Bover, burial 13) exhibits signs of a healed fracture in the form of a round depression on the right parietal. The injury shows no manifestations of the complicated process of healing, such as inflammation or osteomyelitis. After receiving a strong blow to the skull, the man probably fell onto his buttocks.
The decapitation caused by a sharp blow from a chopping weapon to an individual (Bageri Chala, burial 9; Fig. 4) points towards a direct aggression. Decapitation was also observed in two individuals from contemporaneous cemeteries from the Sevan Basin area (Khudaverdyan, 2014a).
The prevalence of skull lesions in the studied samples is highest at Bartsryal, where it is found only in males (23.7 %). In 7 cases the injuries displayed manifestations of healing, and no such manifestations in one case. Peri-mortem injuries were observed in 2 individuals: on the frontal bone (burial 1), and on the mandible, just above the mental eminence (burial 22). These males died shortly after being injured, from general sepsis, caused by an active necrosis stimulated by the infection of the cranial cavity. Two individuals that died at the fourth decade of life (burial 12, 57) displayed various lesions in the right supra-orbital area, caused by a weapon with a sharp, probably cutting, edge. In 5 cases (burial 12, 34, 57, 60, 67) blunt-force traumas on the vault were observed. Two of these skulls (burial 34 and 67) exhibit healed injuries on the frontal bone, either in the center of the bone or with a deviation to the left. These traumas were caused by an attacker standing face to face with his victim. Traumatic lesions on the left parietal were found in 2 individuals (burial 57, 60), and on the right parietal in one individual (burial 12). The later also displayed signs of trauma in the occipital region. These injuries were caused from behind by right-handers.
The prevalence of skull traumas at Bover is 20 %. They are found mostly on the male skulls, and usually these are blunt-force traumas of the vault. The injuries were observed on frontal bone (burial 7, 44; both male), on parietal bone (burial 13, 35, 44, males; burial 27, female), and on occipital bone (burial 10, female). There are reasons to suppose that in all cases a similar weapon was used. This could have been the butt of an axe, mace, or staff. One individual (burial 41) displayed signs of a chopping blow to the parietal area. Some injuries were caused during frontal encounters (traumas of frontal bone and face), while others were caused from behind (parietals and occipital area).
The prevalence of skull traumas at Bageri Chala is 15.6 %. Signs of healing were detected in 3 cases. Depressed blunt-force lesions were observed in 3 male skulls (burial 10, 15, 28). The depressions are quite small; thus the blows were caused by relatively light objects. After the injuries were caused, inflammatory response began in the affected areas. These were probably the results of domestic accidents typical of various social groups. On the right side of the frontal bone of a young man (burial 15), there is a fracture line caused by a straight-contact blow.
At Karakotuk, only one case of cranial injury was detected: trauma of the left parietal, healed long before death (burial 10, male, 30–38 years). The injury was inflicted from behind by a right-hander.
Another type of skull lesion can be considered the result of trepanation. Surgical interventions of this type were observed in 4 individuals: two males, one subadult (8–9 years), and one individual of unknown sex. They have pre-mortem apertures on the parietal bones (Khudaverdyan, 2016).
It is well-known that some types of trepanations are the results of surgery carried out in order to heal cranial injuries. A small fragment of the right parietal bone displaying a penetration wound, and human teeth were found in burial 9 at Bartsryal. These remains belonged to a mature individual. The aperture is quadrangular in shape. The surgery was probably carried out for therapeutic purposes. The wound was surgically cleaned to remove bone fragments. Margins of the aperture are sharp, at some places round, the inner and outer tables of the bone are fused. Scraping of the affected bone-tissue finally led to healing. This individual lived for one and a half years after the surgery.
A rhomboid aperture was detected on the right parietal of the 30-to-39-year-old male from the burial 9 of the Tekhut sample. There are signs of an inflammatory response in the area of trepanation. Our study shows that this individual suffered from acute mastoiditis (purulent inflammation of mastoid tissue). This pathology is usually a complication of acute purulent inflammation of the middle ear, but can also be a result of a trauma or sepsis generated by staphylococci, streptococci, viruses, or fungi. We can assume that this surgery was done for a therapeutic purpose.
Another individual (Bover, burial 7, male, 30– 39 years) displays specific lesions of the outer table of the frontal bone in the form of a round depression (Fig. 5). Such traumas with surface lesions of the outer table and, partially, diploë, can be a result of a gross crushing injury. There are signs of inflammation inside the lesion. The pattern of the demarcation surrounding the injury and the presence of trace-like scars might suggest that there were some attempts of surgical intervention, namely the scraping of the purulent-molten bone tissue. Also, the possibility of a surface trepanation cannot be excluded. Examples of such surgical procedures are found quite often, and previous workers have hypothesized that in some cases it could be related to a physical test of an individual when passing from one social category to another (initiation, marriage, bearing, mourning, etc.) (Mednikova, 2001: 125). Though it is well-known that medical aspects of trepanation closely intertwine with its ritual meanings, there are numerous observations showing that it can be considered as a method of initiation or transformation as well (Mednikova, 2001: 128–131; Khudaverdyan, 2011).
An 8–9-year-old child (Bageri Chala, burial 22) was subjected to a trepanation, which was performed using the crosscut or linear section method (Standards…,
1994: 160; Verano, 2003). Two penetration wounds were detected on his left parietal: one in the sagittal suture area, another closer to the temporal bone. There are no clear manifestations of inflammatory response. The edges of the wound are straight, sharp, without signs of healing. Porotic hyperostosis near pterion, mastoiditis, and the brain abscess were detected in this subadult as well. Porotic hyperostosis is usually thought to be associated with iron-deficiency anemia, which develops during the chronic course of the infectious and parasitic diseases. The abscess could have emerged because of an acute purulent otitis. But in this particular case, there is not enough evidence to derive firm conclusions regarding medical aspects of the surgery.
Signs of curative craniotomy done using the crosscut method were detected on the right parietal of a male (Bageri Chala, burial 18, Fig. 6). This individual did not survive the surgery. Pathological markers found on his postcranial skeleton (osteoarthritis, spinal pathologies, etc.) reflect response to a specific stress, and are related to certain physical activities. These imply a lifestyle involving intense physical labor. Manifestations of tuberculosis were also detected on the skeleton. These lesions are found on the sternum and in vertebral bodies (tubercular spondylitis). Bone tuberculosis usually emerges as a result of a hematogenous metastasis from a primary locus located in the lung or other part of the body.
Similar crosscut trepanations were previously observed on the skulls from cemeteries in Anatolia (Chavlum, Ikiztepe) (Erdal Y.S., Erdal O.D., 2011) and in Dashkesan District of Azerbaijan (Kirichenko, 2007).
In our study, we have also documented symbolic trepanations. The pattern of lesions suggests that the cuts were not a result of violence, but rather were made intentionally in strictly defined areas of the skull (frontal and parietal bones). Females were subjected to ritual trepanations along with males. On the skulls of 16 males (Bageri Chala, burial 8, 9, 11, 15, 16, 18, 23, 30; Bartsryal, burial 60, 76; Bover, burial 6, 28, 30, 35, 44, 49), 11 females (Bageri Chala, burial 4, 5, 10, 25; Bartsryal, burial 3, 19, 84; Bover, burial 42), and of one individual of unknown sex (Bover, burial 45), healed incisions from 2 to 14 mm long were observed on the parietal bones. Some of these lesions are quite deep, while others only slightly affect bone-surface. Similar scars were found on the frontal bones of three male individuals and one female (Bageri Chala, burial 27, 28; Bover, burial 41, 51). Symbolic trepanations were practiced in the tribes of the Bronze and Early Iron Ages in the Sevan Basin (Khudaverdyan, 2010). One of the important symbolic meanings of the surface

Fig. 5. Surface lesions on the skull (Bover, burial 7).

Fig. 6. A skull with signs of a pre-mortem trepanation (Bageri Chala, burial 18).
trepanation may have been a transition from one social group to another (initiation, joining a male union, marriage, bearing, etc.) (Mednikova, 2001: 128–131).
Conclusions
Summing up, our analysis of injuries on the cranial samples from the populations of the Late Bronze and Early Iron Ages leads us to the conclusion that the prevalence of traumatic lesions was moderately high in the studied samples. The comparison of the frequency of cranial traumas between the samples from cemeteries in the Shnogh River basin (present study) and contemporaneous burial grounds in the Sevan Basin and Shirak Plain (Khudaverdyan, 2014b) has shown that the frequency was higher in the former. Most of the injuries are blunt-force traumas of the vault. The fractures were in most cases healed long before death. Traumas are prevalent in males, but are also found in females. A similar pattern is seen in synchronous Armenian skeletal populations. This is quite a predictable result: males, as the most active part of the population, were more often participating in conflicts, protecting their settlements from enemy troops, etc. Lethal injuries were found in 4 male and 1 subadult individuals. The comparative analysis has shown the differences in the prevalence of traumatic lesions between the studied samples. While the prevalence is moderate at Bageri Chala (15.6 %), it is increased at Bover (20 %) and Bartsryal (23.7 %). The difference in trauma-prevalence reflects social differences between the populations.
The osteological samples collected and studied to date provide evidence that the population of the Shnogh River basin was not militarized, despite the high frequency of injuries in males*. The prevalence of transhumance and nomadic herding in the economy of this population, combined with agriculture, attracted small militarized groups that were coming into that area with a view to cattle-theft and robbery. In some cases, we cannot exclude occasional manifestations of aggression that were not a result of large-scale warfare. Items of weaponry are almost never found among grave goods in the studied cemeteries, unlike contemporaneous sites in the Sevan Basin and Shirak Plain (Martirosyan, 1964: 76–85; Torosyan, Khnkikyan, Petrosyan, 2002: 30–40). The graves of warriors are almost indistinguishable in the communal burial grounds, as they are placed alongside the graves of herders and farmers, and only differ in the abundance of grave goods and the presence of armor (Areshyan, 1974). Thus, the analysis of the traumatic lesions found on the skeletons of the people buried at the cemeteries of the Shnogh River basin dated to the 13th–11th centuries BC provides the strongest evidence of their peaceful lifestyle.
Another finding worth noting is the presence of a center of medical trepanation in the Lori Region. People of the Late Bronze and Early Iron Ages possessed all the necessary knowledge and skills to carry out such sophisticated surgery. The fact of successful (healed) trepanation is itself of principal importance for us, as it confirms the possibility of successful cranial surgery in the studied populations (Khudaverdyan, 2015; 2016). The population of the Shnogh River basin was also practicing symbolic trepanations: superficial manipulations only slightly affecting the cranial vault.
