Functional outcome of mid-sole percutaneous plantar fasciotomy versus open plantar fasciotomy in treatment of refractory plantar fasciitis

Author: Kassab Bashi S.A., Isam Y.
Journal: Гений ортопедии @geniy-ortopedii
Section: Оригинальные статьи
Article in issue: 1 т.32, 2026.
Free access
Background Plantar fasciitis is one of the main causes of heel pain, which is one of the most prevalent complaints in foot and ankle clinics. Surgery may be necessary if conservative therapies have failed. The appropriate surgical technique has been debated, open plantar fasciotomy and percutaneous plantar fasciotomy are the two common surgical techniques. The aim of the study is to compare the outcomes of open release versus percutaneous midsole release of the plantar fascia in this study to treat recalcitrant heel pain. Methods A prospective study was conducted on 54 patients who had unresponsive plantar fasciitis following conservative treatment for at least six months. 20 patients in the 54 enrolled cases had open plantar fascia release, whereas the remaining 34 patients had percutaneous mid-sole plantar fascia release. All patients' surgical outcomes were evaluated using the Foot and Ankle Disability Index (FADI) both before and after the procedure and a follow-up period of one year was used to assess the functional results. Results The percutaneous plantar fasciotomy group's mean foot and ankle disability index score improved statistically significantly from 39 ± 6 preoperatively to 101 ± 3 postoperatively, compared to 38 ± 5 preopera tively and 98 ± 2 postoperatively for the open plantar fasciotomy group at the final follow-up. Two patients in the percutaneous group experienced numbness at the site of surgery, compared to seven in the open group. By the time of the last follow-up, there had been no recurrence of pain. Discussion We performed a percutaneous release of the mid-sole plantar fascia with a minimum incision and little dissection. We could thus access the plantar fascia effectively while preserving the surrounding tissues and maintaining optimal cosmetic results. Open plantar fascia release is the most conventional technique. However, disadvantages of the surgery include large wound, longer postoperative recovery time, and potential postoperative occurrence of complex regional pain syndrome. Conclusion Both open and percutaneous plantar fascia releases resulted in a considerable improvement in the patients' limb function and pain symptoms. The long-term curative results of the two surgical treatments were identical. Due to fewer postoperative problems, percutaneous plantar fascia release is a superior procedure.
Percutaneous plantar fascia release, heel spur, plantar fasciitis, open plantar fasciotomy, plantar fasciopathy
Short address: https://sciup.org/142247051
IDR: 142247051 | UDC: 616.758.9-002-089-035 | DOI: 10.18019/1028-4427-2026-32-1-65-73
Функциональный результат чрескожной подошвенной фасциотомии по сравнению с открытой подошвенной фасциотомией при лечении пациентов с рефрактерным подошвенным фасциитом
Введение. Подошвенный фасциит — одна из основных причин боли в пятке, которая относится к наиболее распространенным жалобам в клиниках лечения стопы и голеностопного сустава. При неэффективности консервативной терапии может потребоваться хирургическое вмешательство. Вопрос о выборе хирургического метода остается открытым. Двумя самыми распространенными хирургическими методами являются открытая подошвенная фасциотомия и чрескожная подошвенная фасциотомия. Цель исследования — сравнить результаты открытого и чрескожного релиза подошвенной фасции. Методы. Проспективное исследование проведено с участием 54 пациентов с подошвенным фасциитом, консервативное лечение которых не дало результата в течение как минимум шести месяцев. У 20 из 54 включенных в исследование пациентов выполнена открытая мобилизация подошвенной фасции, тогда как у остальных 34 пациентов — чрескожная мобилизация подошвенной фасции в области средней части подошвы. Результаты хирургического лечения всех пациентов оценивали с использованием индекса нарушения функционирования стопы и голеностопного сустава (FADI) до и после операции. Функциональные результаты оценивали через год. Результаты. Средний показатель индекса функций стопы и голеностопного сустава в группе с чрескожной подошвенной фасциотомией статистически значимо улучшился с (39 ± 6) до операции до (101 ± 3) после операции по сравнению с (38 ± 5) до операции и (98 ± 2) после операции в группе с открытой подошвенной фасциотомией. Онемение в месте операции наблюдали в группе с чрескожной подошвенной фасциотомией у двух, а в группе открытой подошвенной фасциотомии — у семи пациентов. К моменту последнего контрольного осмотра рецидив боли не зарегистрирован. Обсуждение. Чрескожную мобилизацию средней части подошвенной фасции стопы выполнили через минимальный разрез с незначительной диссекцией. Это позволило получить доступ к подошвенной фасции, сохранив при этом окружающие ткани и обеспечив оптимальные косметические результаты. Открытая мобилизация подошвенной фасции является наиболее распространенной методикой. Однако к недостаткам этой операции относятся большой размер раны, более длительный период послеоперационного восстановления и потенциальное послеоперационное развитие комплексного регионального болевого синдрома. Заключение. Как открытая, так и чрескожная подошвенная фасциотомии привели к значительному улучшению функции конечности и уменьшению болевых симптомов у пациентов. Отдаленные результаты двух хирургических методов лечения были идентичны. Благодаря меньшему количеству послеоперационных осложнений чрескожная подошвенная фасциотомия является более эффективной процедурой.
Text of the scientific article Functional outcome of mid-sole percutaneous plantar fasciotomy versus open plantar fasciotomy in treatment of refractory plantar fasciitis
The most frequent cause of plantar heel discomfort is plantar fasciitis, which accounts for one million patient visits annually in the United States of America [1]. Even so, uncertainty surrounds the precise histology of plantar fasciitis. Current theories suggest that it is not caused by an inflammatory process but rather by myxoid degeneration, micro tears in the plantar fascia, collagen necrosis, and angiofibroblastic hyperplasia of the plantar aponeurosis [2]. In fact, a more appropriate term for the condition is plantar fasciosis or plantar fasciopathy; these terms continue to gain traction [3, 4].
The plantar fascia is a densely packed, subcutaneous structure that supports the foot's medial longitudinal arch and runs from the medial tubercle of the calcaneus to the metatarsal heads [5, 6]. It functions as a truss when the foot absorbs stresses in the loading phase of gait, and as a beam for the metatarsals when they experience bending forces, as in gait propulsion [6].
In many cases, patients may not improve after six months or longer of conservative treatment; hence, surgery may be recommended. The technique type is influenced by the three main etiologic factors for heel pain, which are thought to be entrapment neuropathy, plantar fasciitis, and bone spurs [7]. Numerous surgical techniques have been attempted, with varying outcomes and specifics. The most often performed operations include release of the plantar fascia with or without calcaneal spur excision, Steindler stripping, neurolysis of the first branch of the lateral plantar nerve, and endoscopic plantar fasciotomy [8].
A risk factor for plantar fasciitis could be anything that puts mechanical strain on the plantar fascia. Extrinsic and intrinsic factors are the two categories of risk factors. The patient's intrinsic variables include tight calf muscles, decreased ankle dorsiflexion range, obesity, and pes planus and pes cavus [9].
Jogging on hard surfaces, going barefoot, suddenly increasing the volume and/or intensity of one's jogging, and standing for extended periods of time are examples of extrinsic factors that are related to the environment and training [9].
Each year approximately one million office-based physician visits result in a diagnosis of plantar fasciitis [1]. Most patients initially seek care from their primary care physician [1]. Women are more likely than males to suffer from plantar fasciitis, which is most common in those between the ages of 45 and 64 [1, 10]. People with flat (planus) or high-arched (cavus) feet, long-distance runners, military personnel, people in jobs that require a lot of standing, and people who are obese or sedentary are among the other groups who are at risk [10, 11]. Bilateral plantar fasciitis may be seen in up to one-third of the affected individuals [12].
Approximately 85 % to 90 % of patients with plantar fasciitis respond well to non-surgical treatment [12]. Among the methods employed include corticosteroid injections, stretching, counter strain technique, orthoses, rest, over-the-counter (OTC) NSAIDs, ultrasound therapy, and extracorporeal shock wave therapy (ESWT). Eighty percent of individuals treated conservatively do not experience a long-term recurrence of pain, even though treatment may be needed for six months or more [1, 13].
A multimodal evidence-based approach is required for the conservative management of plantar fasciitis, according to current recommendations [14]. Only when conservative treatment has failed for at least six to twelve months is a partial or total plantar fasciotomy recommended [14]. If more than 40 % of the plantar fascia is surgically released, it may negatively impact other foot ligamentous and bony components [15]. However, according to M.S. Davies et al. [16], 75 % of patients who had surgery after failed conservative treatment reported a significant or total improvement in heel pain.
Many operative procedures have been tried with different details and results. The most commonly used procedures are release of the plantar fascia with or without calcaneal spur excision, Steindler stripping, neurolysis of the first branch of the lateral plantar nerve, and endoscopic plantar fasciotomy [17].
H.L. DuVries [18] excised the spur and freed the plantar fascia by making a medial linear incision. H.K. Hassab and A.S. El-Sherif [19] introduced calcaneal decompression using several drill holes from the medial to the lateral cortex of the calcaneus. Complications from these conventional procedures included numbness around the incision and medial heel, delayed wound healing, persistent swelling around the medial heel, plantar fat pad violation, and a stump neuroma within a painful scar after a transected medial calcaneal nerve [20].
The aim of the study is to compare the outcomes of open release versus percutaneous midsole release of the plantar fascia in this study to treat recalcitrant heel pain.
MATERIALS AND METHODS
This prospective case series study was conducted in accordance with the 1975 Declaration of Helsinki and ethical guidelines established by the responsible committee for continuing medical education at the Nineveh Health Directorate. Informed consent was obtained from each patient prior to their inclusion in the study.
Two surgeons conducted the operations for this study at the orthopedic department of AL-Mosul General Hospital and Sinjar General Hospital. The study involved 54 patients who underwent surgery in the period from January 2023 and December 2024. The sample was divided into group one (20 patients) treated with open approach for plantar fascia release and group two (34 patients) treated with percutaneous midsole plantar fascia release. Each patient in those two groups was followed up for one year postoperatively
All those patients failed to respond to a conservative trial of at least sixth months. Conservative measures included one or more of the following: activity modification, orthotics, change footwear, non-steroidal antiinflammatory therapy, physical therapy (ultrasound, stretching, and ice), immobilization, and local steroid injections. According to S.A. Hale and J. Hertel [21] analysis of the sensitivity and reliability of the FADI scales, the former are sensitive to the differences between healthy and CAI (chronic ankle instability) subjects; responsive to functional improvements in CAI subjects following rehabilitation; and reliable in identifying functional limitations in CAI subjects. The Foot and Ankle Disability Index scale (FADI) [21–24] was used as a function-specific self-report. Four stages were used to evaluate the patients using the FADI score (Table 2), and the findings were documented for comparison. Time points recorded are as follows: 1 — one week; 2 — one month; 3 — six months; 4 — one year.
Exclusion criteria
-
• Patients with peripheral neuropathy;
-
• Systemic arthropathies;
-
• Concurrent neurologic symptoms;
-
• Generalized inflammatory disorders (rheumatoid arthritis or sero-negative disorders);
-
• Wounds or skin lesions at the plantar aspect of the foot;
-
• Prior surgery for a painful heel;
-
• Time of less than six months of complaint.
Surgical technique
Percutaneous Method Technique
Following the delineation of medial and lateral margins of the central band of the plantar fascia, the procedure was performed using local anesthesia with xylocaine 2 % infiltration just distal to the fat pad of the heel. A stap wound done with blade size 15 at the med portion of central band and once the plantar fascia encountered a medial 30–40 % of the band was severed with 3 to 4 movements of the blade from the lateral to medial side, excessive manipulation should be avoided to decrease postoperative scaring (Fig. 1). In most of the cases the wounds were about 3–4 mm and no suturing was required, but if needed the wound margins were approximated with a single stitch prolene 4–0 in simple type suture. A gauze and bandage was applied.
The patients were allowed ambulating the next day as tolerated. Dressing changed at day 5 and stitch was removed on day 14.

Fig. 1. The steps of mid sole percutaneous plantar fasciotomy: a — pre-operative marking; b — mark the site of local anaesthesia; c — site of percutaneous plantar fasciotomy
Open Surgical Technique (Fig. 2)
Under general anaesthesia, supine position, tourniquet of the leg, prep and drap then putting the leg in external rotation and flexing the knee.
A transverse incision of 4 cm was performed on the medial side of the calcaneus, where the dorsal and plantar skins meet. The dissection proceeded superficially to the plantar fascia, where it separates all of the areolar tissue and fibrous bands that secure the skin to the fascia, stripping all the muscle attachment from the entire plantar surface of the calcaneus (Fig. 2). The plantar calcaneal spur was identified and removed using an osteotome chisel with bone mallet. Then half the width of the plantar fascia was divided longitudinally distal to its attachment on the calcaneus bone. The skin was closed in one layer with simple stitch, tourniquet was deflated and dressing with cotton and bandage were applied.
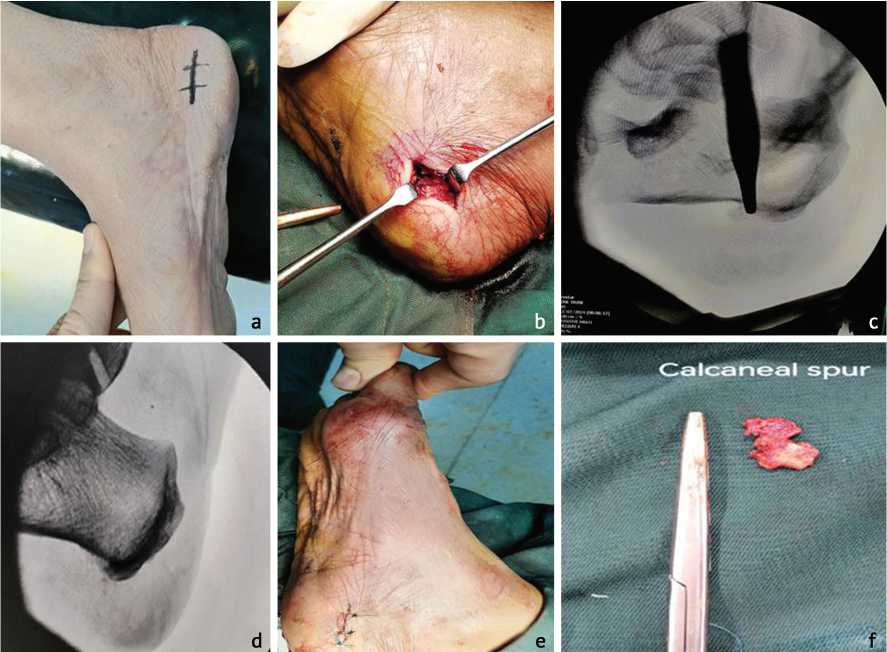
Fig. 2. The steps of traditional open plantar fasciotomy: a — preoperative marking; b — identify the plantar fascia; c — identify the calcaneal spur under fluoroscopy; d — fluoroscopy after excision of spur; e — suture of the wound by 3/0 nylon; f — calcaneal spur
Statistical analysis
Data analysis was done using SPSS (Statistical Package for Social Sciences) software version 26 (IBM Corporation, USA). Mean (± standard deviation) were used to present the numerical data, as appropriate. Paired t test was used to compare change from baseline to post procedure values. Student’s t-test was used to compare numerical variables between the two. Chi-squared test was used to compare categorical variables. A p value of < 0.05 was considered statistically significant for all statistical tests.
RESULTS
The study included 54 subjects; the mean age was 44.6 ± 5.2 years, with 18(33.3 %) males and 36 (66.7 %) females. Thirty–four of them (63 %) had percutaneous method of surgical treatment, while the other 20 (37 %) had open method of surgical treatment. There was no significant difference in terms of age, gender, or job between those who received the percutaneous method of surgical treatment and those who received the open method ( p > 0.05), although the percutaneous method subjects tended to be younger (mean age 43.5 years), Table 1.
Mean FADI (Foot and Ankle Disability Index) scores at various time points before and after the procedures for each method showed significant improvement from pre-procedure to each of post-procedure follow up at one week, one month, 6 months, and one year ( p < 0.01 in all comparisons of pre-procedure versus each of the post-procedure time point (Table 2).
Table 1
Comparison of demographic characteristics between the groups of percutaneous and open methods ( n = 54)
|
Characters |
Percutaneous Method ( n = 34) |
Open Method ( n = 20) |
p -value |
|
|
Age (years), mean ± SD |
43.5 ± 4.8 |
46.4 ± 5.4 |
0.068 |
|
|
Gender |
Male |
9 (26.5 %) |
9 (45 %) |
0.163 |
|
Female |
25 (73.5 %) |
11 (55 %) |
||
|
Job |
Home maker |
16 (47.1 %) |
9 (45 %) |
0.798 |
|
Worker |
6 (17.6 %) |
5 (25 %) |
||
|
Employee |
12 (35.3 %) |
6 (30 %) |
||
Table 2
Comparison of the mean of FADI score from pre-procedure to different time points post-procedure, stratified by percutaneous method and open method, with comparison between the two groups ( n = 54)
|
Time point |
Percutaneous method ( n = 34) |
Open method ( n = 20) |
p -value comparing between two groups |
|
FADI score |
|||
|
Pre-procedure |
39 ± 6 |
38 ± 5 |
0.404 |
|
1 week post |
67 ± 14 |
52 ± 4 |
< 0.001 |
|
1 month post |
86 ± 12 |
65 ± 4 |
< 0.001 |
|
6 months post |
95 ± 5 |
83 ± 5 |
< 0.001 |
|
1 year post |
101 ± 3 |
98 ± 2 |
< 0.001 |
Comparing the FADI scores between the two groups, the mean FADI score at pre-procedure was 39 for the percutaneous group and 38 for the open group, with no significant difference (p = 0.404), while at later follow-up FADI scores were significantly better (higher) in the percutaneous group: at 1 week post-procedure, the percutaneous group showed a significantly higher FADI score with its mean of 67 versus 52 for the open group (p < 0.001), at one-month post-procedure, the percutaneous group showed a significantly higher FADI score with the mean of 86 versus 65 for the open group (p < 0.001). Similarly, at 6 months and one year post-procedure, the percutaneous group showed a significantly higher FADI score with the mean of 95 and 101 (at 6 months and one year, respectively) versus 83 and 98 (at 6 months and one year, respectively) for the open group (p < 0.001 for both comparisons).
Figure 3 illustrates the significant improvement in the mean FADI score over time with each procedure, and highlights the significantly higher FADI scores in the subjects who underwent the percutaneous method compared to the open method.
Looking at the rate of complications, operative site numbness occurred in only 5.9 % of the subjects in the percutaneous group, compared to 35 % in the open group, with a significant difference ( p = 0.007), indicating that the percutaneous method had less incidence of this complication. Intermsof woundinfection, therewas none reported in the percutaneous group (0 %), while 5 % of the open group experienced this complication, with no significant difference ( p -value = 0.834), Table 3.
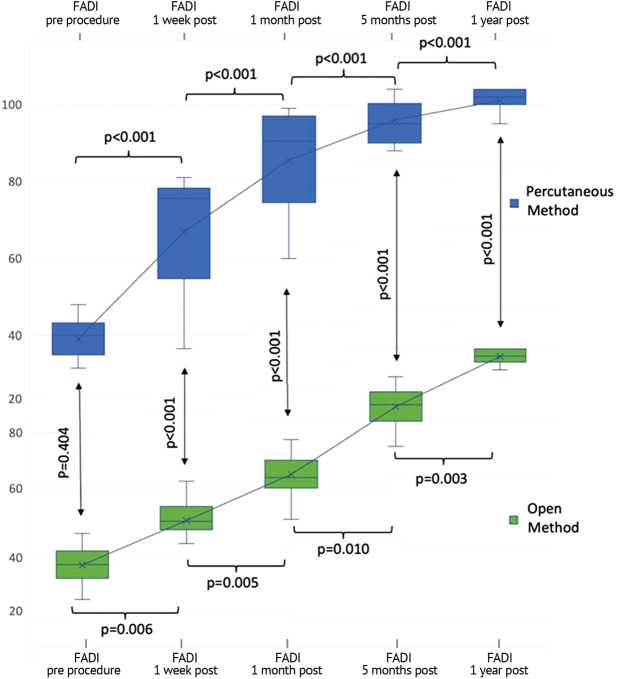
Fig. 3. Comparisons in the mean of FADI score from pre-procedure to different time points post-procedure, stratified by percutaneous method and open method, with comparison between the two groups
Table 3
Comparison of complications between the groups of percutaneous and open methods ( n = 54)
|
Complication |
Percutaneous Method ( n = 34) |
Open Method ( n = 20) |
p -value |
|
No. (%) |
|||
|
Operative site numbness |
2 (5.9) |
7 (35) |
0.007 |
|
Wound infection |
0 |
1 (5) |
0.834 |
In summary, the data suggests that the percutaneous method results in better functional outcomes (higher FADI scores) at all post-procedure time points compared to the open method, with fewer complications, particularly operative site numbness.
DISCUSSION
Plantar fasciitis is a common condition that results in heel pain due to inflammation of plantar fascia. Relieving heel pain and inflammation are the main objectives of treatment for plantar fasciitis.
It is prevalent among adults in the age between 40 and 70 years old. Employees who work standing, runners, and obese patients with a body mass index (BMI) of greater than 30 kg/m2 are the high-risk groups experiencing more severe pain. In light of this, the American Orthopaedic Foot and Ankle Society advise patients with plantar fasciitis to undergo conservative treatment for at least six months prior to surgery [25–30].
When conservative treatments fail to provide relief for refractory plantar fasciitis, surgical options may be considered like the traditional medial heel open release of plantar fascia or mini open midsole plantar fascia release with or without calcaneal decompression by multiple drilling. In our study, we compare the medial open plantar fascia release and the percutaneous midsole plantar fascia release without calcaneal drilling. The open technique leads to larger and more painful scars, requires significantly more dissection, has a longer postoperative recovery period, and can lead to numbness and nerve entrapment [25].
In a 1998 retrospective analysis, it was discovered that the miniinvasive group returned to preoperative activities the quickest, whereas the open heel spur group took the longest time to recover [26].
We performed a percutaneous release of the mid-sole plantar fascia with a minimum incision and little dissection, which ensured a simple operation with fewer adhesions after surgery and a shorter recovery period.
An important consideration for the outcome of this surgical treatment is the location of the incision. Employing a small transverse incision, we can access the plantar fascia effectively while preserving the surrounding tissues and maintaining optimal cosmetic results. The positioning of the incision not only adheres to anatomical considerations, allowing for better surgical exposure and access, but also aligns with physiological principles that reduce postoperative discomfort and minimize complications associated with scarring.
Furthermore, the technique promotes faster healing as the incision mimics the natural lines of tension within the skin, allowing for more efficient tensile strength and alignment during the recovery process. Overall, this approach enhances the surgical outcome by balancing effective intervention with patient comfort and aesthetic considerations [27].
The ideal amount of plantar fascia release is a topic of debate. S.L. Barrett and S.V. Day [28] recommended total plantar fascia resection. However, after more experience and assessment of postoperative problems, they recommended releasing only the medial portion of the plantar fascia. They believed that if the lateral fibers of the plantar fascia remained intact, the calcaneocuboid joint's locking mechanism would remain intact. This mechanism is essential for foot biomechanics during walking and running and aids in maintaining the foot arch, surgeons aim to preserve this stability while still alleviating the pain associated with plantar fasciitis by addressing the inflamed or degenerated medial portion [29–31].
Barrett and Day initially proposed complete resection of the plantar fascia but later adjusted their stance based on clinical experiences and outcomes. Their recommendation to only release the medial one–third of the plantar fascia aims to reduce the risk of complications such as instability of the foot, excessive dorsal flexion, and over-pronation, which can arise from more extensive procedures [28].
Compared to standard open medial release, the mid-sole plantar fasciotomy had fewer problems; however, a plantar incision carries the risk of severe plantar fibrosis, delayed healing, and plantar scarring [28]. In our study, none of the patients developed plantar fibrosis and scarring. Only two patients (5.9 %) developed operation site numbness. However, in the standard open medial plantar fascia release numbness at operation site occurred in 7 patients (35 %) of the open method group.
Calcaneal spur is another name for calcaneal osteophytes. A number of researchers thought that calcaneal osteophytes were a major cause of heel discomfort, and some even called it calcaneal osteophyte syndrome [34].
According to K.S. Johal and S.A. Milner research, plantar fasciitis and calcaneal osteophytes are positively correlated. However, the asymptomatic calcaneal osteophytes could not be explained by the concept [35].
In this study, no calcaneal osteophyte resection was performed on any of the patients in the percutaneous plantar fasciotomy group.
All patients had significant improvement postoperatively. We might have hypothesized that the frequency of heel discomfort and calcaneal osteophytes did not significantly correlate.
Limitation
Our findings may be impacted by a number of factors due to the prospective study design limitations, including selection bias, a small sample size, and the absence of a long-term follow-up period, in contrast to randomized clinical trials. So, further studies are recommended to assess the efficacy of mid-sole release of the plantar fascia with long-term follow-up needed to evaluate the long-term results regarding the instability and recurrence.
CONCLUSION
Our research indicates that patients with refractory plantar fasciitis can benefit greatly from both open and percutaneous plantar fascia release in terms of pain relief and limb function. Percutaneous midsole plantar fascia release may be a preferable choice when choosing surgical therapies for refractory plantar fasciitis because it has demonstrated higher postoperative function scores.
Conflict of interest Not declared.
Funding None.
