Acromioclavicular joint dislocation: reconstruction of coracoclavicular ligament with fiber tape by using a new knot technique

Author: Shinde M.B., Patel M.R., DasGupta B., Sharma A., Sarwey K., Jethliya S., Jain R., Kedia D., Chunawala S., Kowe C., Chiwadshetti S., Singh Y.N.
Journal: Гений ортопедии @geniy-ortopedii
Section: Новые технологии
Article in issue: 6 т.31, 2025.
Free access
Introduction Injuries to the acromioclavicular joint (ACJ) can range from modest, transient pain to significant displacement, chronic pain, and shoulder biomechanical changes that result in long-term disability. We aimed to evaluate the functional outcome of anatomical reconstruction of the ACJ using fiber tape, as in type III–VI AC joint dislocations. Materials and Methods In this study, 28 patients with AC joint dislocation (Rockwood type III–VI) were managed by surgical fixation using fiber tape from November 01, 2019, to October 31, 2024, at the tertiary care center. After providing written informed consent, the study enrolled patients who satisfied the inclusion criteria. The mean age of the participants was 36.50. Preoperative, three-month, and six-month UCLA shoulder scores were assessed. Results The UCLA scores increased from 29.20 at three months to 35 at six months. Radiological evaluation at each visit suggested a 100.0 % success rate of this method. No participants had surgical site infection (SSI). Discussion Several treatment options have been described for managing AC joint dislocations, including various implants and fixation methods, such as Bosworth screws, wires, locking plates, and hook plates. Unfortunately, these methods often lead to hardware-related complications, necessitating implant removal. The advantages of fiber-tape fixation technique include short surgery time, small incisions, fast recovery, cost-effectiveness, and ease of reproducibility. Conclusions Open reduction internal fixation with a knot using fiber tape for type III–VI AC joint injuries is a viable surgical option. It has the advantages of being stable, single surgery, and excellent functional outcomes. However, extensive multicentric comparative studies are required to draw definitive conclusions.
Fiber tape, Acromioclavicular joint, open reduction, loop end, Rockwood type
Short address: https://sciup.org/142246511
IDR: 142246511 | UDC: 616.727.13-001.6-009.7:616.75-089 | DOI: 10.18019/1028-4427-2025-31-6-798-804
Вывих акромиально ключичного сустава: реконструкция коракоклавикулярной связки волоконной лентой с использованием новой узловой техники
Введение. Боль при травмах акромиально-ключичного сустава (АКС) может варьировать от умеренной преходящей до хронической при значительном смещении. Значительные смещения и биомеханические изменения плеча, присущие данной травме, приводят к длительной потере трудоспособности. Цель работы — оценить функциональный результат анатомической реконструкции АКС при применении новой технологии с использованием фиброзной ленты при вывихах АКС III–VI типов. Материалы и методы. В период с 01 ноября 2019 года по 31 октября 2024 года в третичном медицинском центре мы пролечили 28 пациентов с вывихом АКС (тип III–VI по Rockwood), используя хирургическую фиксацию волоконной лентой. В исследование вошли пациенты, удовлетворяющие критериям включения и подписавшие информированное согласие на участие в исследовании. Средний возраст участников составил 36,5 лет. Оценивали показатели состояния плечевого сустава до операции, через три и шесть месяцев по UCLASS (англ.: University of California at Los Angeles Shoulder Score). Результаты. Показатели по шкале UCLA увеличились с 29,2 через три месяца до 35,0 баллов через шесть месяцев. Рентгенологическая оценка на контрольных осмотрах свидетельствовала о 100 % успешности данного метода. Ни у одного участника не отмечена инфекция в области хирургического вмешательства. Обсуждение. Описано несколько вариантов лечения вывихов акромиально-ключичного сустава, включая различные имплантаты и методы фиксации, такие как винты Босворта, спицы, блокируемые пластины и крючковые пластины. К сожалению, эти методы часто приводят к осложнениям, требующим удаления имплантатов. Преимуществами метода фиксации волоконной лентой являются короткое время операции, небольшие разрезы, быстрое восстановление, экономическая эффективность и воспроизводимость. Заключение. Открытая редукционная внутренняя фиксация узлом с использованием волоконной ленты при повреждениях АКС III–VI типов является жизнеспособным вариантом хирургического лечения. К его преимуществам можно отнести стабильность, однократность операции и отличные функциональные результаты. Однако для окончательных выводов необходимы обширные многоцентровые сравнительные исследования.
Text of the scientific article Acromioclavicular joint dislocation: reconstruction of coracoclavicular ligament with fiber tape by using a new knot technique
The acromioclavicular joint (ACJ) is one of the important components of the shoulder girdle and plays a significant role in normal shoulder movements and biomechanics [1]. Several mechanisms can lead to ACJ injuries, such as direct or indirect trauma. These injuries can be minor, with temporary joint pain, but can sometimes lead to substantial displacement, persistent pain, and alterations in shoulder biomechanics, resulting in long-term impairment [2, 3]. Young, active males are more prone to these injuries. Rockwood classified these injuries into six types based on the integrity of the acromioclavicular ligament (AC ligament) and coracoclavicular ligament (CC ligament) [4]. Type I (a mild sprain of the AC ligament with the CC ligament intact) and Type II (a ruptured AC ligament with a sprained CC ligament) injuries are best managed conservatively. However, Type III (a ruptured AC and CC ligaments), Type IV (posterior displacement of the clavicle into the trapezius), Type V (gross and severe displacement of the distal clavicle superiorly), and Type VI (a dislocated AC joint with the clavicle displaced inferiorly to the acromion or coracoid) require surgical intervention [5]. Additionally, fractures at the lateral end of the clavicle are associated with injuries to the CC ligaments [6, 7]. Injury to the CC ligament leads to superior migration of the clavicle lateral end, associated with pain, deformity, and skin tenting. The goal of surgery is to reduce the acromioclavicular and coracoclavicular intervals [8].
Several surgical techniques and implants have been described for the management of ACJ dislocation and lateral end clavicle fractures. Hook plate fixation is the most commonly performed procedure for these injuries. However, this surgery is associated with some complications, such as hardware prominence, irritation, and shoulder stiffness, which may require a second surgery to remove the implant [9]. Other fixation techniques include open reduction and internal fixation with cannulated cancellous screws, suture fixation, acromioclavicular pin fixation, and the use of a semitendinosus graft. The CC screw and suture fixation methods are associated with a risk of fracture of the clavicle or coracoid process [10]. Pin migration is a potential complication with AC pin fixation, and donor site morbidity is a concern with the semitendinosus graft [11, 12].
We describe a new technique that uses a fiber tape. This novel study employs a special fiber tape knot for fixation and prospectively analyzes the fixation of Type III–VI ACJ injuries and lateral end clavicle fractures. As far as we are aware, this surgery is not frequently performed.
The study aims to investigate the long-term outcomes and functional improvements achieved through the use of this special knot with a fiber tape for the fixation of Type III–VI ACJ injuries at three-month and six-month follow-ups, using the UCLA shoulder scoring system. Analyzing the efficacy of this technique prospectively offers important insights into its potential as a cutting-edge method in orthopedic surgery. Furthermore, by enhancing surgical methods and rehabilitation regimens for patients with lateral end clavicle fractures and ACJ injuries, this study may improve the patient's overall recovery and quality of life.
MATERIALS AND METHODS
This is a prospective outcome study carried out at the department of orthopaedics of a tertiary care center from January 2020 to December 2023, after the approval of the institutional ethics committee. All patients between 18 and 60 years of age, presenting with acute AC dislocation (Rockwood type III–VI, within two weeks of injury) and lateral end clavicle fractures, were included in the study. Patients with chronic AC dislocation (more than two weeks), polytrauma, open fractures, or fractures of the coracoid process, acromion, scapula, or proximal humerus, as well as those with type I, type II, or type III AC dislocations as per the Rockwood classification, critically ill patients, or patients unfit for anesthesia, and patients under 18 years or over 60 years of age, were excluded from the study. Based on the inclusion criteria patients were enrolled in this study and their informed consent was taken. All data were documented in the study proforma. The UCLA shoulder score is used to evaluate functional outcomes at three and six months [13, 14].
Our study group involved 28 patients who underwent anatomical reconstruction for AC joint injury. The mean (SD) of age (years) of our study group ranging from 20 to 50 years was 36.50 (9.86). The majority 26 (93 %) of the participants in the group were males. The two most typical injury mechanisms were road traffic accident 14 (50 %) and fall from stairs 9 (32 %, respectively). Twenty-one (75.0 %) participants in the group had Rockwood classification type III while seven patients (25.0 %) in the group had Rockwood classification type V.
Surgical Technique
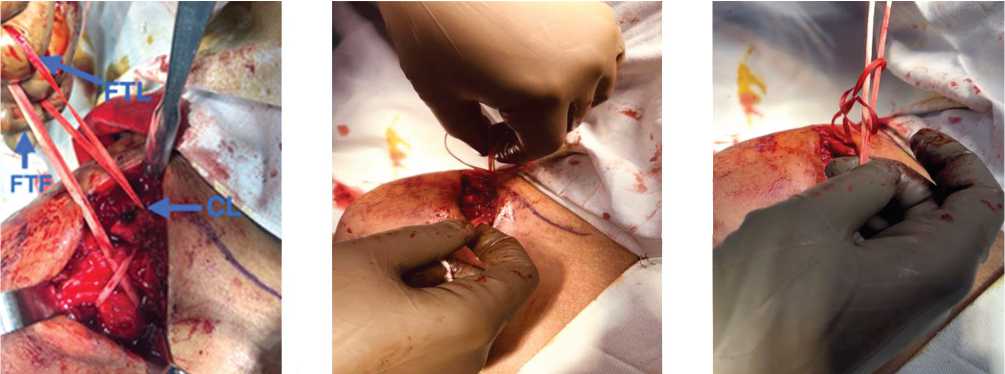
All acute Rockwood III–VI ACJ separations and lateral end clavicle fractures were considered for reconstruction. The patients were given either regional or general anesthesia, depending on the ASA grade or the anesthetist’s preference. Preoperative broad-spectrum antibiotics were administered. A beach chair position was given, and scrubbing, painting, draping, and marking done (Fig. 1). Approximately five centimeters in length, a vertical skin incision was made from the clavicle lateral end to the coracoid process tip and the coracoid process was identified (Fig. 2). From 4 cm of the lateral end of the clavicle, a 4-mm tunnel was drilled. The loop end of the fiber tape was passed from medial to lateral with a passer so the loop end is on the lateral side and the free end is on the medial side of the coracoid (Fig. 3). The looped end was passed through the drill hole at the lateral end of the clavicle and brought anteriorly (Fig. 4). The free ends of the fiber tape were then passed through the loop and tied under tension with a special knot. A diagrammatic representation of this technique is shown in Figures 1–9.

Fig. 1. Landmark and marking
Fig. 2. Identification of coracoid process (CP)
Fig. 3. Passing the fiber tape (FTL — a loop end and FTF — a free end)
-
Fig. 4. Passing the loop end
-
Fig. 5. Making a knot with the
Fig. 6. Passing the free end
(FTL) from the clavicle (CL)
loop end through a knot in loop end

Fig. 7. Pulling the free end through a knot in loop end
Fig. 8. Pre-op X-ray
Fig. 9. Post-op X-ray
Postoperative rehabilitation began the following day. During follow-up visits, patients were evaluated for functional outcomes using the UCLA shoulder score at three and six months.
Statistical analysis of the data was performed using SPSS software, version 22. The Wilcoxon test was conducted to calculate the p -value, with a p -value of < 0.05 considered statistically significant.
RESULTS
The mean (SD) UCLA score increased from 29.20 (1.68) (range 30–35) at three months to a maximum of 35.00 at the six-month review. The improvement in the UCLA score at six months was statistically significant (Wilcoxon test: V = 0.0, P = 0.001). Radiological evaluation confirmed 100 % reduction and congruence among the participants.
Most of the group participants (96.5 %) had no complications. Only one patient (3.5 %) showed deep vein thrombosis (DVT). No participants in the group had surgical site infections.
DISCUSSION
Rockwood type III–VI AC joint dislocations require surgical intervention to restore shoulder girdle function. Clinically, these dislocations may present with bruising, swelling, and skin tenting. X-rays of the affected shoulder help in determining the type of AC joint dislocation. Several treatment options have been described for managing AC joint dislocations, including various implants and fixation methods, such as Bosworth screws, wires, locking plates, and hook plates. Unfortunately, these methods often lead to hardware-related complications, necessitating implant removal and procedure-specific issues.
H.Y. Lin et al. [15] conducted a USG study showing that hook plates may cause subacromial shoulder impingement and rotator cuff lesions. Other issues include hardware prominence and the need for a second surgery to remove the implant. C. Kirchhoff et al. [16] found that the Weaver–Dunn procedure, along with its modifications, is associated with high rates of re-dislocation and coracoid fractures. This may be because the transferred ligaments are weaker than native coracoclavicular (CC) ligaments and cannot replicate their natural anatomy, as demonstrated by O. Galasso et al. [17]. AC joint pin fixation is also associated with complications such as pin breakage and migration, which can injure vital structures, including the brachial plexus, as reported by R. Ma et al. [18].
The use of a semitendinosus graft is associated with donor site morbidity, and no study has shown that biological fixation is superior to the use of fiber tapes. As a result, autogenic, allogenic, and synthetic grafts have been developed to anatomically restore the CC ligaments, leading to improved structural and functional outcomes and reduced complications. This study aims to reconstruct the CC ligaments in both AC joint dislocations and lateral end clavicle fractures using a fiber tape with a special knot in Rockwood type III–VI AC joint dislocations.
In our study, most patients were 20–50 years old. The highest incidence of injury was observed in the male population (93 %). High-grade injuries were primarily caused by road traffic accidents (50 %), followed by falls from stairs (32 %) and slip-and-fall incidents (18 %). Seventy-five percent of the cases reported were type III, while the remaining cases were type V dislocations. Similar demographic findings were reported by C. Chillemi et al. [19], who found that 50 % of dislocations occurred in the 20–40 year age group. The incidence was 1.8 per 10,000 people per year in their study, with a male-to-female ratio of 8.5:1 and sports injuries as the most prevalent mechanism. Sports injuries were the most common traumatic mechanism, and Rockwood type III dislocations were the most common. Our results are also consistent with those of J.S. Nordin et al. [20], who reported the incidence of ACJ dislocation to be two per 10,000 persons annually, with a male preponderance in the younger age group. They also found good clinical and radiological outcomes, along with a low failure rate at follow-ups.
We used a fiber tape for the reconstruction of the coracoclavicular ligament (CCL) in both AC joint dislocations and lateral end clavicle fractures. The loop end of the fiber tape is passed below the coracoid process from medial to lateral, and a 4 mm drill hole is created 4 cm medial to the AC joint. The loop end is then passed through this hole, and a knot is used to reconstruct the CCL ligament. We regularly followed up our patients, evaluating their UCLA scores and X-rays at three and six months. A.J. Guzman et al. [21] used fiber tape for AC joint repair with the suture cerclage tension system in 16 patients, considering it a viable and cost-effective technique for restoring vertical and horizontal stability. The effectiveness of fiber tape in AC joint dislocation was demonstrated by G. Vrgoč et al. [22], who showed that fiber tape offers a shorter recovery period and a significantly more cost-effective outcome in their study on 16 patients. N.W. Tully et al. [23] used fiber tape augmentation with semitendinous allograft in the management of AC joint dislocations. K.P. Solanki et al. [24] used fiber tape in 2020 for the treatment of lateral end clavicle fractures, showing a 100 % union rate and excellent clinical outcomes with minimal complications.
We used the UCLA scoring system to assess functional outcomes in operated patients at three and six months postoperatively. We observed an improvement in the UCLA average score from 33.10 at three months to 35 at six months, which is considered an excellent score. This improvement in the UCLA score was statistically significant ( p -value = 0.001). A. Joukainen et al. [25] used the UCLA scoring system to evaluate functional outcomes in the treatment of AC joint dislocation. Similarly, G. Wang et al. [14] used the UCLA scoring system to assess functional outcomes, including clinical and radiological recovery, following coracoclavicular and acromioclavicular ligament reconstruction using an allogenic tendon graft. Their study reported excellent outcomes for acute AC dislocation.
In our study, the radiological evaluation during follow-up confirmed 100 % reduction and convergence at six months. No donor site morbidity was reported. However, DVT was observed in one patient that was managed conservatively.
The advantages of this technique include short surgery time, small incisions, fast recovery, cost-effectiveness, and ease of reproducibility. It is also easy to tie the knot without assistance, and the knot automatically tightens. Additionally, the deforming forces from the trapezius muscle contribute to further tightening of the knot, preventing upward displacement of the clavicle.
The limitations of this study include its non-comparative design and a small sample size. Therefore, more extensive, multicenter, and comparative studies are needed to draw definitive conclusions.
CONCLUSION
Surgical fixation of Rockwood type III–VI AC joint dislocations and lateral end clavicle fractures with using a special fiber tape knot is a viable option with excellent outcomes. Overall, this surgical technique is cost-effective for the treatment of both AC joint dislocation and lateral end clavicle fractures.
Conflicts interests There are no conflicts of interest.
Funding None.
Ethics approval and consent to participate Ethics committee approval was taken from institutional ethics board.
Consent for publication Consent was taken from all the participants.
Availability of data and materials The datasets used in and/or analyzed in the current study are available from the corresponding author upon reasonable request.
