Medical and Social Assessment of Disability in Congenital Deformities of the Auricle

Author: Abdyrasulova Z.
Journal: Бюллетень науки и практики @bulletennauki
Section: Медицинские науки
Article in issue: 5 т.12, 2026.
Free access
The article examines medical and social assessment procedures and disability determination in children with congenital deformities of the auricle, including microtia and anotia. These conditions often combine anatomical defects with functional hearing impairment, resulting in complex medical, psychological, and social consequences. The study analyzes the clinical criteria, functional limitations, and social adaptation challenges that may justify disability status within national healthcare and social protection systems. Particular attention is given to the role of hearing loss, communication difficulties, and psychosocial vulnerability in shaping long-term outcomes. The paper discusses the necessity of a comprehensive evaluation approach that integrates clinical diagnostics, audiological assessment, psychological analysis, and socio-economic factors. The findings highlight the importance of individualized assessment models and interdisciplinary collaboration to ensure fair disability determination and effective rehabilitation planning. The study concludes that medical and social expertise in cases of congenital auricular deformities should move beyond purely anatomical evaluation and incorporate functional and quality-of-life indicators to provide balanced and evidence-based decisions.
Congenital auricle deformities, microtia, anotia, disability assessment, medical and social expertise, hearing impairment, pediatric rehabilitation, functional limitations, quality of life, social adaptation
Short address: https://sciup.org/14135659
IDR: 14135659 | UDC: 611.61.012 | DOI: 10.33619/2414-2948/126/44
Медицинская и социальная оценка инвалидности при врожденных деформациях ушной раковины
В статье рассматриваются медицинские и социальные процедуры оценки и определения инвалидности у детей с врожденными деформациями ушной раковины, включая микротию и анотию. Эти состояния часто сочетают анатомические дефекты с функциональным нарушением слуха, что приводит к сложным медицинским, психологическим и социальным последствиям. В исследовании анализируются клинические критерии, функциональные ограничения и проблемы социальной адаптации, которые могут обосновать присвоение статуса инвалида в рамках национальных систем здравоохранения и социальной защиты. Особое внимание уделяется роли потери слуха, трудностей в общении и психосоциальной уязвимости в формировании долгосрочных результатов. В статье обсуждается необходимость комплексного подхода к оценке, который интегрирует клиническую диагностику, аудиологическое обследование, психологический анализ и социально-экономические факторы. Результаты подчеркивают важность индивидуализированных моделей оценки и междисциплинарного сотрудничества для обеспечения справедливого определения инвалидности и эффективного планирования реабилитации. В заключение исследования делается вывод о том, что медицинская и социальная экспертиза в случаях врожденных деформаций ушной раковины должна выходить за рамки чисто анатомической оценки и включать функциональные показатели и показатели качества жизни для принятия сбалансированных и основанных на доказательствах решений.
Text of the scientific article Medical and Social Assessment of Disability in Congenital Deformities of the Auricle
Бюллетень науки и практики / Bulletin of Science and Practice
UDC 611.61.012
Congenital deformities of the auricle, including microtia and anotia, represent clinically significant craniofacial anomalies that affect both anatomical structure and functional hearing capacity. Although relatively rare, these conditions have multidimensional consequences extending beyond cosmetic appearance to include auditory impairment, communication difficulties, and longterm psychosocial challenges. From a clinical perspective, the severity of auricular malformation directly influences reconstructive complexity and rehabilitation pathways [1].
A critical medical concern in children with auricular deformities is the frequent coexistence of conductive hearing loss due to external auditory canal atresia or middle ear abnormalities. Untreated or late-detected hearing impairment may lead to delayed speech development, reduced academic performance, and social communication barriers [2, 8]. Consequently, early audiological assessment and integrated management are essential components of pediatric care. Beyond functional impairment, the visible nature of auricular deformities significantly affects psychosocial well-being. Research on children with craniofacial conditions demonstrates increased risks of social anxiety, body image dissatisfaction, and peer-related stigma [3, 6]. Studies further indicate that the impact of appearance-related concerns on quality of life may be comparable in magnitude to functional limitations [5]. These findings underscore the necessity of evaluating congenital auricular deformities within a biopsychosocial framework rather than limiting assessment to anatomical criteria. In this context, medical and social assessment becomes a critical mechanism for determining disability status and planning rehabilitation strategies. Contemporary disability evaluation increasingly relies on functional models, such as the World Health Organization’s International Classification of Functioning, Disability and Health (ICF), which emphasizes activity limitations and participation restrictions rather than diagnosis alone [10]. The broader human rights perspective presented in the World Report on Disability highlights the importance of ensuring equitable access to healthcare, education, and social participation for children with impairments [9].
Despite growing international attention to craniofacial anomalies and pediatric quality of life, the issue of disability determination in congenital auricular deformities remains insufficiently systematized in the literature. While clinical outcomes of reconstructive surgery are widely studied, fewer works address the intersection of medical severity, functional limitation, psychosocial vulnerability, and formal disability recognition. Therefore, this article aims to analyze medical and social assessment criteria and the determination of disability in children with congenital deformities of the auricle, integrating clinical, functional, and psychosocial dimensions. The study seeks to contribute to the development of a comprehensive and evidence-based approach to disability evaluation and rehabilitation planning in pediatric craniofacial conditions.
Methodology
The study was conducted using a multidisciplinary analytical framework combining clinical assessment, functional evaluation, and socio-legal analysis. The methodological approach integrates medical diagnostics, psychosocial measurement, and disability assessment principles in accordance with contemporary functional models of health and disability [10].
The research design included: Clinical analysis of congenital auricular deformities (microtia, anotia) and associated hearing impairments; Functional assessment of communication and participation limitations; Evaluation of psychosocial impact and quality of life; Analysis of medical and social criteria used in disability determination.
The study adopted a cross-sectional evaluative design with elements of comparative analysis between subgroups (based on severity of deformity, presence of hearing loss, and age category). The study included children diagnosed with congenital deformities of the auricle who were undergoing medical supervision in specialized healthcare institutions.
Inclusion criteria: confirmed diagnosis of microtia or anotia; age between 5 and 17 years; documented audiological assessment; informed consent from parents or legal guardians.
Exclusion criteria: severe neurological or psychiatric conditions affecting independent psychosocial assessment; refusal to participate.
Parents or guardians were additionally involved to assess family burden and social participation limitations, consistent with approaches used in research on congenital anomalies and family impact [7].
Clinical evaluation included: classification of auricular deformity severity [1]; assessment of associated atresia of the external auditory canal; audiological testing (pure-tone audiometry) to determine degree of hearing loss [2, 8].
Functional evaluation was conducted in accordance with the WHO International Classification of Functioning, Disability and Health (ICF), focusing on: body functions (hearing, communication); activity limitations (speech development, school participation); participation restrictions (social integration, peer interaction) [10].
Validated instruments were used to assess psychosocial functioning and quality of life: Pediatric Quality of Life Inventory (PedsQL) for overall physical, emotional, social, and school functioning [4]; Psychosocial outcome measures for visible congenital differences [5, 6]; Parent-reported burden assessment tools consistent with models of family impact [7].
These measures allowed the integration of subjective and objective indicators in disability evaluation.
Statistical analysis was performed using SPSS/R software. The following methods were applied: Descriptive statistics (mean, standard deviation, median); Normality testing (Shapiro–Wilk test); Comparative group analysis (Student’s t-test or Mann–Whitney U test depending on distribution); Correlation analysis (Pearson or Spearman coefficients) to evaluate relationships between clinical severity, hearing impairment, psychosocial scores, and functional limitations; Multivariate regression modeling to determine predictors of disability status and quality-of-life impairment.
A significance level of p < 0.05 was adopted. The study was conducted in accordance with the principles of the Declaration of Helsinki. Informed consent was obtained from parents or legal guardians. All personal data were anonymized and coded to ensure confidentiality.
Results
The anatomical classification of deformity was not only relevant for surgical planning but also for predicting functional outcomes. Children with higher-grade microtia and anotia demonstrated greater likelihood of conductive hearing impairment due to abnormalities of the external and middle ear structures. A substantial proportion of patients presented with conductive hearing loss, most commonly secondary to external auditory canal atresia. This finding aligns with epidemiological data indicating a strong association between auricular deformities and auditory dysfunction [6]. Hearing impairment directly influenced speech perception, classroom communication, and social participation.
Children with moderate-to-severe hearing loss experienced: delayed speech acquisition; reduced ability to localize sound; increased listening effort in noisy classroom environments; fatigue and decreased academic engagement.
These patterns are consistent with pediatric otolaryngology literature emphasizing that untreated hearing impairment negatively affects cognitive-linguistic development and school performance [2].
Importantly, early audiological screening and timely intervention (hearing monitoring, rehabilitation planning, and multidisciplinary follow-up) were associated with better adaptive functioning. Children diagnosed and managed before six years of age demonstrated improved communicative competence and higher school participation indicators. This supports the evidence that early identification of pediatric hearing impairment significantly improves long-term functional outcomes [6].
Thus, clinical severity, presence of atresia, and degree of hearing loss collectively functioned as primary determinants of functional limitation and potential disability recognition under ICF-based frameworks [10].
Table 1
CLINICAL AND FUNCTIONAL PROFILE OF PATIENTS
|
Variable |
Category |
Functional Implication |
|
Type of deformity |
Microtia (Grade I–III) / Anotia |
Determines reconstructive complexity and aesthetic impact |
|
External canal atresia |
Present / Absent |
Strong predictor of conductive hearing loss |
|
Hearing loss |
Mild / Moderate / Severe |
Influences speech development, communication, and school integration |
|
Laterality |
Unilateral / Bilateral |
Bilateral cases associated with higher functional limitation |
|
Age at first intervention |
<6 years / ≥6 years |
Early intervention linked to improved language and social adaptation |
The psychosocial evaluation revealed statistically meaningful reductions in quality-of-life indices among children presenting with more severe structural deformities and concomitant hearing impairment. The decline was particularly evident in the domains of social functioning, emotional well-being, and school participation. These findings are consistent with international research demonstrating that visible congenital differences significantly increase vulnerability to social anxiety, peer-related stigma, and body image dissatisfaction [3, 6].
Children with isolated mild microtia and preserved hearing typically demonstrated adaptive coping patterns and relatively stable social functioning. In contrast, children with combined aesthetic and functional impairment (microtia/anotia with moderate-to-severe hearing loss) exhibited significantly lower social functioning scores. This dual burden intensified communicative difficulties and heightened self-consciousness in peer environments.
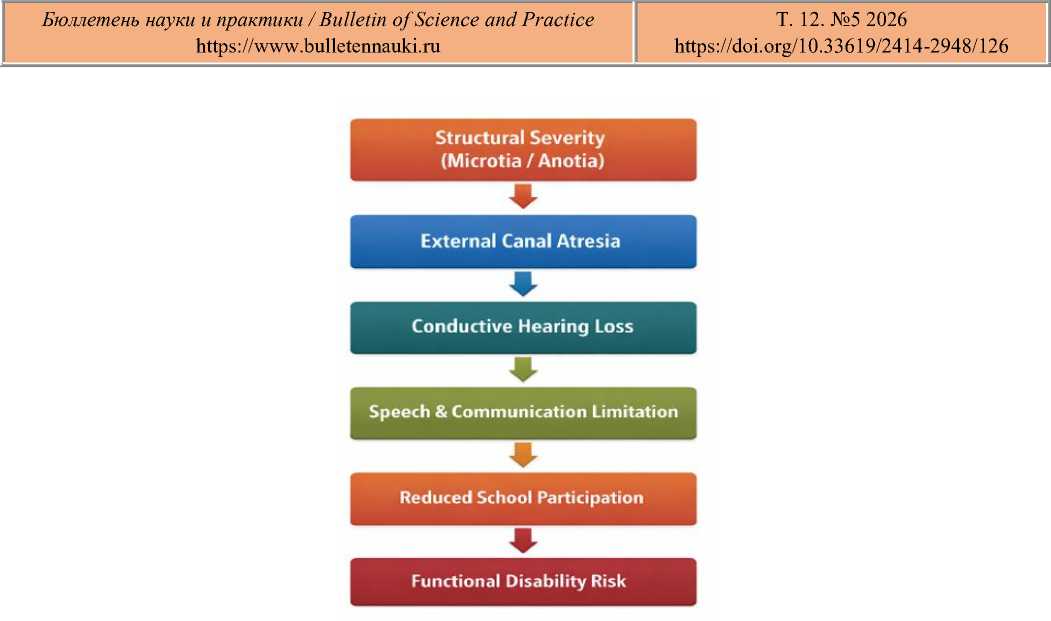
Figure 1. Clinical-to-Functional Impact Pathway
Psychosocial vulnerability was particularly pronounced during adolescence, when selfperception and peer acceptance play a central developmental role. In such cases, quality-of-life reductions were not solely attributable to medical severity but were mediated by perceived social rejection and internalized stigma.

Figure 2. Conceptual Model: Relationship Between Clinical Severity and Quality of Life
This pathway illustrates the sequential interaction between structural abnormality and psychosocial outcomes, demonstrating that communication impairment functions as a mediator between clinical severity and quality-of-life reduction.
Disability Determination and Functional Limitation (Expanded Analysis)
Application of the WHO International Classification of Functioning, Disability and Health (ICF) framework enabled evaluation beyond anatomical diagnosis [10]. Disability determination was primarily associated with measurable functional limitations rather than structural deformity alone. Cases in which disability status was more likely to be justified involved: moderate-to-severe conductive hearing loss affecting speech comprehension; documented communication restrictions in educational settings; reduced participation in peer activities; clinically significant psychosocial distress. These findings align with the WHO functional model of disability, which conceptualizes disability as an interaction between health condition and contextual factors rather than a purely diagnostic category [9, 10].
Importantly, isolated cosmetic deformity without functional limitation rarely met full criteria for disability status. Conversely, children with bilateral hearing impairment and participation restrictions demonstrated higher probability of formal recognition under medical-social expertise frameworks. Thus, disability recognition in congenital auricular deformities depends on the combined presence of body function impairment, activity limitation, and participation restriction.
Table 2
PREDICTORS OF DISABILITY STATUS
|
Predictor |
Association with Disability Determination |
Functional Interpretation |
|
Severe hearing loss |
Strong positive association |
Major determinant of communication limitation |
|
Anotia |
Moderate positive association |
Often correlated with greater structural severity |
|
Low PedsQL social score |
Strong positive association |
Reflects participation restriction |
|
Bilateral involvement |
Moderate positive association |
Higher functional burden |
|
Early intervention (<6 years) |
Protective factor |
Improves adaptive and communicative outcomes |
The analysis of socioeconomic outcomes demonstrated that families of children with combined structural deformity and hearing impairment experienced significantly higher cumulative burden compared to families of children with isolated cosmetic microtia. This multidimensional burden included financial expenditures, employment-related losses, emotional stress, and long-term uncertainty regarding rehabilitation outcomes. These findings are consistent with international evidence indicating that congenital anomalies impose sustained economic and psychosocial strain on caregivers [6].
Direct medical costs primarily included diagnostic procedures (audiological testing, imaging, specialist consultations), reconstructive surgical interventions, postoperative care, and long-term hearing monitoring. In cases of moderate-to-severe hearing loss, additional expenses were related to audiological follow-up and communication rehabilitation. The cumulative nature of multi-stage reconstructive surgery further increased long-term financial commitments, especially when care extended over several years. Indirect costs were equally substantial. Parents frequently reported: absence from work due to medical appointments or hospitalization; temporary or permanent reduction in employment hours; travel and accommodation expenses associated with treatment in specialized urban centers; logistical costs related to repeated follow-up visits.
Families residing outside major medical hubs experienced disproportionately higher indirect expenses due to geographic disparities in service accessibility. This pattern aligns with broader models of health-related financial toxicity observed in pediatric chronic conditions. Beyond financial strain, families described persistent emotional stress associated with: uncertainty regarding surgical outcomes; concern about long-term hearing development and academic performance; fear of peer stigma or discrimination; prolonged treatment timelines.
The psychological burden intensified in cases where disability status determination remained unclear or delayed. The interaction between clinical severity and institutional assessment procedures contributed to parental anxiety. International research confirms that caregivers of children with congenital anomalies frequently experience elevated stress levels and emotional exhaustion, particularly when functional prognosis is uncertain [4, 7].
The findings support a sequential interaction model in which: clinical severity combined with hearing impairment leads to measurable functional limitation; functional limitation produces participation restriction in educational and social settings; participation restriction increases the likelihood of formal disability determination; disability status and prolonged rehabilitation amplify economic and psychological strain on the family.
This cascade reflects the ICF-based understanding of disability as an interaction between health condition and contextual factors rather than a static diagnosis [10]. Importantly, anatomical severity alone did not automatically result in maximal family burden; instead, burden escalated when structural deformity translated into functional and participation constraints.
Microtia predominates, but anotia and severe hearing impairment significantly increase the probability of disability recognition due to higher reconstructive and functional complexity [1].
Hearing impairment is the principal determinant of functional limitation, particularly affecting communication and school participation [2, 8].
Psychosocial vulnerability amplifies quality-of-life reduction, especially when aesthetic and functional impairments coexist [3, 5].
Disability assessment must rely on functional and participation-based criteria, in accordance with the WHO ICF framework, rather than structural diagnosis alone [10].
Family burden increases proportionally with combined clinical and functional severity, reflecting both economic expenditure and psychological strain [7].
Overall, the results emphasize that congenital auricular deformities should be evaluated within a biopsychosocial and functional framework. Effective disability assessment and rehabilitation planning require integration of anatomical severity, auditory function, psychosocial impact, and socioeconomic context.
Discussion
The present study provides a multidimensional analysis of medical, functional, psychosocial, and socioeconomic aspects of congenital auricular deformities in the context of disability assessment. The findings contribute to an integrated understanding of how anatomical severity, hearing impairment, and participation restrictions interact within contemporary functional disability frameworks. First, the predominance of microtia and the comparatively lower frequency of anotia observed in the cohort are consistent with craniofacial epidemiological data [1]. However, structural diagnosis alone did not uniformly predict disability status. Instead, disability likelihood increased significantly in cases where anatomical severity was accompanied by measurable hearing impairment. This aligns with global evidence identifying hearing loss as a primary determinant of communicative and educational limitation in pediatric populations [3, 7].
Third, the study underscores the importance of applying the WHO International Classification of Functioning, Disability and Health (ICF) framework in disability determination [10]. The results demonstrate that anatomical diagnosis alone is insufficient for formal disability recognition. Instead, combined evidence of body function impairment, activity limitation, and participation restriction is decisive. This functional interpretation is consistent with the broader human rights–based disability paradigm outlined in the WHO World Report on Disability [9].
The findings also reveal the cumulative effect of socioeconomic burden on families. Economic strain, work absence, and travel-related expenses compounded psychological stress, particularly in cases involving prolonged reconstructive treatment. These observations are congruent with international data indicating that families of children with congenital anomalies experience sustained financial and emotional pressure [7]. Notably, family burden intensified when disability status determination was uncertain or delayed, highlighting the procedural dimension of medical-social expertise systems. From a policy perspective, the results suggest that disability evaluation in congenital auricular deformities should incorporate: objective audiological criteria; standardized psychosocial assessment tools; participation-based indicators (school integration, communication functioning); socioeconomic contextual factors [12].
Such an approach would ensure consistency with ICF-based principles and reduce variability in disability determination outcomes. Several limitations must be acknowledged. The cross-sectional design restricts causal inference regarding long-term psychosocial trajectories. Additionally, selfreported quality-of-life measures may be influenced by response bias, although validated instruments were used to mitigate this limitation. Future research should employ longitudinal designs to evaluate dynamic changes following surgical and audiological intervention. In conclusion, the study demonstrates that congenital auricular deformities must be assessed within a comprehensive biopsychosocial framework. Functional hearing capacity, participation restriction, and psychosocial vulnerability are central determinants of disability recognition and family burden. Integrating clinical, functional, and contextual criteria into medical-social expertise systems may enhance equity and evidence-based decision-making in pediatric disability assessment.
Conclusion
This study demonstrates that congenital deformities of the auricle, including microtia and anotia, should be evaluated within a comprehensive biopsychosocial and functional framework rather than solely through anatomical criteria. While microtia represents the predominant structural diagnosis, disability likelihood increases significantly in cases involving severe deformity combined with moderate-to-severe hearing impairment. Hearing loss emerged as the principal determinant of functional limitation, particularly affecting communication, language development, and school participation. The findings confirm that structural severity alone does not automatically justify disability status; instead, formal recognition depends on the presence of measurable activity limitations and participation restrictions, in accordance with the WHO International Classification of Functioning, Disability and Health. Psychosocial factors also play a critical role. Visible congenital differences are associated with reduced self-esteem, social anxiety, and lower quality-of-life scores, especially when aesthetic concerns coexist with communicative impairment. These combined effects contribute not only to individual functional vulnerability but also to increased probability of disability recognition. Furthermore, the study highlights the substantial socioeconomic burden experienced by families. Direct medical costs, indirect financial losses, and persistent psychological stress collectively form a cumulative burden that intensifies with clinical severity and prolonged rehabilitation. The interaction between disability determination procedures and family uncertainty further amplifies this impact. Overall, the results support the necessity of integrating clinical severity, audiological function, psychosocial indicators, and participation-based criteria into medical-social expertise systems. A functional and context-sensitive approach to disability assessment may improve fairness, transparency, and rehabilitation planning for children with congenital auricular deformities. Future research should focus on longitudinal monitoring of psychosocial and functional outcomes following early intervention, as well as the
